Download presentation
Presentation is loading. Please wait.

1
Vaginitis and PID – The Basics Wanda Ronner, M.D.

2
Vaginitis Disruption in the normal vaginal ecosystem Alteration of vaginal pH A decrease in lactobacilli Growth of other bacteria

3
Normal physiologic discharge Cervical mucus Endometrial fluid Fluid from Skene’s and Bartholin’s glands Exfoliated squamous cells Normal pH: 3.5 – 4.5 during reproductive years; 6 – 8 after menopause

4
Common Causes of Vaginitis Bacterial Vaginosis: 15 - 50% of cases; all ages; anaerobic bacteria and Gardnerella vaginalis Trichomonas: 15 - 20% of cases; 20- 45years; protozoan Trichomonas vaginalis Candida: 33% of cases; premenopausal women: 90% caused by Candida albicans

6
Common Treatments Yeast: oral fluconazole 150mg single dose, or clotrimazole, miconazole, or terconazole. Trichomonas: oral metronidazole 2 grams in a single dose or 500mg bid for 7 days. Bacterial Vaginosis: oral metronidazole 500mg bid for 7 days, or vaginal clindamycin cream or metronidazole gel.

7
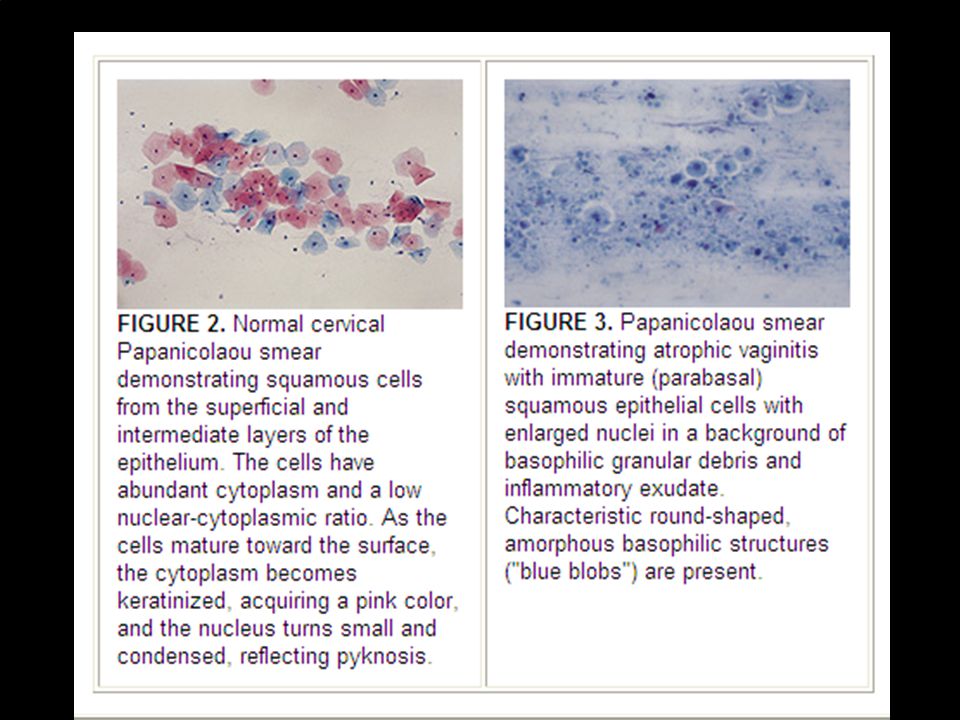
Atrophic Vaginitis 40% of postmenopausal women Caused by estrogen deficiency Symptoms: dryness, itching, burning, dyspareunia, pelvic pressure, yellowish- green malodorous discharge Findings: pH > 5, decreased superficial cells, WBCs Treatment: vaginal or oral estrogen

8
67 yr. old with vulvar/vaginal atrophy

10
Pelvic Inflammatory Disease Inflammatory disorders of the upper female genital tract – endometritis, salpingitis, tubo-ovarian abscess, pelvic peritonitis Organisms responsible: mainly Gonorrhea and Chlamydia; anaerobes, G. vaginalis, Haemophilus, enteric Gram-negative rods, Streptococcus agalactiae.

11
PID – a public health concern Most common gyn reason for ER visits: 350,000/year. 70,000 hospitalizations/year. Most common serious infection of women age 16 – 25. One in four women have significant medical or reproductive complications.

12
Diagnosis of PID Cervical motion tenderness Uterine tenderness Adnexal tenderness Temp > 101º F Mucopurulent discharge Abundant WBCs on wet mount Elevated ESR, elevated C-reactive protein GC or Chlamydia

13
Differential Diagnosis Ectopic pregnancy Acute appendicitis Functional pain (e.g. pain with ovulation) Dysmenorrhea Endometriosis UTI/Pyelonephritis Bowel disorders
 Dysmenorrhea Endometriosis UTI/Pyelonephritis Bowel disorders.")
14
Treatment of PID Need to provide empiric, broad spectrum coverage of likely pathogens Must include treatment for GC and Chlamydia See handout for April 2007 CDC treatment regimens

15
CDC Recommended Regimens Parenteral: Cefotetan (2g IV every 6 hrs) OR Cefoxitin (2g IV every 6 hrs) PLUS Doxycycline (100 mg orally or or IV) every 12 hrs. Oral: Ceftriaxone (250mg IM in a single dose) PLUS Doxycycline 100mg orally twice a day for 14 days with or without Metronidazole 500mg orally twice a day for 14 days
 PLUS Doxycycline 100mg orally twice a day for 14 days with or without Metronidazole 500mg orally twice a day for 14 days.")
16
Why do we treat aggressively? Even mild cases may result in severe damage: infertility, ectopic pregnancy, and chronic pelvic pain.

17
Follow Up Improvement should be seen within 3 days on oral meds – defervescence, reduction in abdominal tenderness, uterine, adnexal and cervical motion tenderness – if not – HOSPITALIZE In no improvement after 3 days on parenteral meds consider laparoscopy

Similar presentations


>")





 as PID is an infection that affects a woman’s reproductive.>")
>")

 Study.>")




>")



