Download presentation
Presentation is loading. Please wait.

1
Insulin, Glucagon & Diabetes mellitus ENDOCRINE HORMONE

8
Islet

11
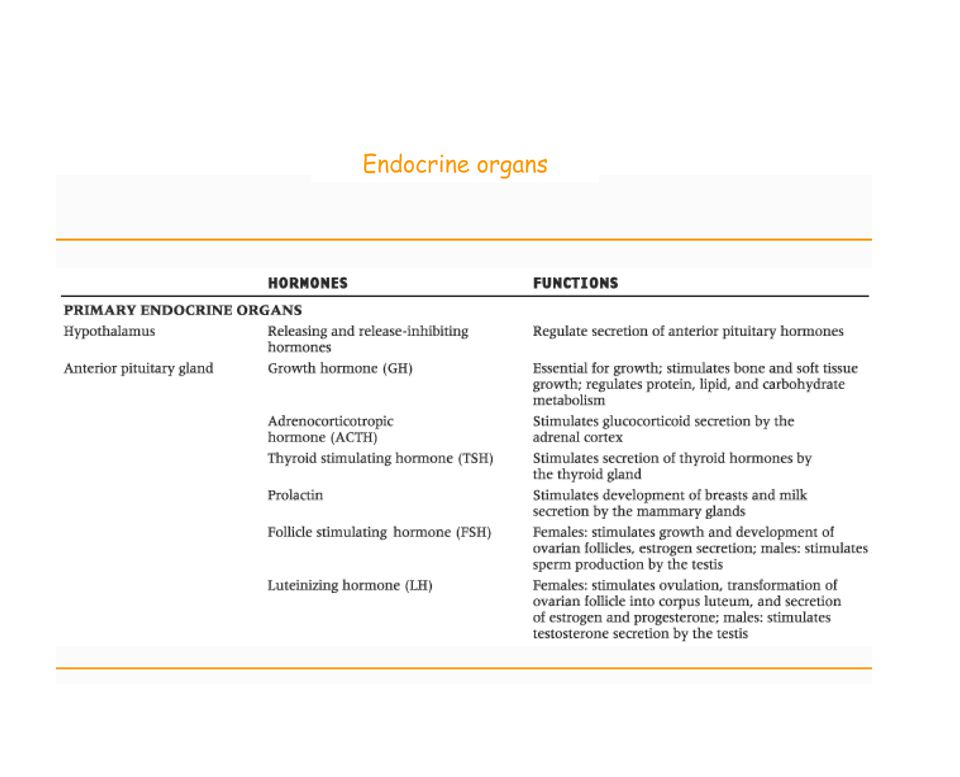
Pancreas Insulin secretagogue Sulphonylureas Meglitinides, GLP-1 Pancreas – 3 types of cells 1.a cell (5-10%) – secrete glucagon 2.b cells (70-80%) – secrete insulin 3.d cells (5%) – secrete somatostatin cells cell
 – secrete glucagon 2.b cells (70-80%) – secrete insulin 3.d cells (5%) – secrete somatostatin cells cell")
12
Diabetes Diabetes mellitus is a heterogeneous group of metabolic disorders characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. (American Diabetes Association 2001) Defective Insulin secretion Defective Insulin action Absolute insulin Diabetes
 Defective Insulin secretion Defective Insulin action Absolute insulin Diabetes.")
13
Symptoms of Diabetes 1.Polydipsia (Excessive thirst, dry mouth) 2.Polyuria (excessive urination) 3.Tiredness, fatigue, irritability 4.Recent change in weight. 5.Polyphagia (increased food consumption) 6.Blurring of vision 7.Nausea, headache
 6.Blurring of vision 7.Nausea, headache.")
14
Complication of Diabetes 1.Macrovascular complication - Coronary and peripheral vascular disease - hypertension 2. Microvascular complication - Retinopathy with potential blindness - Neuropathies with risk of foot ulcer, amputation. - Nephropathy that may lead to renal failure. - Reduce resistance to infection Diabetes is a complex heterogeneous disease where multiple levels of abnormalities are present in various tissues. Defects of diabetes mellitus include long-term damage, dysfunction and failure of various organs. The major long-term complications of diabetes mellitus are macrovascular and microvascular diseases such as nephropathy, retinopathy and neuropathy

15
Diabetes - classification 1.Type 1 (IDDM) 2.Type 2 (NIDDM) 3.MODY (Maturity-onset diabetes) 4.Gestational diabetes
 2.Type 2 (NIDDM) 3.MODY (Maturity-onset diabetes) 4.Gestational diabetes")
16
Type 1 diabetes Type 1 diabetes is defined by an absolute requirement of exogenous insulin results from the autoimmune destruction of insulin-secreting pancreatic B c ells. Type 1 diabetes prone to ketoacidosis and exogenous insulin is required to prevent ketosis. Type 2 diabetes Type 2 diabetes is characterized by a relative insulin deficiency due to insulin secretory defect with insulin resistance. Ketoacidosis is absent. Common risk factors: obesity, genetics.

