Download presentation
Presentation is loading. Please wait.

1
Determining the Incidence of Drug-Associated Acute Kidney Injury in Nursing Home Residents Steven M. Handler, MD, PhD, CMD Assistant Professor of Geriatric Medicine and Biomedical Informatics; CMIO UPMC Community Provider Services.

2
U.S. Nursing Home (NH) Demographics Approximately 1.6 million Americans receive health care in more than 16,000 NHs annually In 2006, national spending on NH care totalled 125 billion dollars or about 5.3% of total U.S. healthcare spending Lifetime risk of NH placement for those over the age of 65 is ~45% The number of people expected to need NH services is expected to double by the year 2020 Hanlon JT, Handler SM, et al. Brocklehurst’s Textbook of Geriatric Medicine & Gerontology. 7th ed. London, UK. Churchill Livingstone (2010).
 Demographics Approximately 1.6 million Americans receive health care in more than 16,000 NHs annually In 2006, national spending on NH care totalled 125 billion dollars or about 5.3% of total U.S. healthcare spending Lifetime risk of NH placement for those over the age of 65 is ~45% The number of people expected to need NH services is expected to double by the year 2020 Hanlon JT, Handler SM, et al. Brocklehurst’s Textbook of Geriatric Medicine & Gerontology. 7th ed. London, UK. Churchill Livingstone (2010)..")
3
PAHs are defined as hospitalizations that could have been avoided because the condition could have been prevented or treated outside of an inpatient hospital setting. 26% percent of hospitalizations were considered PAHs Had an ALOS of 6.1 days and an estimated cost of $8 billion Five conditions were responsible for nearly 80% of PAHs (CHF, COPD/asthma, UTIs, pneumonia, and dehydration/AKI) Potentially Avoidable Hospitalizations (PAHs) Medicare & Medicaid Research Review 2014;4.
 Potentially Avoidable Hospitalizations (PAHs) Medicare & Medicaid Research Review 2014;4..")
4
