Download presentation
Presentation is loading. Please wait.

1
School Employee Health Care Board Conference Joe San Filippo Chief Health Care Strategist Nationwide Better Health

2
Water Level Health Promotion/ Lifestyle Management Disease Management Population at risk who have filed a claim Health Maintenance Population with no known risk factors Total Population Population with risk but not sick Water Level Understanding Health Risks Total Population Health Management

3
Boden WE et al. NEJM 2007;356

4
Treatment Groups PCI (n=1149) OMT (n=1138) Both groups received OMT, which included cardio-protective medications (e.g., ASA, BB, ACE-inhibitors, anti-platelet agents, statins) as well as smoking cessation, exercise, weight control and nutrition counseling.
 OMT (n=1138) Both groups received OMT, which included cardio-protective medications (e.g., ASA, BB, ACE-inhibitors, anti-platelet agents, statins) as well as smoking cessation, exercise, weight control and nutrition counseling.")
5
Cumulative Event Rates at 4.6 Years PCI Group Medical Tx Group p Value Outcome#%#% Death, nonfatal MI21119.020218.50.62 Death, MI, Stroke22220.021319.50.62 Death857.6958.30.38 Nonfatal MI14313.212812.30.33 Stroke222.1141.80.19 Hospitalization*13512.412511.80.56 Revascularization **22821.134832.6<0.001 * for ACS; ** PCI or CABG

6
Approximate Mortality Reduction Potential of Drug Vs Lifestyle Interventions in Patients with Coronary Disease* Drug Lifestyle Low dose aspirin18% Statins21% ß Blockers23% ACE Inhibitors26% Smoking cessation35% Physical activity25% Moderate alcohol20% Combined lifestyle changes45% Iestra JA et al. Circ 2005;112:924

7
Two meta-analyses now suggest that regular exercise can reduce the overall risk of cardiovascular events by up to 50% 5 0 % Powell KE et al. Annu Rev Publ Health 1987;8:253 Berlin JA et al. Am J Epidemiol 1991;134:232

8
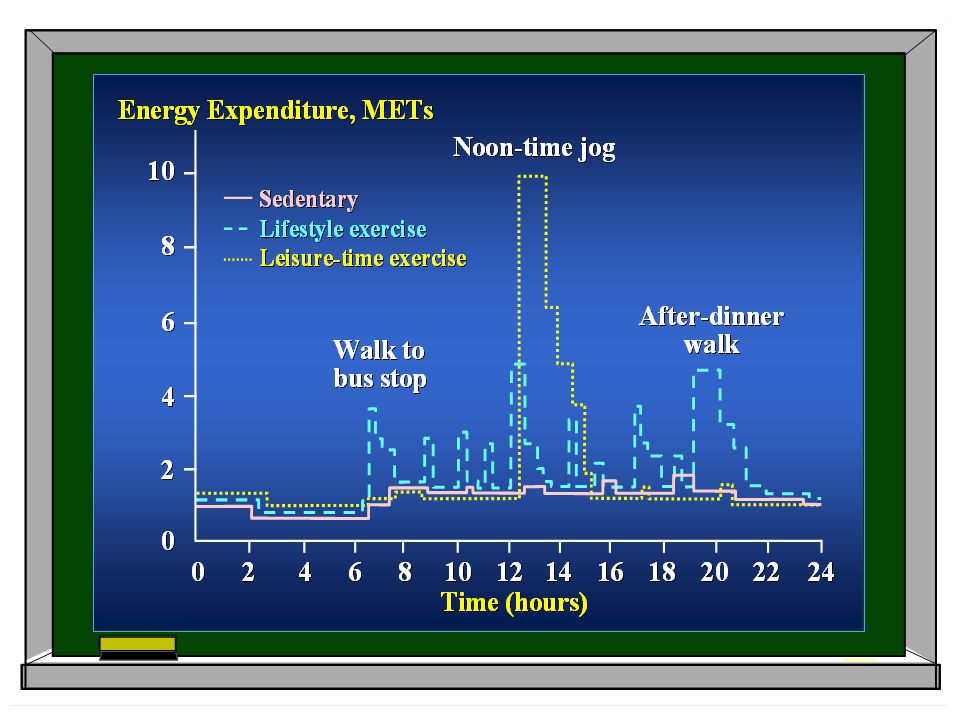
Benefit Dose- Response Curve A = Sedentary B = Moderately Active C = Active Baseline Activity Status ABC LowHigh

