Download presentation
Presentation is loading. Please wait.

1
Blood Component Preparation and Therapeutic Utilization
Prof. A. Pourazar Immunohematologist and Transfusion medicine School of Medicine, Isfahan Medical Science University IRAN

2
Whole Blood Red Blood cells, Platelets and White Blood Cells- all suspended in Plasma constitute Whole Blood.

3
Whole Blood Unit After centrifugation whole blood separates into the plasma and platelets on top and packed red blood cells on the bottom. A plasma expresser is used to squeeze the plasma and pla telets off the top and leave only the red blood cells in the original bag.

4
Blood Components Random donor Platelets Packed Red Blood Cells
Plasma Product When whole blood is separated into it’s component parts we now have Blood Components!!

5
Labeling the Bag Base Label: Bag comes with label indicating manufacturer and anticoagulant/ preservative. 2. Completed label: Paste ABO Group, Rh Type, Collection date, collecting facility etc. on label See Harmening p

6
Base label on bag at time of collection.
Blood Bag label when testing is complete.

7
RBC Components

8
Packed RBCs Approx. half the volume of Whole Blood
Same RBC mass therefore same oxygen carrying capacity Total Volume: ml Hematocrit <80% for CPDA-1 anticoagulant/ preservative. Expiration Date: depends on sterility and anticoagulant/preservative CPDA days closed system AS days closed system Open System - 24 hours

9
RBC:Anticoagulant/Preservative Solutions
Purpose of RBC Preservation Designed to prevent clotting and maintain red cell viability and function during storage. Anticoagulant-Preservative Contents Citrate: anticoagulant (chelates calcium) Dextrose: ATP generation via glycolytic pathway Adenine: Acts as a substrate for RBC synthesis of ATP Sodium diphosphate: Buffer to control decrease of pH expected from generation of lactic acid over time.
 Dextrose: ATP generation via glycolytic pathway. Adenine: Acts as a substrate for RBC synthesis of ATP. Sodium diphosphate: Buffer to control decrease of pH expected from generation of lactic acid over time.")
10
RBC Anticoagulant/Preservative Solutions
Cold Temperature RBC components are kept at 1-6oC in a monitored refrigerator Inhibits bacterial growth Slows glycolytic activity: But RBCs continue metabolic activity during storage consuming nutrients and depleting intracellular energy sources.

11
RBC Component Storage Lesion
Definition: The biochemical changes that occur during storage of RBC components. Changes in Red Blood Cells include: 2,3-DPG, K+, ATP Na+ Changes in the PLASMA include: K+, Ammonia, pH, and haemolysis

12
Indications for Transfusion of Packed Red Blood Cells
Need for blood depends on patients: Oxygen demand Cardiac Output Haemoglobin concentration (Hgb and Hct) Each unit of transfused RBCs increases -Hemoglobin by 1.0 g/dL -Hct by 3%.
 Each unit of transfused RBCs increases. -Hemoglobin by 1.0 g/dL. -Hct by 3%.")
13
Indications for Transfusion of Packed Red Blood Cells…
RBC Transfusion Categories Iatrogenic: neonatal transfusions often result from withdrawal of too much blood for testing. Decreased Bone Marrow Production: Leukemia, aplastic anemia, etc. Decreased RBC Survival: Hemolytic anemia, etc. Surgical/Trauma: Excessive bleeding

14
Indications for Transfusion of Packed Red Blood Cells…
Fresh Red Blood Cells (<7 days old) Neonatal transfusion. Why? Massive Transfusion is defined as replacing the patients entire blood volume within 24 hours. Why would we want to transfuse fresh blood in this situation? 2,3-DPG levels drop within 10 to 15 days of collection to levels that will NOT adequately oxygenate the tissues. Also want to avoid transfusion of excess K+, ammonia and haemolysis.
 Neonatal transfusion. Why Massive Transfusion is defined as replacing the patients entire blood volume within 24 hours. Why would we want to transfuse fresh blood in this situation 2,3-DPG levels drop within 10 to 15 days of collection to levels that will NOT adequately oxygenate the tissues. Also want to avoid transfusion of excess K+, ammonia and haemolysis.")
15
RBC Components continued…
Leukocyte reduced RBC: to a level of <5.0 X 106 per unit Leukocyte filtration: removes WBCs, see p242 Washing- removes WBCs, not efficiently, 24 hour outdate, -see p242 Freezing/Deglycerolization: Frozen RBC unit is thawed and washed to remove both glycerol and WBCs, see p242

