Download presentation
Presentation is loading. Please wait.

1
Deep space infections of the neck and floor of mouth
Dr David Maritz

2
Introduction Penicillin 1940’s Odontogenic infections Deep anatomic fascial space Threaten vital structures

4
Clinical examination underestimate extent in 70%
Introduction Most important: Submandibular Lateral Pharyngeal Retropharyngeal / Danger / Prevertebral Clinical examination underestimate extent in 70%

5
Potential pathways of extension of deep fascial space infections of the head and neck

7
Fascial spaces around the mouth and face

8
Figure 69-4 Natural progression of dental infection
Figure 69-4 Natural progression of dental infection. The pathways by which such infections may travel are: 1, postzygomatic (from canine fossa in cuspid and bicuspid region; pterygomaxillary fossa communicates from rear); 2, vestibular; 3, facial; 4, submandibular; 5, sublingual; 6, palatal; 7, antral; 8, pterygomandibular; 9, parapharyngeal; 10, masseteric. (Redrawn from Rose LF, Hendler BH, Amsterdam JT: Temporomandibular disorders and odontic infections. Consultant 22:125, 1982.) Downloaded from: Rosen's Emergency Medicine (on 15 January :57 PM) © 2007 Elsevier
; 2, vestibular; 3, facial; 4, submandibular; 5, sublingual; 6, palatal; 7, antral; 8, pterygomandibular; 9, parapharyngeal; 10, masseteric. (Redrawn from Rose LF, Hendler BH, Amsterdam JT: Temporomandibular disorders and odontic infections. Consultant 22:125, 1982.) Downloaded from: Rosen s Emergency Medicine (on 15 January :57 PM) © 2007 Elsevier.")
9
Clinical examination of odontogenic infections

10
Stages of infection 4 stages Inoculation Cellulitis Abscess Rupture Spreading odontogenic infection

11
Trismus Inability to open mouth widely Inflammation muscles of mastication Masticator space / Pterygomandibular space Difficult intubation

12
Airway / Physical evaluation
Pharyngeal swelling – difficulty swallowing Difficulty sleeping supine Sniffing position – Retropharyngeal space Head deviated to opposite side – Lateral pharyngeal space Muffled voice – Epiglottitis Distant quality to voice – Retropharyngeal / Lateral Pharyngeal Elevated tongue – Sublingual space

14
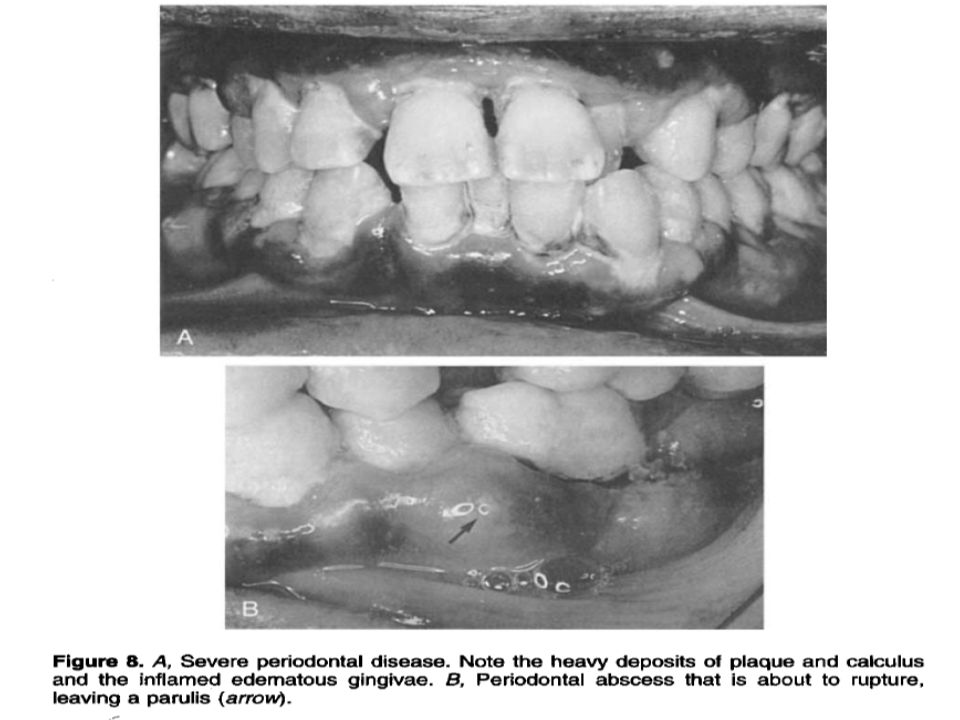
Intraoral examination
Caries Swellings of oral vestibule Periodontal disease Tooth mobility Pericoronitis Swellings Position of uvula