10
Conventional Risk Factors for Coronary Heart Disease 4 Risk Factors CigaretteSmokingCigaretteSmokingHyper-lipidemiaHyper-lipidemiaHyper-tensionHyper-tensionDiabetesDiabetes 87% to 100% of patients who experienced a fatal coronary event had an antecedent exposure to 1 risk factor.* > 80% of patients with coronary disease had 1 of the 4 conventional risk factors.** * JAMA 2003;290:891 ** JAMA 2003;290:898

11
Lifetime Risk: Age 50 Lloyd-Jones DM et al. Circ 2006;113:791 0. 7 0.6 0.5 0.4 0.3 0.2 0.1 0 50607080905060708090 ≥ 2 Major RFs 1 Major RF ≥ 1 Elevated RF ≥ 1 Not Optimal RF All Optimal RFs 69% 50% 46% 36% 5% 50% 39% 27% 8% Adjusted Cumulative Incidence Attained Age

12
HRA Stratification Referrals Disease Management and Lifestyle Management HRA Trigger Questions Diabetes Confirmed CAD Confirmed Hypertension Confirmed Hyperlipidemia Maternity COPD Asthma Depression Recurrent Long-term Lower Back Pain Unconfirmed CAD or Hyperlipidemia Unconfirmed Hypertension Anxiety / Stress Overweight Physical Activity / Exercise Tobacco Cessation Lifestyle Management Referrals Disease Management Referrals Referrals From “Triggers”

13
Our predictive modeling tool determines relative risk scores unique to conditions and identifies risk 12 months prior to an episode. Predictive Modeling HealthCheck HRA Gaps in Care Treatment Compliance Stratification / Intervention Elements Combines predictive modeling that identifies and stratifies members with our proprietary business rules, so that we effectively prioritize and manage co-morbidities Proprietary RiskScreen ® High Acuity Low Acuity Moderate Acuity RiskScreen ® Process Medical Claims Data Pharmacy Claims Data Population With Risk Factors

14
Diabetes Coronary Artery Disease Congestive Heart Failure Chronic Obstructive Pulmonary Disease Low Back Pain Asthma Core Conditions All Chronic Conditions Precursors Maternity Oncology 1 year program Arthritis GERD HIV Self Referral Depression Optional Coverage Core Conditions represent the health conditions where we can have the maximum impact on improving health and reducing costs. Hypertension Hyperlipidemia Runs through six weeks post-partum tailored to member during treatment cycle Obesity Disease Management Program

15
Welcome Kit Telephonic Outreach Clinical Assessment Determine Appropriate Program High Acuity Low Acuity Moderate Acuity Identification LOW Intervention MODERATE Intervention HIGH Intervention Components of the Disease Management Process Disease Management Process

16
Welcome Kit Telephonic Outreach Clinical Assessment Disease Management Process High Acuity Low Acuity Moderate Acuity Identification Methods of Identification Determine Appropriate Program RiskScreen ® Predictive Modeling Health Risk Assessment Biometric Screening Referral Opportunities Case Management Disability Management EAP Lifestyle Health Coaching Maternity Management Nurse Advice Line On-site opportunities (health fairs, clinics) Self referral Utilization Management LOW Intervention MODERATE Intervention HIGH Intervention
 Self referral Utilization Management LOW Intervention MODERATE Intervention HIGH Intervention")
17
Clinical Assessment Disease Management Process Welcome Kit Contents Determine Appropriate Program Welcome Kit Telephonic Outreach High Acuity Low Acuity Moderate Acuity Identification Welcome letter Disease-specific educational materials Instructions to access specific lifestyle management kits online Self-assessment tool to encourage engagement with a coach Member experience brochure Note: if member self-refers they will only receive applicable disease-specific literature LOW Intervention MODERATE Intervention HIGH Intervention

18
Telephonic Outreach Clinical Assessment Disease Management Process Telephonic Outreach Determine Appropriate Program Welcome Kit High Acuity Low Acuity Moderate Acuity Identification Up to 8 calls in 30 days Track time of day and day of week to maximize outreach If we are unable to contact member during initial outreach phase, we’ll continue to contact them via phone and mail for the remainder of the year. LOW Intervention MODERATE Intervention HIGH Intervention

19
Disease Management Process Clinical Assessment Lifestyle Functionality Disease specific behaviors Disease specific clinical values Welcome Kit Telephonic Outreach Clinical Assessment High Acuity Low Acuity Moderate Acuity Identification Determine Appropriate Program LOW Intervention MODERATE Intervention HIGH Intervention

20
Disease Management Process Program Interventions Welcome Kit Telephonic Outreach Clinical Assessment High Acuity Low Acuity Moderate Acuity Identification Determine Appropriate Program Results of the clinical assessment as well as member's readiness determines the most appropriate program and intensity level Low acuity members may ultimately be assigned to any level of intervention. LOW Intervention MODERATE Intervention HIGH Intervention