16
Indications for Transfusion of Leukocyte Reduced RBCs
Febrile non haemolytic transfusion reactions Patient history of febrile transfusion reactions HLA allo-immunization: antibody to HLA antigens Transfusion related acute lung injury (TRALI) Transfusion associated Graft vs. Host disease (TA-GvHD). Transfusion related immune suppression: - Reduces risk of transmission of CMV and HIV.
 Transfusion associated Graft vs. Host disease (TA-GvHD). Transfusion related immune suppression: - Reduces risk of transmission of CMV and HIV.")
17
RBC Components continued…
Frozen, Deglycerolized RBC Freezing RBCs in glycerol gives minimal damage to the cell. >10 years Shelf life, while in frozen, for ‘rare’ blood types Free (almost) of WBCs, Platelets & Plasma Indicated for patient with anti-IgA; Intra-uterine transfusion (as lacks WBCs) Two methods: Page
 of WBCs, Platelets & Plasma. Indicated for patient with anti-IgA; Intra-uterine transfusion (as lacks WBCs) Two methods: Page")
18
Platelet Components Includes Random donor platelets, Single donor platelets and Pooled Platelets.

19
Platelet Components Preparation
Random Donor From a Whole Blood (WB) Unit at kept 20-24oC, Step 1: WB centrifuged using a Soft (light) Spin for 2-3 min at 3200 rpm (to keep the platelets in the plasma). Step 2: Separate platelet rich plasma from RBCs and using a Hard (heavy) Spin (5 min at 3600 rpm) to settle platelets. Step 3: Express off all but ml of plasma and let platelets rest and resuspend at RT for 1-2 hours Single Donor (by apheresis)
 Unit at kept 20-24oC, Step 1: WB centrifuged using a Soft (light) Spin for 2-3 min at 3200 rpm (to keep the platelets in the plasma). Step 2: Separate platelet rich plasma from RBCs and using a Hard (heavy) Spin (5 min at 3600 rpm) to settle platelets. Step 3: Express off all but ml of plasma and let platelets rest and resuspend at RT for 1-2 hours. Single Donor (by apheresis)")
20
Platelet Components Random Donor Platelet
At least 5.5 x 1010 platelets/unit Store at 20 to 24oC with continuous agitation Suspended in ml plasma Shelf life of 5 days Single Donor Platelet - Apheresis At least 3.0 x 1011 platelets/unit Store at 22 to 24oC with agitation Suspended in 300 ml plasma (equivalent to 4-8 random donor platelets)
")
21
Platelet and Plateletpheresis
Platelet Increment (desired): Patient platelet count should increase by 5-10,000/ random donor platelet transfusion and 30-60,000/ per single donor platelet. ABO and Rh Compatibility Paediatric: Transfuse ABO/Rh compatible units Volume may be reduced by Adults:Want to use ABO compatible with adults but it is NOT necessary. Need to be careful since there is ml of plasma per unit. No cross match is necessary.
: Patient platelet count should increase by 5-10,000/ random donor platelet transfusion and 30-60,000/ per single donor platelet. ABO and Rh Compatibility. Paediatric: Transfuse ABO/Rh compatible units. Volume may be reduced by. Adults:Want to use ABO compatible with adults but it is NOT necessary. Need to be careful since there is ml of plasma per unit. No cross match is necessary.")
22
Platelet refractoriness (Poor platelet increment)
Transfusion of platelets is indicated when patient’s bleeding results from decreased platelet count. Platelet Products Platelet refractoriness (Poor platelet increment) ITP (idiopathic thrombocytopenic purpura) and TTP (thrombotic thrombocytopenic purpura) Due to antibody to platelets: don’t transfuse unless absolutely necessary (ITP and TTP). Adding fuel to the fire. Splenomegaly, drugs or sepsis can also cause platelet refractoriness.
 ITP (idiopathic thrombocytopenic purpura) and. TTP (thrombotic thrombocytopenic purpura) Due to antibody to platelets: don’t transfuse unless absolutely necessary (ITP and TTP). Adding fuel to the fire. Splenomegaly, drugs or sepsis can also cause platelet refractoriness.")
23
Indications for Transfusion of Platelets
Thrombocytopenia Decreased platelet count Causes: Decreased Platelet production: chemo-therapy, malignancy, etc. Increased Platelet destruction: DIC Decrease by dilution: Massive transfusion Transfusion indicated, if associated with bleeding