Public Health Significance of Adverse Drug Events (ADEs) in Nursing Homes Are the most frequent medication-related adverse event, with ~2 million ADEs/year when all U.S. NHs are combined Handler SM, et al. Am J Geriatr Pharmacother 2006; 4:264-72 Are the most clinically significant medication-related adverse events and are associated with approximately 93,000 deaths/year Gurwitz JH, et al. J Am Geriatr Soc. 2008;56(12):2225-33. Are the most costly medication-related adverse events, resulting in as much as 4 billion dollars of excess healthcare expenditures/year Bootman JL, et al. Arch Intern Med. 1997;157(18):2089-96.
: Are the most costly medication-related adverse events, resulting in as much as 4 billion dollars of excess healthcare expenditures/year Bootman JL, et al. Arch Intern Med. 1997;157(18):")
5
Systems Analysis of ADEs in NHs Only the presence of polypharmacy has consistently been found to increase the likelihood of developing an ADE Leape LL, et al. JAMA 1995;274(1):35-43. Approximately half of the events are considered preventable (i.e., medication errors) Gurwitz JH, et al. Am J Med. 2005;118(3):251-8. Most (80%) are associated with monitoring rather than prescribing errors Gurwitz JH, et al. Am J Med 2000; 109:87-94.
: Approximately half of the events are considered preventable (i.e., medication errors) Gurwitz JH, et al. Am J Med. 2005;118(3): Most (80%) are associated with monitoring rather than prescribing errors Gurwitz JH, et al. Am J Med 2000; 109:")
6
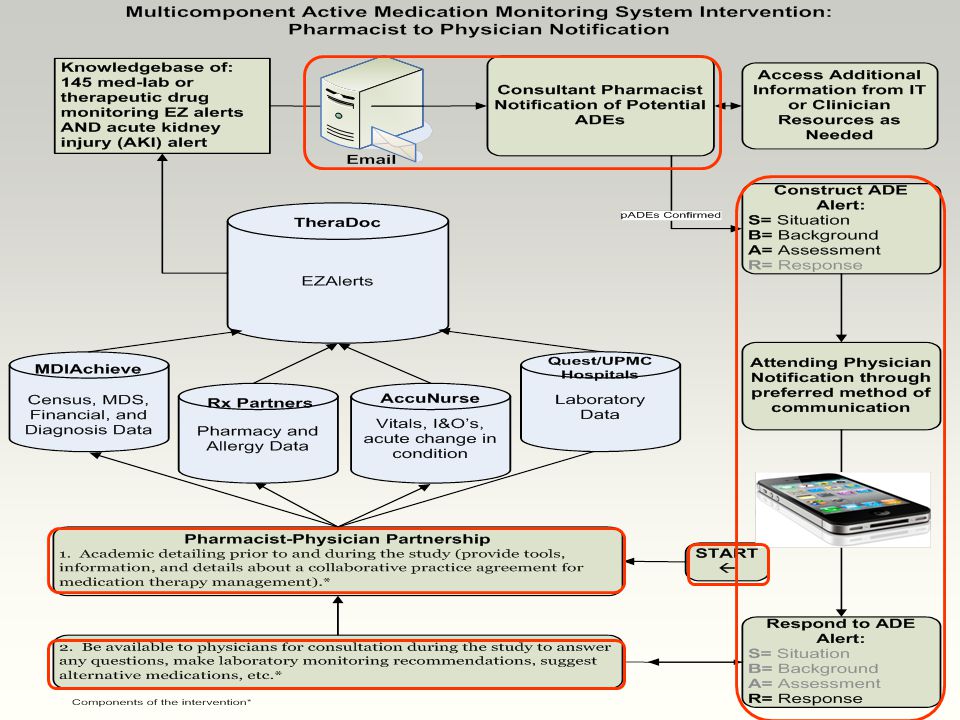
The Institute of Medicine recommends that all health- care settings assess the safety of medication use through active monitoring systems IOM. Preventing Medication Errors. Washington, DC: National Academies Press; 2006. Active medication monitoring systems are particularly needed to detect and prevent ADEs in priority populations such as institutionalized elderly because of: –concerns about the quality of pharmaceutical care, –frequency of polypharmacy, and –an insufficient healthcare workforce with a poorly developed safety culture Handler SM et al. Qual Saf Health Care. 2006 Dec;15(6):400-4. Active Medication Monitoring Systems
: Active Medication Monitoring Systems.")
7
Steinman MA, Handler SM, Gurwitz JH, Schiff GD, Covinsky KE. J Am Geriatr Soc. 2011;59(8):13-20. Impact of Medication Monitoring on ADEs Seriousness
: Impact of Medication Monitoring on ADEs Seriousness.")
8
8