21
Avoiding Costs per member/ per year Disease Management Success 0% 50% 100% Cardiac Disease $12,077 Following Physician’s Medication Regimen Asthma $1,340 Diabetes $12,672 Typical Compliance* NBH Program Compliance** 98% 50% *US food and Drug Administration Dept of Health and Human Services 2006 – AND– National Council on Patient Information and Education 2008 **Based on 2007 NBH operational outcomes

22
0-5510152025303540 Alcohol consumption <2 drinks / day Willing to make changes to improve health Blood pressure tested Cholesterol checked yearly Going to doctor Taking medication (compliance) Pneumonia vaccination in last 5 years Urine tested for protein (yearly) Flu Shot in last 12 months Feet examined yearly Eye exam yearly Understand diabetes and type Monitoring blood sugar Exercising 3 times/week Following a special diet Percent Change Program Measurement Behavior Changes for the Population
 Pneumonia vaccination in last 5 years Urine tested for protein (yearly) Flu Shot in last 12 months Feet examined yearly Eye exam yearly Understand diabetes and type Monitoring blood sugar Exercising 3 times/week Following a special diet Percent Change Program Measurement Behavior Changes for the Population")
23
52% 48% 70% HbA1c < 7HbA1c >= 7 Post DM HbA1c LevelPre DM HbA1c Level 30% HbA1c < 7 or Met Goal HbA1c >= 7 n = 593 n = 696 n = 899 n = 390 Program Measurement Clinical Changes for the Population

24
Diabetes HbA1c Level (%) Pre-Disease Management Post-Disease Management Target (< 7.0) 54%67% Suboptimal (≥ 7.0 and ≤ 8.0) 22%21% Poor Control (> 8.0 and ≤ 9.5) 15%10% Markedly Elevated (> 9.5) 9%2% Total 100% Asthma Coronary Artery Disease Hypertension *Excludes members with diabetes, CAD or CHF Outcomes Medication Compliance Pre-Disease Management Post-Disease Management Full Compliance 87%97% Partial Compliance 10% 2% Non-Compliance 3% 1% Total 100% LDL Cholesterol (mg/dL) Pre-Disease Management Post-Disease Management Target (< 100) 64%74% Suboptimal (100 - 129) 16% Poor Control (≥ 130) 20%10% Total 100% Blood Pressure (mmMg)* Pre-Disease Management Post-Disease Management Elevated BP 33%7% Controlled BP 67%93% Total 100%
 Pre-Disease Management Post-Disease Management Target (< 7.0) 54%67% Suboptimal (≥ 7.0 and ≤ 8.0) 22%21% Poor Control (> 8.0 and ≤ 9.5) 15%10% Markedly Elevated (> 9.5) 9%2% Total 100% Asthma Coronary Artery Disease Hypertension *Excludes members with diabetes, CAD or CHF Outcomes Medication Compliance Pre-Disease Management Post-Disease Management Full Compliance 87%97% Partial Compliance 10% 2% Non-Compliance 3% 1% Total 100% LDL Cholesterol (mg/dL) Pre-Disease Management Post-Disease Management Target (< 100) 64%74% Suboptimal ( ) 16% Poor Control (≥ 130) 20%10% Total 100% Blood Pressure (mmMg)* Pre-Disease Management Post-Disease Management Elevated BP 33%7% Controlled BP 67%93% Total 100%")
25
Maternity Program 14% 44% 1 st Trimester 3 rd Trimester 42% 2 nd Trimester Enrollment % by Trimester 46% 38% 1 st Trimester 3 rd Trimester 16% 2 nd Trimester High Risk & Very High Risk Designations by Trimester N=253 N=807 Dedicated maternity nurse Enroll All expectant mothers, starting in first trimester – not just ‘high risk’ as many programs do Extends through postpartum Same nurse manages all chronic and co-morbid conditions Differentiators: Source: 2007 NBH Outcomes

26
We reduce the average NICU length of stay by 21%. Average Savings: $51,099 Maternity Program NICU Results Results: For 2007, preterm birth rate is 10.6% (National average = 12.5%) NICU days per 1000: NBH has 1,302 days /1000 newborns Low birth weight and very low birth weight rate for NBH for 2007 is 7.7% (National average = 8.1%) NBH reports $8.8 million in savings for NICU admissions for 2007 Source: 2007 NBH Outcomes
 NICU days per 1000: NBH has 1,302 days /1000 newborns Low birth weight and very low birth weight rate for NBH for 2007 is 7.7% (National average = 8.1%) NBH reports $8.8 million in savings for NICU admissions for 2007 Source: 2007 NBH Outcomes.")
Similar presentations