Download presentation
Presentation is loading. Please wait.

1
Presentor: Ainani Aima Ismail Supervisor: Dr Lee Pui Kuan
JOURNAL PRESENTATION Presentor: Ainani Aima Ismail Supervisor: Dr Lee Pui Kuan

2
MULTIMODAL THERAPIES FOR POSTOPERATIVE NAUSEA AND VOMITING AND PAIN
SOCIETY FOR AMBULATORY ANAESTESIA GUIDELINES FOR THE MANAGEMENT OF POSTOPERATIVE NAUSEA AND VOMITING – TJ GAN et all, anaesthesia and anagesia, December 2007 vol. 105 no MULTIMODAL THERAPIES FOR POSTOPERATIVE NAUSEA AND VOMITING AND PAIN A Chandrakantan and P.S.A glass, Br. J. Anaesth. (2011) 107 (suppl 1): i27-i40.
 107 (suppl 1): i27-i40.")
3
Incidence of PONV varies considerably in both inpatient and outpatient setting
Untreated, PONV occurs in 20-30% of the general surgical population and up to 70-80% of high risk surgical patients

4
Adverse effects of PONV range from patient- related distress to postoperative morbidity
PONV associated with ambulatory surgery increases health care costs due to hospital admission and accounts for 0.1 – 0.2% of these unanticipated admissions

5
GOALS OF GUIDELINES Identify the primary risk factors for PONV in adults and postoperative vomiting in children Establish factors that reduce the baseline risks for PONV Determine the most effective antiemetic monotherapies and combination therapy regimens for PONV/POV prophylaxis, including pharmacologic and nonpharmacologic approaches

6
4. Ascertain the optimal approach to treatment of PONV with or without PONV prophylaxis 5. Determine the optimal dosing and timing of antiemetic prophylaxis 6. Evaluate the cost-effectiveness (C/E) of various PONV management strategies using incremental C/E ratio (cost of treatment A − cost of treatment B)/(success of treatment A − success of treatment B) 7. Create an algorithm to identify individuals at increased risk for PONV and to suggest effective treatment strategies
 of various PONV management strategies using incremental C/E ratio (cost of treatment A − cost of treatment B)/(success of treatment A − success of treatment B) 7. Create an algorithm to identify individuals at increased risk for PONV and to suggest effective treatment strategies .")
7
GUIDELINES Identify patients’ risk for PONV
Reduce baseline risk factors for PONV Administer PONV prophylaxis using one to two intervention in adults at moderate risk for PONV Administer prophylactic therapy with combination (>2) interventions/multimodal therapy in patients at high risk for PONV Administer prophylactic antiemetic therapy to children at increased risk for POV; as in adults, use of combination therapy is most effective Provide antiemetic treatment to patient with PONV who did not receive prophylaxis or in whom prophylaxis failed
 interventions/multimodal therapy in patients at high risk for PONV. Administer prophylactic antiemetic therapy to children at increased risk for POV; as in adults, use of combination therapy is most effective. Provide antiemetic treatment to patient with PONV who did not receive prophylaxis or in whom prophylaxis failed.")
8
GUIDELINE 1: Identify patients’ risk for PONV
Can indicate who will most likely benefit from prophylactic antiemetic therapy In adult, only a few baseline risk factors occur with enough consistency to be considered independent predictors for PONV Some studies also reported migraine, young age, anxiety, and patient with low ASA risk classification are independent predictors for PONV

9
RISK FACTORS OF PONV Patient - specific Female gender
Non smoking status History of PONV / motion sickness Anaesthetic Volatile anesthetics Nitrous oxide Intraoperative and post operative opiods usage Surgical Duration of surgery Types of surgery

10
Many factors commonly believed to augment risk are not actually independent factors. These include obesity, anxiety, antagonizing neuromuscular blockade More liberal prophylaxis is appropriate for patients whom vomiting poses a particular medical risk including those with wired jaw, increased ICP, gastric / esophageal surgery and when the anaesthesia care provider determines the need or the patients has a a strong preferences to avoid PONV

