Download presentation
Presentation is loading. Please wait.

1
Mrs. Ashley Medical Assistant Science

3
PANCREAS ANATOMY stomach esophagus ductus choledocus duodenum duct of Santorini duct of Wirsung pancreas

4
Exocrine and endocrine cells 90% of pancreas related to exocrine (digestive function) 10% endocrine (homeostasis for glucose levels in the body)
 10% endocrine (homeostasis for glucose levels in the body)")
5
5

6
◦ Both an exocrine and endocrine organ ◦ Cells with exocrine function release an alkaline fluid containing sodium bicarbonate and enzymes → pancreatic duct → small intestine ◦ Pancreatic “juice” aids in breakdown and digestion of food in the small intestine ◦ Pancreatic exocrine cells = acinar cells

7
Acinar cells - exocrine cells of the pancreas that produce and transport digestive enzymes Amylase, lipase, phospholipase, proteases (trypsinogen, chymotrypsinogen)
")
8
PANCREATIC SECRETIONS 1. PROTEASES (70%) Endopeptidases (trypsin, chymotrypsin, elastases) Exopeptidases (carboxypeptidases) trypsinogen trypsin activates all other precursors enterokinase (duct walls) 2. NUCLEASES (DNAase, RNAase) 3. PANCREATIC AMYLASE (hydrolyse starch and gl;ycogen) 4. PANCREATIC LIPASE (triglycerides fatty acids and glycerol)
 Endopeptidases (trypsin, chymotrypsin, elastases) Exopeptidases (carboxypeptidases) trypsinogen trypsin activates all other precursors enterokinase (duct walls) 2. NUCLEASES (DNAase, RNAase) 3. PANCREATIC AMYLASE (hydrolyse starch and gl;ycogen) 4. PANCREATIC LIPASE (triglycerides fatty acids and glycerol).")
9
PANCREAS (PANORAMIC) pancreatic acini islet of Langerhans islet of Langerhans BV pancreatic lobe
 pancreatic acini islet of Langerhans islet of Langerhans BV pancreatic lobe")
10
Islets of Langerhans - endocrine cells of the pancreas that produce and secrete hormones into the bloodstream Glucagon - Alpha cells (A cells) - raises the level of glucose (sugar) in the blood by causing liver to break down stored glycogen Insulin - Beta cells (B cells) - stimulates cells to use glucose and reduce glucose levels in blood Antagonistic Hormones
 - raises the level of glucose (sugar) in the blood by causing liver to break down stored glycogen Insulin - Beta cells (B cells) - stimulates cells to use glucose and reduce glucose levels in blood Antagonistic Hormones")
11
11 Endocrine Function : Cells of the Islet of Langerhans synthesize and release hormones into the circulation. Hormones travel through the bloodstream to target tissues (especially liver and muscle) At the target cells, hormones bind specific receptors and cause cell changes that control metabolism
 At the target cells, hormones bind specific receptors and cause cell changes that control metabolism.")
12
12

13
13 Chemically – high levels of glucose and amino acids in the blood Hormonally – beta cells are sensitive to several hormones that may inhibit or cause insulin secretion Neurally – stimulation of the parasympathetic nervous system causes insulin to be secreted.

14
14 Transported through the blood to target tissues where it binds to specific receptors The binding of insulin to target cells: ◦ Acts as a biochemical signal to the inside of the cell Overall, cell metabolism is stimulated There is increased glucose uptake into the cell Regulation of glucose breakdown within the cell Regulation of protein and lipid breakdown within the cell

15
Blood glucose is decreased because insulin causes glucose to leave the bloodstream and enter the metabolizing cells. With the exception of brain, liver and erythrocytes, tissues require membrane glucose carriers.

16
Inflammation of the pancreas

17
Pancreas suddenly becomes inflamed Causes: Gallstones Ethanol Trauma Steroids Mumps Autoimmune Scorpion venom Hyperlipidaemia, hypothermia ↑Ca 2+ Drugs

18
Symptoms epigastric and central abdominal pain vomiting and nausea swollen and tender abdomen fever dehydration and low blood pressure Diagnosis medical history and physical exam blood test: ↑ amylase, lipase abdominal ultrasound, Endoscopic Ultrasound, CT scan

19
Treatment nothing to eat or drink intravenous fluids analgesia ERCP and gallstone removal Complications shock, Acute respiratory distress syndrome, renal failure, Disseminated intravascular coagulation, sepsis, ↓Ca 2+ pancreatic necrosis, pseudocyst, abscesses, bleeding, thrombosis

20
inflammation of the pancreas - gets worse over time and leads to permanent damage Causes: many years of alcohol use hereditary disorders of the pancreas cystic fibrosis haemochromatosis autoimmune conditions

21
Symptoms nausea and vomiting weight loss diarrhea steatorrhea

22
Treatment drugs - analgesia, lipase, fat-soluble vitamins diet surgery – pancreatectomy pancreaticojejunostomy Complications pseudocyst, diabetes, biliary obstruction, local arterial aneurysm, splenic vein thrombosis

24
The single most common endocrine disorder – group of glucose intolerance disorders Incidence is estimated at 8.3% of the North American population 35% are pre-diabetic Many of these cases are undiagnosed