24
Plasma Components Fresh Frozen Plasma
Plasma expressed from Whole Blood, frozen within 8 hours of collection for CPDA-1 anticoagulant (6 hrs for ACD). Frozen at -18oC: 1 year expiration date Frozen at -65oC: 7 year expiration date Thawed: 24 hour kept at 1-6oC ml total volume Contains all clotting factors
. Frozen at -18oC: 1 year expiration date. Frozen at -65oC: 7 year expiration date. Thawed: 24 hour kept at 1-6oC ml total volume. Contains all clotting factors.")
25
Indications for Transfusion of Plasma Products
Fresh Frozen Plasma (FFP) Treat multiple coagulation factor deficiencies such as DIC, liver failure, vitamin K deficiency, or massive transfusion Good for factor deficiency where there is no suitable clotting factor concentrate: Factor XI deficiency NEED to be ABO compatible. No cross-match needed Contraindicated for volume expansion and protein replacement.
 Treat multiple coagulation factor deficiencies such as DIC, liver failure, vitamin K deficiency, or massive transfusion. Good for factor deficiency where there is no suitable clotting factor concentrate: Factor XI deficiency. NEED to be ABO compatible. No cross-match needed. Contraindicated for volume expansion and protein replacement.")
26
Plasma Substitutes Colloid Solutions Albumin: 5% and 25%
Plasma Protein Fraction: 5% albumin and non albumin plasma proteins Crystalloid Solutions Normal saline, lactated Ringers, dextran Indications: Volume expansion/protein replacement without risk of transfusion transmitted viruses. Advantages over plasma: No disease transmission, cost, reduced risk of allergic reactions.

27
Cryoprecipitated Antihemophilic Factor (Cryo)
Cold insoluble portion of Plasma Preparation Procedure (Page 246) Take FFP and thaw at 1 to 6oC until it becomes slushy (14-16 hours) centrifuged using Hard Spin (5-7 min at 3500 rpm). Remove cryo-poor plasma leaving about ml of plasma with Cryo-precipitates. Freeze Cryo at -18oC for 12 months
 Take FFP and thaw at 1 to 6oC until it becomes slushy (14-16 hours) centrifuged using Hard Spin (5-7 min at 3500 rpm). Remove cryo-poor plasma leaving about ml of plasma with Cryo-precipitates. Freeze Cryo at -18oC for 12 months.")
28
Cryoprecipitated Antihemophilic Factor (Cryo)
Contains at least 80 units of AHF and mg Fibrinogen Also contains Factor XIII and von Willebrands factor Must be transfused within 6 hours of thawing or within 4 hours of pooling Once thawed store at room temperature until transfusion

29
Indications for Transfusion of Cryoprecipitated AHF
Primary use: intravenous supplementation of Factor XIII and fibrinogen Topical Use: Fibrin sealant (glue) in surgery Factor concentrates (i.e. Factor VIII) have replaced CRYO in many situations because of reduced risk of transmission of disease. See Table 16-4, Page 349 Harmening
 in surgery. Factor concentrates (i.e. Factor VIII) have replaced CRYO in many situations because of reduced risk of transmission of disease. See Table 16-4, Page 349 Harmening.")
30
Granulocyte Concentrates
Prepared by Pheresis (Chapter 17) Single donor component Should contain 1 x 1010 granulocytes/unit ml plasma and red cells Must be ABO and Crossmatch compatible with recipient Store at 20oC to 24oC Shelf life is 24 hours
 Single donor component. Should contain 1 x 1010 granulocytes/unit ml plasma and red cells. Must be ABO and Crossmatch compatible with recipient. Store at 20oC to 24oC. Shelf life is 24 hours.")
31
Indications for Transfusion of Granulocyte
Patient should meet the following conditions: Neutropenia: WBC count <500/mL Fever for hours, positive bacterial or fungal cultures, unresponsive to antibiotic therapy. Myeloid hypoplasia A reasonable chance for recovery of marrow function. Component should be irradiated and CMV seronegative.