9
Although acute kidney injury (AKI) is well-studied in the acute care setting, investigation of AKI in the nursing home (NH) setting is virtually nonexistent The goal of this study was to determine the incidence of drug-associated AKI using the RIFLE (Risk, Injury, Failure, Loss of kidney function or End-Stage kidney disease) criteria in NH residents Background/Objective
 is well-studied in the acute care setting, investigation of AKI in the nursing home (NH) setting is virtually nonexistent The goal of this study was to determine the incidence of drug-associated AKI using the RIFLE (Risk, Injury, Failure, Loss of kidney function or End-Stage kidney disease) criteria in NH residents Background/Objective")
10
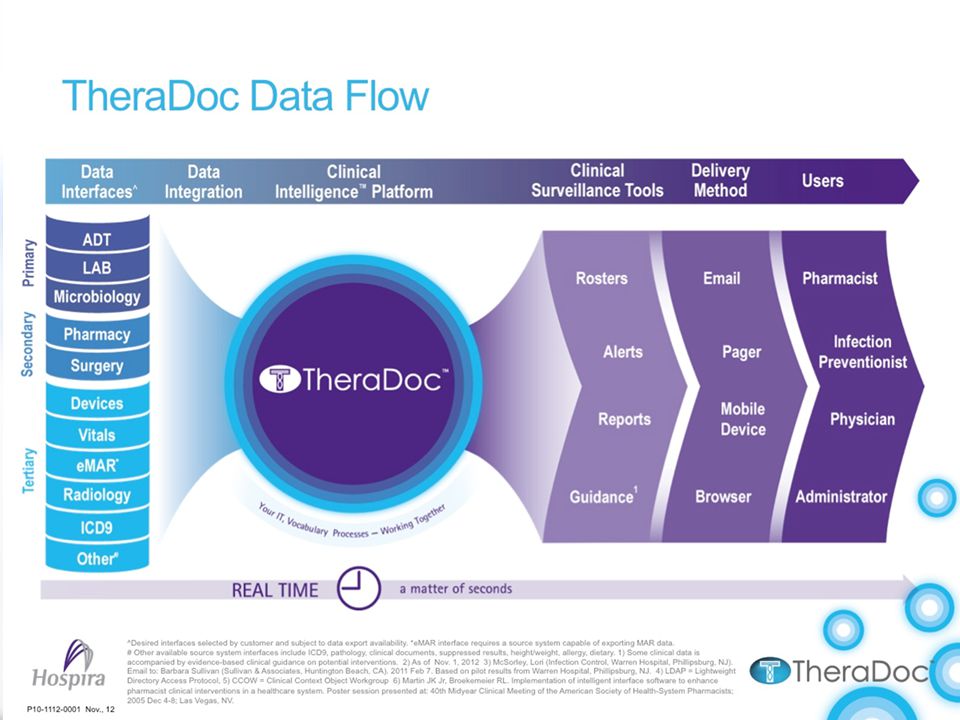
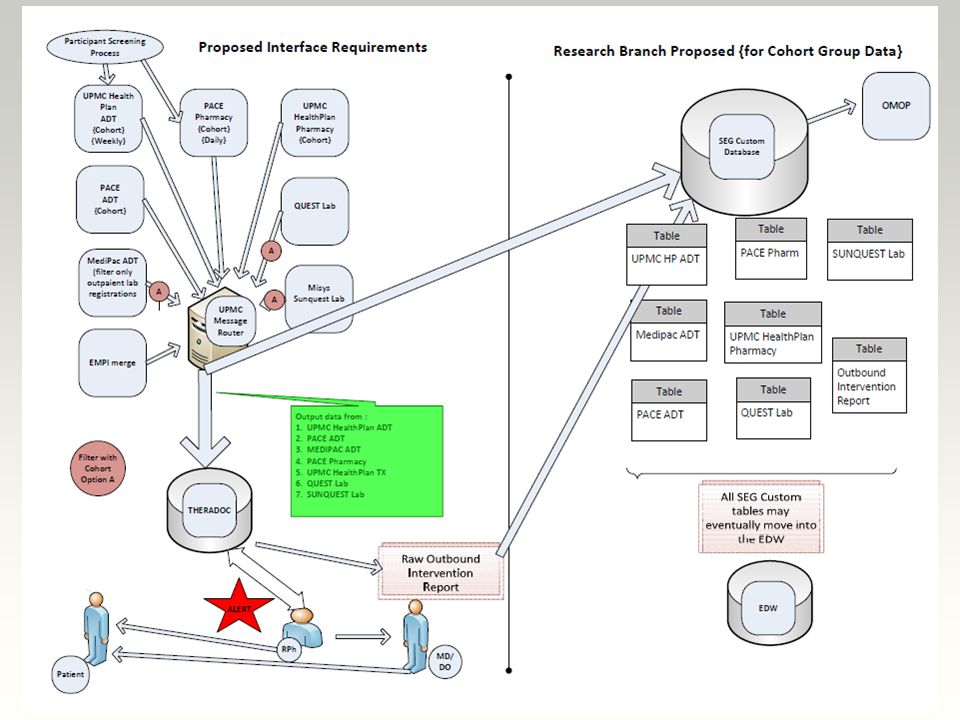
We conducted a retrospective study between February 9, 2012 and February 8, 2013 for all residents at four UPMC NHs located in Southwest Pennsylvania The TheraDoc™ Clinical Surveillance System, which monitors laboratory and medication data and fires alerts when patients have a sufficient increase in SCr, was used for automated case detection Design/Setting/Measurements

