Download presentation
Presentation is loading. Please wait.

1
DR SACHIN VERMA MD( MEDICINE),FICM,FCCS CONSULTANT INTERNAL MEDICINE & CRITICAL CARE IVY HOSPITAL MOHALI Hepatitis D
,FICM,FCCS CONSULTANT INTERNAL MEDICINE & CRITICAL CARE IVY HOSPITAL MOHALI Hepatitis D")
3
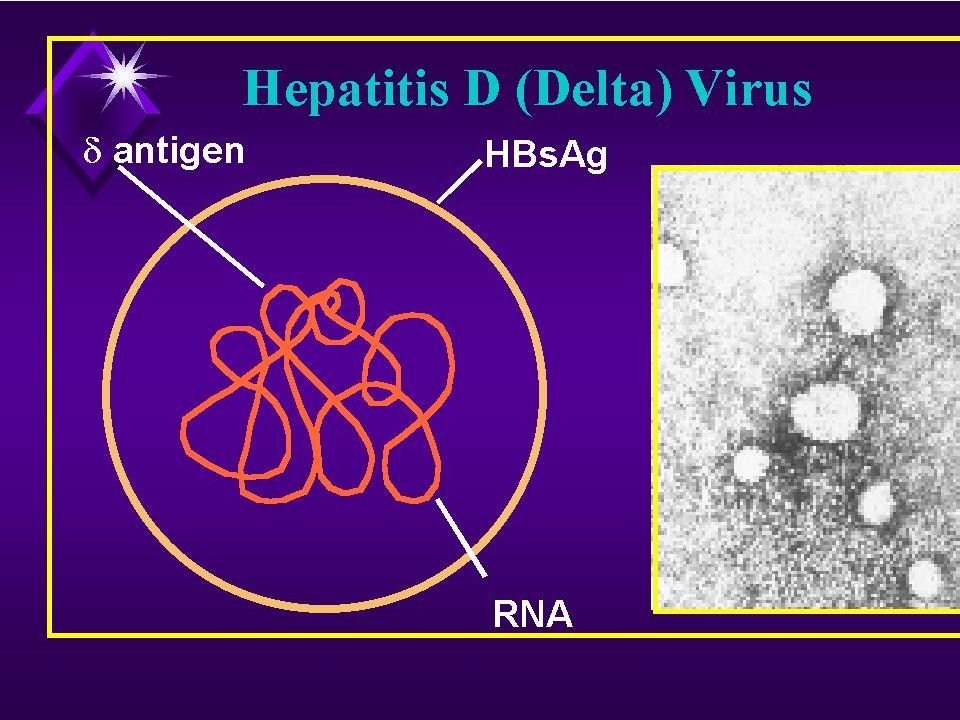
Introduction Recognized in 1977 – co existent with HBV infection A defective RNA virus than need hepadnavirus (HBV) to replicate 1980 – noticed the dependency of HDV to HBV (need HBsAg to as virion coat) Associated with most severe form of acute and chronic HBsAg +
 to replicate 1980 – noticed the dependency of HDV to HBV (need HBsAg to as virion coat) Associated with most severe form of acute and chronic HBsAg +")
4
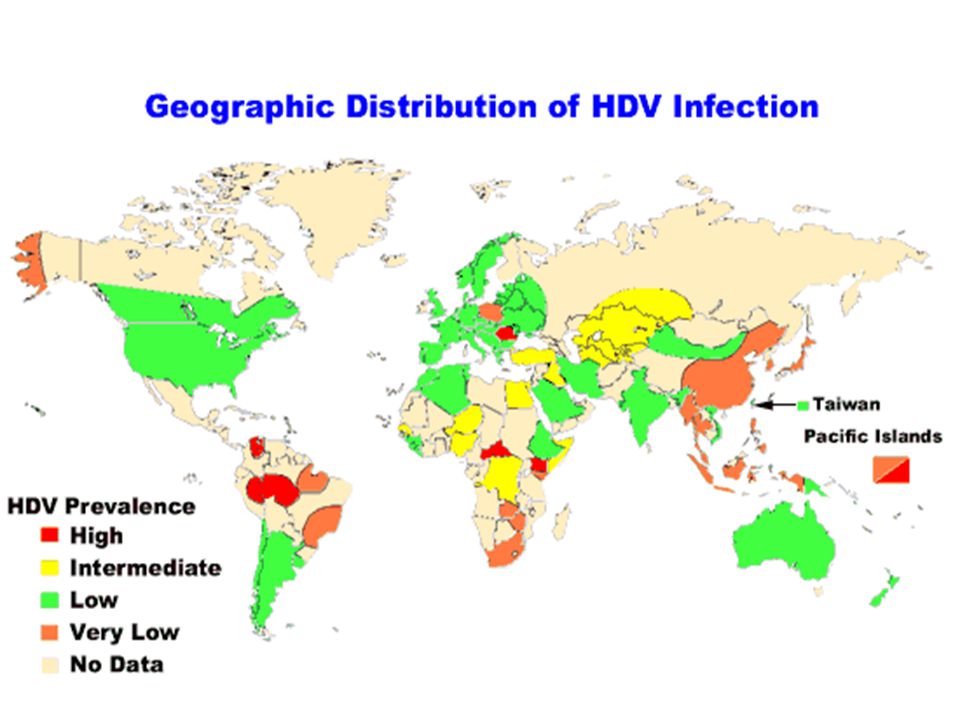
Epidemiology of Hepatitis D Spread worldwide Highest in Russia, Romania, Southern Italy, Mediterranean countries, Africa, South America Low in China, Taiwan, India Latest trends New foci in Okinawa, certain area of China, India, Albania Decreasing trend in Mediterranean