17
Radiographic evaluation
Rapid CT scanners Contrast enhanced CT Postero-anterior / lateral soft tissue x-rays of neck Dental panoramic view (Orthopantomogram)
")
18
Lateral radiograph of the neck

20
Figure 69-5 Periapical abscesses (arrows) as seen on Panorex film.
Downloaded from: Rosen's Emergency Medicine (on 15 January :07 PM) © 2007 Elsevier
 © 2007 Elsevier.")
21
Culture and sensitivity testing
Penicillin resistance 30 – 50%

23
1. Submandibular Space

24
Introduction ‘’Ludwigs angina’’ ‘’Angina maligna’’ ‘’Morbus strangulatorius’’ ‘’Garotillo’’

25
Early appearance of patient who has Ludwig’s angina with characteristic submandibular ‘’woody’’ swelling

27
Anatomy and pathogenesis
Sublingual and submylohyoid spaces Odontogenic ( periapical abscesses of mandibular molars – 2nd / 3rd) Communicate freely: Entire submandibular space Buccopharyngeal gap – lateral pharyngeal space – retropharyngeal space
 Communicate freely: Entire submandibular space. Buccopharyngeal gap – lateral pharyngeal space – retropharyngeal space.")
28
Anatomic relationships in submandibular infections

29
Routes of spread of odontogenic orofacial infections along planes of least resistance

30
Clinical manifestations
Mouth pain / stiff neck / drooling / dysphagia No trismus Woody inflammation No lymph node involvement Protruding tongue

31
Ludwig's Angina Involvement submandibular spaces bilaterally and submental space in midline Rapid spread to lateral pharyngeal / retropharyngeal space Rapidly obstruct upper airway

32
Early Ludwig's angina

33
Early Ludwig's angina

34
Submandibular space abscess and Cellulitis

35
Potential complications
Airway compromise Spread into the lateral pharyngeal space and beyond

36
Figure 69-6 Extensive spread of infection of odontogenic origin involving masseteric, sublingual, submental, and submandibular spaces with extension to mediastinum. A, Preoperative. B, Postoperative. Note drainage from mediastinum. (From Guernsey LH: Practical problem solving in oral surgery. In Cohen DW [ed]: Continuing Dental Education, vol 2, suppl 10. Philadelphia, University of Pennsylvania School of Dental Medicine, 1979.) Downloaded from: Rosen's Emergency Medicine (on 15 January :09 PM) © 2007 Elsevier
![Figure 69-6 Extensive spread of infection of odontogenic origin involving masseteric, sublingual, submental, and submandibular spaces with extension to mediastinum. A, Preoperative. B, Postoperative. Note drainage from mediastinum. (From Guernsey LH: Practical problem solving in oral surgery. In Cohen DW [ed]: Continuing Dental Education, vol 2, suppl 10. Philadelphia, University of Pennsylvania School of Dental Medicine, 1979.)](http://slideplayer.com/slide/4555813/15/images/36/Figure+69-6+Extensive+spread+of+infection+of+odontogenic+origin+involving+masseteric%2C+sublingual%2C+submental%2C+and+submandibular+spaces+with+extension+to+mediastinum.+A%2C+Preoperative.+B%2C+Postoperative.+Note+drainage+from+mediastinum.+%28From+Guernsey+LH%3A+Practical+problem+solving+in+oral+surgery.+In+Cohen+DW+%5Bed%5D%3A+Continuing+Dental+Education%2C+vol+2%2C+suppl+10.+Philadelphia%2C+University+of+Pennsylvania+School+of+Dental+Medicine%2C+1979.%29.jpg "Downloaded from: Rosen s Emergency Medicine (on 15 January :09 PM) © 2007 Elsevier.")
37
Figure 69-6 Extensive spread of infection of odontogenic origin involving masseteric, sublingual, submental, and submandibular spaces with extension to mediastinum. A, Preoperative. B, Postoperative. Note drainage from mediastinum. (From Guernsey LH: Practical problem solving in oral surgery. In Cohen DW [ed]: Continuing Dental Education, vol 2, suppl 10. Philadelphia, University of Pennsylvania School of Dental Medicine, 1979.) Downloaded from: Rosen's Emergency Medicine (on 15 January :07 PM) © 2007 Elsevier
![Figure 69-6 Extensive spread of infection of odontogenic origin involving masseteric, sublingual, submental, and submandibular spaces with extension to mediastinum. A, Preoperative. B, Postoperative. Note drainage from mediastinum. (From Guernsey LH: Practical problem solving in oral surgery. In Cohen DW [ed]: Continuing Dental Education, vol 2, suppl 10. Philadelphia, University of Pennsylvania School of Dental Medicine, 1979.)](http://slideplayer.com/slide/4555813/15/images/37/Figure+69-6+Extensive+spread+of+infection+of+odontogenic+origin+involving+masseteric%2C+sublingual%2C+submental%2C+and+submandibular+spaces+with+extension+to+mediastinum.+A%2C+Preoperative.+B%2C+Postoperative.+Note+drainage+from+mediastinum.+%28From+Guernsey+LH%3A+Practical+problem+solving+in+oral+surgery.+In+Cohen+DW+%5Bed%5D%3A+Continuing+Dental+Education%2C+vol+2%2C+suppl+10.+Philadelphia%2C+University+of+Pennsylvania+School+of+Dental+Medicine%2C+1979.%29.jpg "Downloaded from: Rosen s Emergency Medicine (on 15 January :07 PM) © 2007 Elsevier.")
38
Therapeutic considerations
Mixed infection – synergistic interaction Immunocompromised MRSA Candida / Aspergillus