11
Figure 1. Simplified risk score for PONV in adults (3).
Figure 1. Simplified risk score for PONV in adults (3). Simplified risk score from Apfel et al. (3) to predict the patients risk for PONV. When 0, 1, 2, 3, or 4 of the depicted independent predictors are present, the corresponding risk for PONV is approximately 10%, 20%, 40%, 60%, or 80%. Gan T J et al. Anesth Analg 2007;105: ©2007 by Lippincott Williams & Wilkins
. Simplified risk score from Apfel et al. (3) to predict the patients risk for PONV. When 0, 1, 2, 3, or 4 of the depicted independent predictors are present, the corresponding risk for PONV is approximately 10%, 20%, 40%, 60%, or 80%. Gan T J et al. Anesth Analg 2007;105: ©2007 by Lippincott Williams & Wilkins.")
12
Figure 2. Simplified risk score for POV in children (39).
Figure 2. Simplified risk score for POV in children (39). Simplified risk score from Eberhart et al. (39) to predict the risk for POV in children. When 0, 1, 2, 3, or 4 of the depicted independent predictors are present, the corresponding risk for PONV is approximately 9%, 10%, 30%, 55%, or 70%. Gan T J et al. Anesth Analg 2007;105: ©2007 by Lippincott Williams & Wilkins
. Simplified risk score from Eberhart et al. (39) to predict the risk for POV in children. When 0, 1, 2, 3, or 4 of the depicted independent predictors are present, the corresponding risk for PONV is approximately 9%, 10%, 30%, 55%, or 70%. Gan T J et al. Anesth Analg 2007;105: ©2007 by Lippincott Williams & Wilkins.")
13
Pathophysiology of PONV
Emesis is believed to be governed by the emesis centre in the brain, which receives several afferent inputs. Vagal input from the gut can activate the emetic centre, and also afferent action from the chemoreceptor trigger zone (CTZ). The CTZ sits outside the blood–brain barrier and contains several different receptors that modulate its activity.
. The CTZ sits outside the blood–brain barrier and contains several different receptors that modulate its activity.")
14
Most antiemetic medications act by either a direct or indirect antagonizing of emetogenic substances on receptors in the CTZm Antiemetic work on several different receptors sites to prevent / treat PONV

15
CTZ and emetic centre. CTZ and emetic centre. With permission from Watcha and White.73 Chandrakantan A , and Glass P S A Br. J. Anaesth. 2011;107:i27-i40 © The Author [2011]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please

16
GUIDELINE 2: Reduce baseline risk factors for PONV
Avoidance GA by the use of regional anesthesia 2. Use of propofol for induction & maintenance 3. Avoidance of nitrous oxide 4. Avoidance of volatile anesthetics 5. Minimization of intraoperative & postoperative opioids 6. Minimization of neostigmine Adequacy hydration

17
IMPACT study evaluated several strategies to reduce PONV in 5199 high risk patient
59% incidence of PONV in patient treated with volatile nitrous oxide Use of propofol reduce PONV risk by 19% Avoidance of nitrous oxide reduce PONV risk by 12% Combination of propofol and air/oxygen had additive effects, reducing PONV risk by 25%

18
GUIDELINE 3: Administer PONV prophylaxis using one to two intervention in adults at moderate risk for PONV 5-HT3 receptor antagonists Dexamethasone Butyrophenones Dimenhydrinate Transdermal scopolamine

19
The recommended 1st and 2nd line pharmacologic antiemetics for PONV prophylaxis in adults
the 5-hydroxytryptamine (5-HT3) receptor antagonists (ondansetron, dolasetron, granisetron, and tropisetron), steroid (dexamethasone), phenothiazines (promethazine and prochlorperazine), phenylethylamine (ephedrine), butyrophenones (droperidol, haloperidol), antihistamine (dimenhydrinate), anticholinergic (transdermal scopolamine
 receptor antagonists (ondansetron, dolasetron, granisetron, and tropisetron), steroid (dexamethasone), phenothiazines (promethazine and prochlorperazine), phenylethylamine (ephedrine), butyrophenones (droperidol, haloperidol), antihistamine (dimenhydrinate), anticholinergic (transdermal scopolamine.")
21
Side-effects of commonly used antiemetics by drug class
Serotonin antagonists Headache, diarrhoea, constipation, arrhythmia Neurokinin inhibitors Dizziness, diarrhoea, headaches, weakness Steroids Dizziness, mood changes, nervousness Antihistamines Confusion, drying of mucosal membranes, sedation, urinary retention Butyrophenones Prolonged QT interval (at doses ≥0.1 mg kg−1), hypotension, tachycardia, extra-pyramidal symptoms Benzodiazepines Sedation, disorientation
, hypotension, tachycardia, extra-pyramidal symptoms. Benzodiazepines. Sedation, disorientation.")
22
5-HT3 receptor antagonists
E.g: ondansetron, dolasetron, granisetron, and tropisetron Most effective in the prophylaxis of PONV when given at the end of surgery

23
Dexamethasone Effectively prevents nausea and vomiting
Prophylactic dose 4-5mg (IV) Recommended timing for administration is at induction of anaesthesia rather than at the end of surgery
 Recommended timing for administration is at induction of anaesthesia rather than at the end of surgery.")
24
Butyrophenones E.g : droperidol, haloperidol
The efficacy of droperidol is equivalent to that of ondansetron for PONV prophylaxis Many physicians have stopped using droperidol due to the FDA “black box” restrictions on its use Haloperidol, which has antiemetic properties when used in low doses, has been investigated as an alternative to droperidol