32
Irradiated Blood Components
Gamma irradiation of component Purpose: Inactivate donor lymphocytes to prevent Graft Vs. Host disease (GVHD). Only accepted method. Expiration date: 28 days (RBCs) from irradiation or original outdate - which ever comes first.
. Only accepted method. Expiration date: 28 days (RBCs) from irradiation or original outdate - which ever comes first.")
33
Indications for Transfusion of Irradiated Blood Products
Congenital Immunodeficiency's: SCID, Di George Syndrome Hodgkin's Lymphoma Bone Marrow Transplant Intrauterine Transfusion to Fetus Exchange transfusion: Neonate Transfusion of first degree relative: Blood relative

34
ALL BLOOD COMPONENTS ARE ADMINISTERED THROUGH A FILTER!
Necessary to remove any accumulated debris that may be present in the blood component such small clots, fibrin, etc.

35
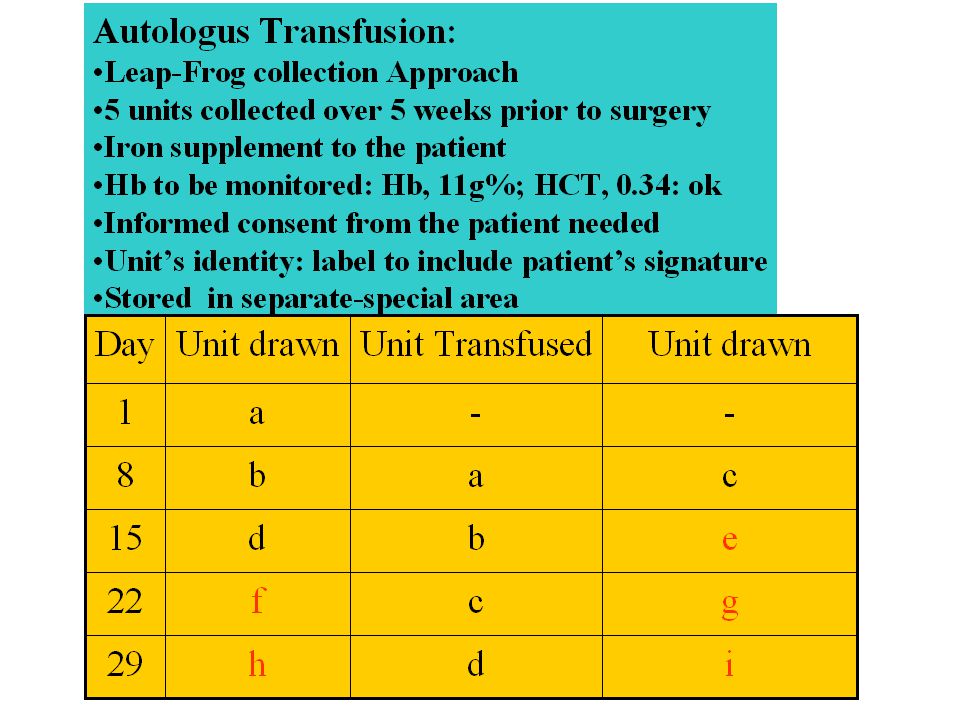
Autologous Blood Transfusion
Donation from the recipient, Rare blood type Having antibody to high frequency antigen Having a presence of multiple CSA Useful in planned surgery Large number of units by leap-frog method

Similar presentations
BB>")


 – Leukocytes (WBCs) – Thrombocytes (platelets) Plasma – 90% water – 10% solutes – Proteins,>")





 Blood-cells products whole blood packed red blood cells leukocyte-poor (reduced) red cells washed red blood cells random-donor.>")