39
2. Lateral Pharyngeal Space

40
Potential pathways of extension of deep fascial space infections of the head and neck

42
Anatomy and pathogenesis
Anterior / muscular compartment Posterior / neurovascular compartment Carotid sheath 9 to 12 cranial nerves Sympathetic trunk Peritonsillar abscesses

43
Clinical manifestations
Anterior compartment Dysphagia Trismus pain Posterior compartment No trismus Neurologic / vascular Edema epiglottis / larynx

45
Abscess of lateral Pharyngeal space

47
Potential complications
NB: Posterior compartment Laryngeal edema Vagal nerve Horner's syndrome Cranial nerve palsies Suppurative jugular thrombophlebitis (lemierre syndrome) Carotid artery erosion
 Carotid artery erosion.")
48
Lemierre’s Syndrome Septic thrombophlebitis of internal jugular vein Septic emboli – lung / liver abscesses / septic arthritis Fusobacterium necrophorum

49
Jugular venous thrombosis

50
Therapeutic considerations
Suppurative Posterior more conservative Anterior more aggressive treatment

51
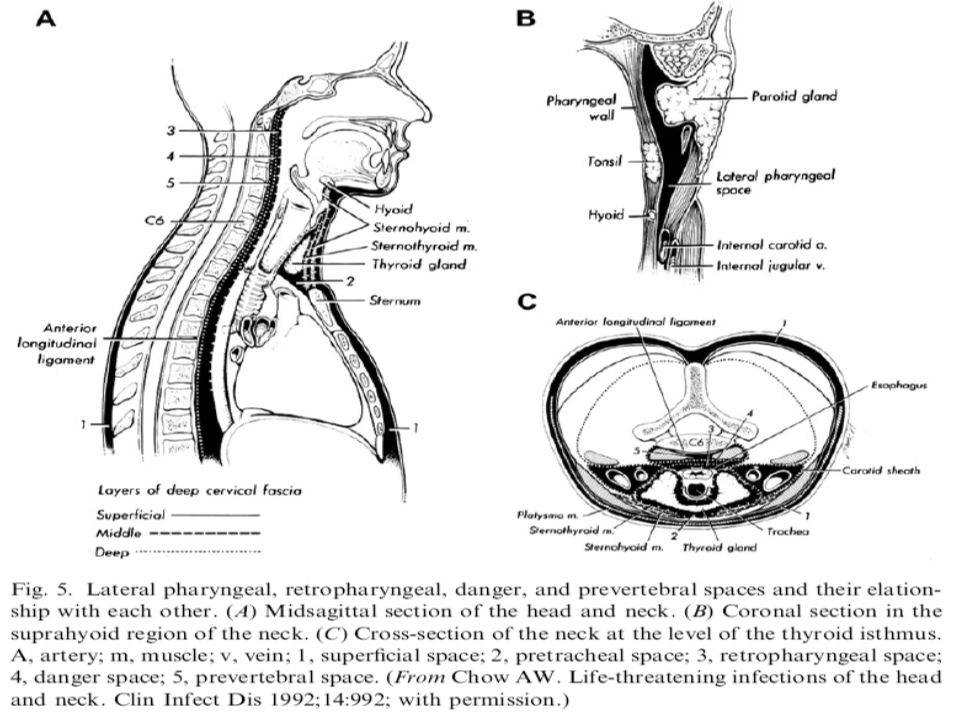
3. Retropharyngeal / Prevertebral / Danger Space

52
Introduction Caudal extension of infection Considered together

53
Anatomy and pathogenesis
Between pharynx-esophagus and spine Delineated by fascial planes: 3 layers of deep cervical fascia

55
Retropharyngeal space
Base skull to C7 / T1 Mediastinal spread Pleural / pericardial spread Deep cervical chain of nodes in children Other causes eg: oesophageal instrumentation, foreign bodies….