25
DIMENHYDRINATE An antihistamine with antiemetic effect
Data from placebo controlled trial suggest that its degree of antiemetic efficacy may be similar to the 5HT3 receptor antagonists, dexamethasone and droperidol

26
TRANSDERMAL SCOPOLAMINE
A systematic review of transdermal scopolamine shows that it is useful as an adjunct to other antiemetic therapies It is applied the evening before surgery or 4h before the end of the anaesthesia due to its 2-4h onset of effect, which may be problematic in some centers

27
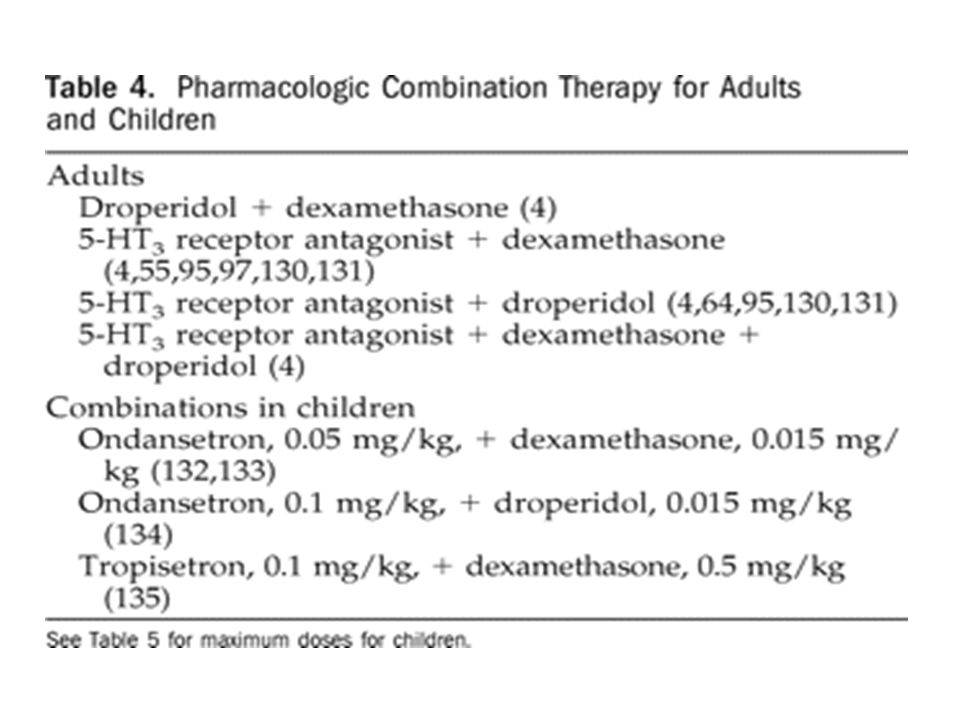
Combination therapy Adults at moderate risk for PONV should receive combination therapy with one or more prophylactic drugs from different classes combination therapy has superior efficacy compared with monotherapy for PONV prophylaxis Drugs with different mechanisms of action should be used in combination to optimize efficacy the combination of a 5-HT3 antagonist and promethazine significantly reduced both the frequency and severity of nausea and vomiting

29
Lack or Limited Evidence of Effect
Some therapies have proven ineffective for PONV prophylaxis. These include metoclopramide when used in standard clinical doses (10 mg IV), ginger root, and cannabinoids (nabilone, tetra-hydrocannabinol) which, although promising in the control of chemotherapy-induced sickness, are not effective in PONV In two randomized trials, the phenothiazines, promethazine, 12.5–25 mg IV, administered at the induction of surgery, and prochlorperazine, 5–10 mg IV, given at the end of surgery were shown to have some antiemetic efficacy it was suggested that the phenylethylamine, ephedrine, 0.5 mg/kg IM, may have an antiemetic effect when administered at the end of surgery
, ginger root, and cannabinoids (nabilone, tetra-hydrocannabinol) which, although promising in the control of chemotherapy-induced sickness, are not effective in PONV. In two randomized trials, the phenothiazines, promethazine, 12.5–25 mg IV, administered at the induction of surgery, and prochlorperazine, 5–10 mg IV, given at the end of surgery were shown to have some antiemetic efficacy. it was suggested that the phenylethylamine, ephedrine, 0.5 mg/kg IM, may have an antiemetic effect when administered at the end of surgery.")
30
Nonpharmacologic Prophylaxis
A meta-analysis of nonpharmacologic PONV prophylaxis demonstrated antiemetic efficacy with acupuncture, transcutaneous electrical nerve stimulation, acupoint stimulation, and acupressure P6 stimulation was particularly effective at reducing the incidence and severity of nausea (19%) compared with ondansetron (40%) and placebo (79%)
 compared with ondansetron (40%) and placebo (79%)")
31
GUIDELINE 4: Administer prophylactic therapy with combination (>2) intervention / multimodal therapy in patients at high risk for PONV
 intervention / multimodal therapy in patients at high risk for PONV")
32
Multimodal therapy Multimodal approach constitutes both pharmacological and non pharmacological therapies, which commences in the preoperative area and continues until discharge of the patient In the preoperative area, minimizing anxiety is important. Anxiolysis with benzodiazepines has been shown to reduce PONV in several small studies Other interventions to minimize anxiety include optimizing information provided to the patient, a patient-friendly facility layout, and positive and compassionate interactions with staff