25
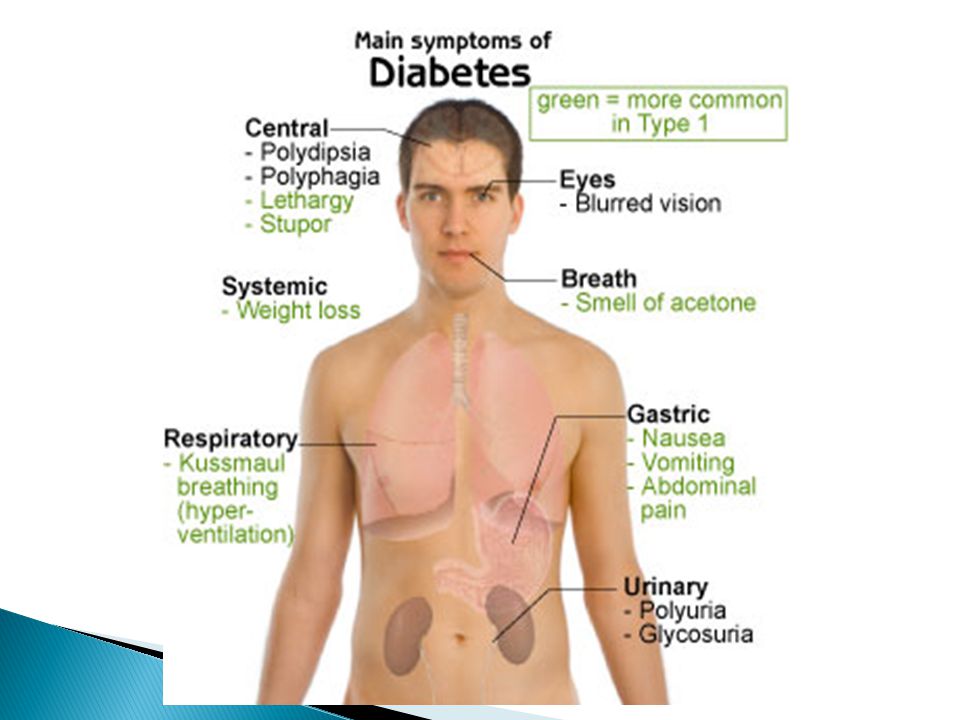
25 Historically ‑ distinguished by weight loss, excessive urination, thirst, hunger Excessive urination = polyuria Excessive thirst = polydipsia Excessive hunger = polyphagia Modern characterization is by hyperglycemia and other metabolic disorders

26
increased level of glucose in the blood (normal blood glucose level 3.5-6.0 mmol/l) 90 mg/100ml Type 1 ( insulin-dependent DM, IDDM) destruction of insulin-secreting pancreatic β cells (autoimmune response) juvenile diabetes-tends to begin in early childhood patient always needs insulin
 90 mg/100ml Type 1 ( insulin-dependent DM, IDDM) destruction of insulin-secreting pancreatic β cells (autoimmune response) juvenile diabetes-tends to begin in early childhood patient always needs insulin")
27
Type 2 (non-insulin dependent DM, NIDDM) insulin resistance Β cell dysfunction, ↓insulin secretion Causes of insulin resistance: metabolic syndrome (central obesity, hyperglycaemia, hypertension, ↓HDL cholesterol, ↑triglycerides) renal failure pregnancy cystic fibrosis polycystic ovarian syndrome
 insulin resistance Β cell dysfunction, ↓insulin secretion Causes of insulin resistance: metabolic syndrome (central obesity, hyperglycaemia, hypertension, ↓HDL cholesterol, ↑triglycerides) renal failure pregnancy cystic fibrosis polycystic ovarian syndrome")
28
28 Glucose in urine- Because when insulin is not present, glucose is not taken up out of the blood at the target cells. So blood glucose is very highly increased → increased glucose filtered and excreted in the urine (exceeds transport maximum)
.")
29
Mechanisms of insulin resistance: post-receptor defects in insulin action gene mutation circulating autoantibodies

31
Diagnosis blood glucose level urine sample HbA1c test

32
Treatment: diet oral hypoglycaemics

33
33 Control diet Carbohydrates should make up about 55-60% of patient’s total calories Fats should make up <30% of patient’s total calories Proteins should make up about 15-20% of patient’s total calories

34
34 Monitor exercise Remember: muscles are a target tissue of insulin, and metabolize much glucose for energy Sometimes exercise → irregular blood glucose levels So diabetic patients should be monitored when they are exercising

35
insulin injections (long-acting, short- acting, rapid-acting) insulin pen insulin pump therapy
 insulin pen insulin pump therapy")
36
Complications

37
diabetec ketoacidosis hypoglycaemia diabetic retinopathy

38
atherosclerosis (heart disease and stroke) neuropathy (diabetic foot care)
 neuropathy (diabetic foot care)")
39
Age over 40 years Diabetes during a previous pregnancy Excess body weight Family history of diabetes Dyslipidaemia (large amount of lipids in body) Hypertension Low activity level Metabolic syndrome Polycystic ovarian syndrome Acanthosis nigricans- darkening and thickening of skin
 Hypertension Low activity level Metabolic syndrome Polycystic ovarian syndrome Acanthosis nigricans- darkening and thickening of skin")
Similar presentations







![Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]](/15/4663650/big_thumb.jpg "Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]>")




 muscle proteins liver glycogen fat lipids glucose.>")
 muscle proteins liver glycogen fat lipids glucose.>")



 state>")
 into small molecules. Allows absorption of nutrients (ions and.>")

>")