56
Retropharyngeal abscess

57
Retropharyngeal space

59
Danger space Base skull to diaphragm Contiguous spread from adjacent spaces

60
Prevertebral space Between prevertebral fascia and vertebral bodies Base skull to coccyx Contiguous with psoas muscle sheath Haematogenous spread NB Local instrumentation Contiguous spread Different microbiology

61
Clinical manifestations Retropharyngeal danger space
Sore throat / dysphagia / stiff neck Upper airways obstruction Head tilt contralateral side Pleuritic chest pain Bulging posterior oropharynx

62
Lateral radiograph of the neck

63
Prevertebral space Spinal cord compression Epidural abscess

64
Potential complications
Laryngeal inflammation Rupture with aspiration Descending necrotizing mediastinitis Pyothorax / pericardial involvement Spinal epidural collections Psoas muscle infection

65
Therapeutic considerations
Retropharyngeal / danger space: Adequate anaerobic / oral gram + cover Surgery if indicated Prevertebral: Surgical drainage NB gram + / MRSA / gram - rods

66
4. Buccal space Subcutaneous space
Connects to: infraorbital space, periorbital tissues, superficial temporal space Hemophilus influenzae Cellulitis: Children Recent URTI / sinusitis

69
Buccal Cellulitis (Hib)
")
70
5. Infraorbital space Lower lid / periorbital swelling
Point medially (inner canthus) or laterally (lateral canthus) Septic thrombophlebitis angular vein → cavernous sinus
 or laterally (lateral canthus) Septic thrombophlebitis angular vein → cavernous sinus.")
71
6. Orbital space Preseptal Cellulitis
Subperiosteal abscess (orbital wall) Orbital Cellulitis / abscess → optic nerve damage / cavernous sinus thrombosis
 Orbital Cellulitis / abscess → optic nerve damage / cavernous sinus thrombosis.")
75
7. Vestibular space Diffuse facial swelling
Elevation of the oral vestibule Potential space between oral mucosa and muscles facial expression Draining sinus

77
8. Subperiosteal space Dental infection
Perforates cortical layer but not periosteum Eg: mandibular subperiosteal infection

78
9. Submental space Secondary spread from submandibular space

80
10. Masticator space Severe trismus Surrounding muscles of mastication

82
Masticator space infection with trismus

83
Masticator space abscess

84
11. Temporal space Trismus (infratemporal fossa – part of masticator space) Cavernous sinus thrombosis
 Cavernous sinus thrombosis.")
85
Deep temporal space infection with spread to parotid space

87
Treatment

88
The admission decision
Airway issues High fever Dehydration Need for I+D Inpatient control systemic disease Immune compromise

89
Airway security Protect against aspiration ETT ruptures abscess Trismus / Swelling Maintain airway reflexes during intubation

90
Surgical treatment Gravity dependent surgical drainage Antibiotics secondary Tooth extraction

91
Antibiotic therapy Predominately anaerobic nature Initially: aerobic streptococci ( penicillin ) Later: anaerobic bacteria ( penicillin resistant ) Synergistic interaction
 Synergistic interaction.")
94
Complications

95
Mediastinitis Airway security Contrast CT Open thoracotomy Broad spectrum antibiotics

96
Cavernous sinus thrombosis
Ascending septic thrombophlebitis Anterior route – angular vein (infraorbital space) Posterior route – facial vein (buccal space) Congestion retinal veins CN 6 paresis → ophthalmoplegia / blindness Severe orbital / periorbital / infraorbital swelling
 Posterior route – facial vein (buccal space) Congestion retinal veins. CN 6 paresis → ophthalmoplegia / blindness. Severe orbital / periorbital / infraorbital swelling.")
97
Cavernous Sinus Thrombosis
Treatment: Tooth extraction root canal Drainage deep spaces High dose IV antibiotics Anticoagulation

100
Summary Preventative dental care Effective antibiotics

Similar presentations