33
Scuderi et al. tested the efficacy of a multimodal approach to reducing PONV.
Their multimodal approach consisted of preoperative anxiolysis and aggressive hydration; oxygen; prophylactic antiemetics (droperidol and dexamethasone at induction and ondansetron at end of surgery); total IV anesthesia with propofol and remifentanil; and ketorolac. No nitrous oxide or neuromuscular blockade was used. Patients who received multimodal therapy had a 98% complete response rate compared with a 76% response rate among patients receiving antiemetic monotherapy and a 59% response rate among those receiving routine anesthetic plus saline placebo
; total IV anesthesia with propofol and remifentanil; and ketorolac. No nitrous oxide or neuromuscular blockade was used. Patients who received multimodal therapy had a 98% complete response rate compared with a 76% response rate among patients receiving antiemetic monotherapy and a 59% response rate among those receiving routine anesthetic plus saline placebo.")
34
Figure 3. Algorithm for management of postoperative nausea and vomiting (PONV).
.")
35
GUIDELINE 5: Administer prophylactic antiemetic therapy to children at increased risk for POV; as in adults, use of combination therapy is most effective

36
In children, the POV rate can be twice as high as in adults, which suggests a greater need for POV prophylaxis in this population Children who are at the moderate or high risk for POV should receive combination therapy with prophylactic drugs from different classes

37
Because the 5-HT3 antagonists as a group have greater efficacy for the prevention of vomiting than nausea, they are the drugs of first choice for prophylaxis in children. Meta-analyses and single studies have shown that the 5-HT3 antagonists are superior to droperidol and metoclopramide for the prophylaxis of POV in children.

39
GUIDELINE 6: Provide antiemetic treatment to patient with PONV who did not receive prophylaxis or in whom prophylaxis failed

40
When PONV occurs postoperatively, treatment should be administered with an antiemetic from a pharmacologic class that is different from the prophylactic drug initially given, or, if no prophylaxis was given, the recommended treatment is a low-dose 5-HT3 antagonist

41
Alternative treatments for established PONV include dexamethasone, 2–4 mg IV, droperidol, mg IV, or promethazine 6.25–12.5 mg IV Propofol, 20 mg as needed, can be considered for rescue therapy in patients still in the PACU and has been found as effective as ondansetron

42
The attempt at rescue should be initiated when the patient complains of PONV and, at the same time, an evaluation should be performed to exclude an inciting medication or mechanical factor for nausea and/or vomiting Contributing factors might include a morphine PCA, blood draining down the throat, or an abdominal obstruction

43
POST DISCHARGED NAUSEA AND VOMITING
Defined from 24h post discharged up to 72h Incidence is up to 55% A systematic review of 58 articles demonstrated that use of propofol versus inhaled anesthesia also reduced the incidence of PDNV (P < 0.05) Small randomized controlled trials have demonstrated efficacy in preventing PDNV with orally disintegrating ondansetron tablets, acupoint stimulation of P6, and transdermal scopolamine
 Small randomized controlled trials have demonstrated efficacy in preventing PDNV with orally disintegrating ondansetron tablets, acupoint stimulation of P6, and transdermal scopolamine.")
44
CONCLUSION Not all surgical patients will benefit from antiemetic prophylaxis identification of patients who are at increased risk leads to the most effective use of therapy and the greatest cost-efficacy. Although antiemetic prophylaxis can not eliminate the risk for PONV, it can significantly reduce the incidence.

45
Depending upon the level of risk, prophylaxis should be initiated with monotherapy or combination therapy using interventions that reduce baseline risk, nonpharmacologic approaches, and antiemetics When rescue therapy is required, the antiemetic should be chosen from a different therapeutic class than the drugs used for prophylaxis

Similar presentations






 and Post discharge nausea and Vomiting.>")










 and Inpatient (Study 2) Settings Study.>")