12
An increase in SCr in the presence of an active medication order identified to potentially cause AKI triggered an alert, and drug-associated AKI was staged according to the RIFLE criteria –Risk: (1.5 SCr increase) –Injury (2x SCr increase) –Failure (3x SCr increase or increase of 0.5 if SCr ≥ 4) Data were analyzed by frequency and distribution of alert type by risk, injury, and failure Methods (Continued)
 –Injury (2x SCr increase) –Failure (3x SCr increase or increase of 0.5 if SCr ≥ 4) Data were analyzed by frequency and distribution of alert type by risk, injury, and failure Methods (Continued)")
13
Sample ADE Alert

15
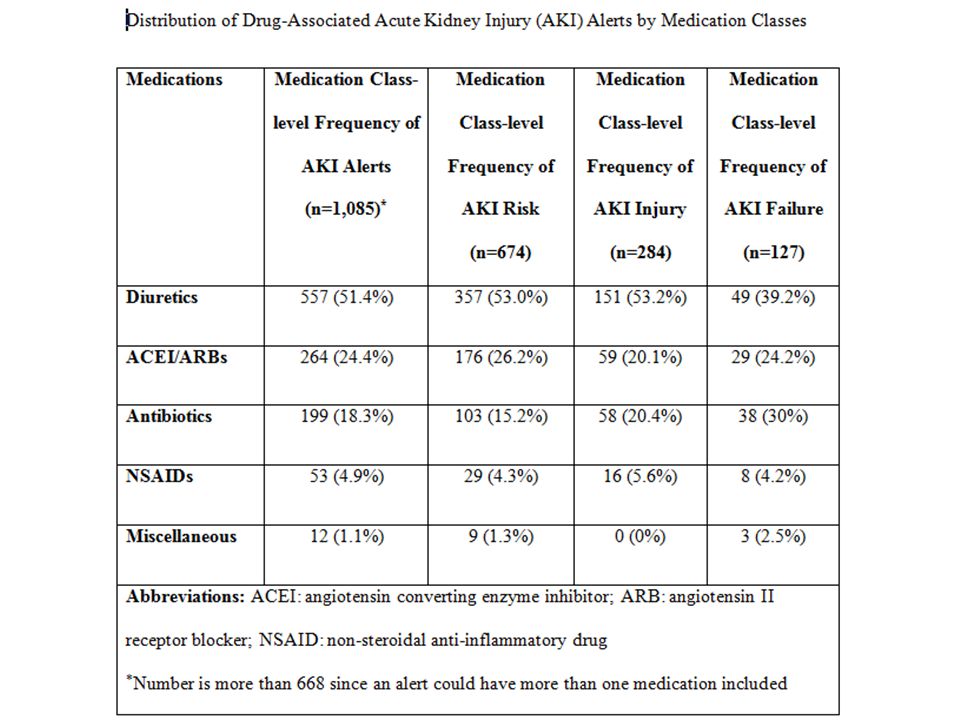
Of the 249 residents who had a drug-associated AKI alert fire, 170 (68.3%) were female, and the mean age was 74.2 years Using the total number of alerts (n=668), the rate of drug-associated AKI was 0.41 events per 100 resident- days Based on the RIFLE criteria, there were 191, 70, and 44 residents who were classified as AKI Risk, Injury, and Failure, respectively The most common medication classes included in the AKI alerts were diuretics, ACEIs/ARBs, and antibiotics Results (Continued)
 were female, and the mean age was 74.2 years Using the total number of alerts (n=668), the rate of drug-associated AKI was 0.41 events per 100 resident- days Based on the RIFLE criteria, there were 191, 70, and 44 residents who were classified as AKI Risk, Injury, and Failure, respectively The most common medication classes included in the AKI alerts were diuretics, ACEIs/ARBs, and antibiotics Results (Continued)")
17
The TheraDoc Clinical Surveillance Software System is currently limited to assessing medications prescribed It is possible that we overestimated the attribution of medications to the development of AKI, as no formal causality assessment tool (e.g., Naranjo algorithm) was used to exclude competing factors, such as comorbid disease, polypharmacy, and volume depletion Limitations
 was used to exclude competing factors, such as comorbid disease, polypharmacy, and volume depletion Limitations")
18
Ideally for staging purposes, patients should be staged according to both RIFLE and Acute Kidney Injury Network (AKIN) criteria that give them the highest stage Limited number of NHs which may limit generalizability Limitations (Continued)
 criteria that give them the highest stage Limited number of NHs which may limit generalizability Limitations (Continued)")
19
This is the first study that assessed the incidence of drug associated AKI in NHs Drug-associated AKI was a common cause of potential ADEs Vast majority of the cases were related to the use of diuretics, ACEIs/ARBs and antibiotics Future studies are needed to better understand patient, provider and facility risk factors as well as strategies to enhance the detection and management of drug-associated AKI in the NH Conclusions

20
QUESTIONS? HANDLERSM@PITT.EDU Thank you!

23
In FY 2011, SNFs transferred one quarter of their Medicare residents to hospitals for inpatient admissions, and Medicare spent $14.3 billion on these hospitalizations Medicare spent an average of $11,255 on each hospitalization of a SNF resident, which was 33.2% above the average cost ($8,447) of hospitalizations for all Medicare residents Office of Inspector General (OIG) Report 23 Office of the Inspector General. Medicare Nursing Home Resident Hospitalization Rates Merit Additional Monitoring, 2013.

Similar presentations