17
Etiology/causes of Diabetes Type 2 Diabetes Obesity Insulin resistance Genetic factors (family history of diabetes) Type 1 Diabetes The common causes of type 1 diabetes (90% cases) is autoimmune destruction of B cells. Environmental factors (virus and dietary component Genetic factors (HLA antigen) Autoimmune destruction of B cell HLA, Human leukocyte antigen
 Autoimmune destruction of B cell HLA, Human leukocyte antigen.")
18
Important feature of type 1 and type 2 diabetes Clinical & other features Type 1Type 2 Age of onsetUsually <30Usually >40 WeightNon-obeseUsually obese KetosisCommonRare Plasma glucose levelHigh Mild to moderate Islet cell mass Severely reduced Moderately reduced AutoantibodiesPresentAbsent Family history of diabetes UncommonCommon

19
Mechanism of insulin secretion Insulin

20
AA, arachadonic acid; AC, adenylyl cyclase; Ach, acetylcholine; CaM PK, calmodulin-dependent kinase; CCK, cholecystokinin; DAG, diacylglycerol; GK, glucokinase; GIP, gastric inhibitory polypeptide; G p, G protein; IP 3, inositol 1,4,5-triphosphate; PKA, protein kinase A; PKC, protein kinase C; PLA 2, phospholipase A 2 ; PLC, phospholipase C.

21
M/A of Sulphonylurea

22
GLP, GIP 5-AMP PDE Insulin release

23
Ach, CCK Insulin secretion Ca 2+ RX871024 + Imidazoline compd (RX871024) DAG level & activates PKC Troglitazone
 DAG level & activates PKC Troglitazone")
24
Diabetes therapy The goal of diabetes management is to achieve as near normoglycemia as in practicable. 1.Diet 2.Insulin 3.Oral hypoglycemic agents (sulphonylyurea or biguanide)
.")
25
1. Sulphonylurea ( insulin secretagogue) First generation tolbutamide tolazamide acetohexamide Second generation glibenclamide glipizide gliclazide 2. Biguanide metformin phenformin buformin 3. a-glucosidase inhibitors acarbose ibitor 4. Thiazolidinediones (insulin sensitizers) troglitazone pioglitazone rosiglitazone 5. Meglitinides ( insulin secretagogue) repaglinide Drugs in pipeline Ö glucagon-like-peptide 1 (GLP- 1) and analogues Ögastric inhibitory polypeptide (GIP) and analogues Ö Amylin Antidiabetic drugs
 First generation tolbutamide tolazamide acetohexamide Second generation glibenclamide glipizide gliclazide 2. Biguanide metformin phenformin buformin 3. a-glucosidase inhibitors acarbose ibitor 4. Thiazolidinediones (insulin sensitizers) troglitazone pioglitazone rosiglitazone 5. Meglitinides ( insulin secretagogue) repaglinide Drugs in pipeline Ö glucagon-like-peptide 1 (GLP- 1) and analogues Ögastric inhibitory polypeptide (GIP) and analogues Ö Amylin Antidiabetic drugs.")
26
Principal modes and sites of action of antidiabetic drugs Liver glucose output Metformin Thiazolinediones Pancreas Insulin secretion Sulphonylureas Meglitinides, GLP-1 Gut Delayed glucose absorption a-glucosidase inhibitors (eg. Acarbose) Metformin, GLP-1 Muscle & Adipose tissue Peripheral glucose uptake Metformin Insulin sensitivity Thiazolidinediones, Amylin
 Metformin, GLP-1 Muscle & Adipose tissue Peripheral glucose uptake Metformin Insulin sensitivity Thiazolidinediones, Amylin.")
27
Antidiabetic drugs: main modes of action DrugMain actions Insulin HGO peripheral glucose utilization Sulphonylureas Insulin release Metformin * Insulin resistance Acarbose § Rate of carbohydrate digestion Troglitazone Actions of insulin Repaglinide Postprandial insulin release * Biguanide; § glucosidase inhibitor, thiazolidinedione; non-sulfonylurea insulin release. HGO, hepatic glucose output.

28
M/A of Sulphonylurea Sulpholylurea

29
GLP, GIP 5-AMP PDE Insulin release IBMX Piperazine GLP-1 receptor agonist : Extendin (newer drug) Extendin
 Extendin")
30
Ach, CCK Insulin secretion Ca 2+ RX871024 + Imidazoline compd (RX871024) DAG level & activates PKC Troglitazone
 DAG level & activates PKC Troglitazone")
Similar presentations






![Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]](/15/4663650/big_thumb.jpg "Islets of Langerhan. Prof. K. Sivapalan. 08-01-14Islets of Langerhan2 Histology. A cells 20 % [glucogon] B cells 50% [Insulin] D cells 8% [somatostatin]>")





 muscle proteins liver glycogen fat lipids glucose.>")









 Diabetes Mellitus.>")