6
Prevalence in region New Delhi : 8.1% in 1996[ Irshad M et al. Eur J Gastroenterol Hepatol 1996; 8: 995-99816] New Delhi: 10.6% in 2005[ Chakraborty P et al. Indian J Med Res2005; 122: 254-25715 ] Chandigarh :14.2%[ Singh et al. J Viral Hepat 1995; 2: 151-15417]. Ludhiana:10% in HBsAg-positive patients [Ghuman et al. Indian J Med Sci 1995; 49: 227-23023].

7
Mode of Transmission Spread Percutaneous and sexually and through body fluid/blood Potentially infectious in whole phase People at risk HBV carrier, HBV unvaccinated person IVDU Unprotected sex Exposed to unscreen blood, body fluid People receiving blood, blood product

8
Hepatitis D Features IP – 5 to 64 days Super-infection* or co-infection with HBV

9
CLINICAL FEATURES : In acute CO-Infection jaundice,fatigue, abdominal pain, loss of appetite, nausea, vomiting,joint pain, dark (tea colored) urine In super-infection CLD and HCC.
 urine In super-infection CLD and HCC.")
10
DIAGNOSIS Following HBV-HDV co-infection both IgM anti- HDV during the acute illness and IgG anti- HDV during convalescence are detectable Following HBV-HDV super infection, chronic HDV infection with detectable HDAg usually occurs. Both IgM anti-HDV and IgG anti-HDV remain detectable.

11
DIAGNOSIS Anti LKM3 antibodies

12
Serologic Course

14
Prevention HBV-HDV Coinfection Pre or postexposure prophylaxis to prevent HBV infection. HBV-HDV Superinfection Education to reduce risk behaviors among persons with chronic HBV infection

15
TREATMENT: 1. Acute HDV infection a) Supportive care 2. Chronic HDV infection 1. interferon-alfa 2. liver transplant

16
a-interferon 2b 9 mu sc tiw, Rx > 12 months 21-50% lose HDV RNA and have improved histology Relapse occurs in almost all patients stopping treatment Can stop treatment if HBV Surface Ag disappears (rare)
")
17
Thank you

Similar presentations
















BB Unit 4 Part 4 Hepatitis A-E Viruses.>")


 Virus Division of Viral Hepatitis.>")
