Download presentation
Presentation is loading. Please wait.

1
Tuberculosis CAPT John Sanders CO, NMRC

2
2 Outline Importance of TB Clinical Overview of TB Active vs. Latent TB Active TB diagnosis and treatment LTBI diagnosis and treatment

3
3 Global Burden of Tuberculosis 9.2 million cases and 1.7 million deaths yearly Associated with co-pandemic of HIV Drug-resistance increasingly common 1/3 of the world’s population estimated to be infected with LTBI o Focus on identification and treatment of active TB (DOTS) o LTBI not a well-known concept outside the US o Increasing efforts to extend LTBI treatment to HIV populations
 o LTBI not a well-known concept outside the US o Increasing efforts to extend LTBI treatment to HIV populations")
5
Global Framework for Control The five-element WHO DOTS (Directly Observed Therapy, Short-course) strategy –Government commitment to TB control –Case detection among symptomatic patients –Standardized chemotherapy for all sputum smear-positive cases under proper case management conditions –Regular drug supply –Monitoring system for program supervision and evaluation The global incidence of (TB) peaked around 2003 and has been declining In 2010, 8.8 million individuals became ill (down from 9 mil in 2005) and 1.4 million died (down from 1.8 mil in 2003)
 strategy –Government commitment to TB control –Case detection among symptomatic patients –Standardized chemotherapy for all sputum smear-positive cases under proper case management conditions –Regular drug supply –Monitoring system for program supervision and evaluation The global incidence of (TB) peaked around 2003 and has been declining In 2010, 8.8 million individuals became ill (down from 9 mil in 2005) and 1.4 million died (down from 1.8 mil in 2003)")
7
7 TB Pathophysiology Spread person-to-person through the air Droplet nuclei may remain in the air Primary infection o Inhale tubercle bacilli o Reach alveoli, engulfed by macrophages o Some multiply intracellularly and released o Immune system (cell-mediated) prevents progression Activation o Tubercle bacilli overcome immune system o “5% risk in 2 years, 10% lifetime”
 prevents progression Activation o Tubercle bacilli overcome immune system o 5% risk in 2 years, 10% lifetime")
8
Active TB Chronic granulomatous infection caused by M. tuberculosis complex Contagious Lung disease is the most common manifestation (80%) Extrapulmonary (20%) –Lymphadenitis (scrofula) –Meningitis 8
 Extrapulmonary (20%) –Lymphadenitis (scrofula) –Meningitis 8.")
9
Symptoms of TB Fever Chronic cough Night sweats Hemoptysis Weight loss (unplanned) Fatigue 9
 Fatigue 9")
13
Diagnosis of Active TB Clinical symptoms and signs CXR (not confirmatory) AFB Smear (sensitivity 50%) Culture Nucleic Acid Amplification Tests (NAATs) 13
 AFB Smear (sensitivity 50%) Culture Nucleic Acid Amplification Tests (NAATs) 13")
14
CXR 14

15
AFB Smear 15

16
Treatment of Active TB “4 for 2 and 2 for 4” –INH, RIF, PYR, EMB X 2 months –INH, RIF X 4 months DOT is standard of care Check bacteriologic response monthly HIV test Drug susceptibility vs. adherence for persistent cases “Never add a single drug to a failing regimen” 16

17
When are they non-infectious? On adequate therapy Clinical response 3 consecutive negative sputum smears from sputum collected on different days 17

18
Infection Control Administrative controls –Primary strategy for infection control! ***** –“Develop policies and protocols to ensure the rapid identification, isolation, diagnostic evaluation, and treatment of persons likely to have TB” Engineering controls (ventilation) –Isolation –Negative pressure rooms Personal respiratory protection (N95) 18
 –Isolation –Negative pressure rooms Personal respiratory protection (N95) 18.")
19
HIV and TB 10% risk of progression per year Atypical presentations, anergy Leading cause of death in HIV patients MDR and XDR TB Drug interactions Reconstitution syndrome 19

20
MDR and XDR MDR=INH, RIF resistance XDR=MDR+ –Any fluoroquinolone; AND –1 of 3 injectable second line drugs Capreomycin Kanamycin Amikacin 20

21
21 LTBI vs. Pulmonary TB Disease Latent Tuberculosis Infection TST* or IGRA † positive Negative chest radiograph No symptoms or physical findings suggestive of TB disease Pulmonary TB Disease TST or IGRA usually positive Chest radiograph may be abnormal Symptoms may include one or more of the following: fever, cough, night sweats, weight loss, fatigue, hemoptysis, decreased appetite Respiratory specimens may be smear or culture positive –* Tuberculin Skin Test (TST) – † Interferon Gamma Release Assay (IGRA) are blood tests to detect M. tuberculosis infection.
 – † Interferon Gamma Release Assay (IGRA) are blood tests to detect M. tuberculosis infection..")
22
Diagnosis of Latent TB Two major tests for identification of latent tuberculosis infection: –The tuberculin skin test (TST) –The interferon gamma release assay (IGRA) Both tests evaluate cell-mediated immunity.
 –The interferon gamma release assay (IGRA) Both tests evaluate cell-mediated immunity.")
26
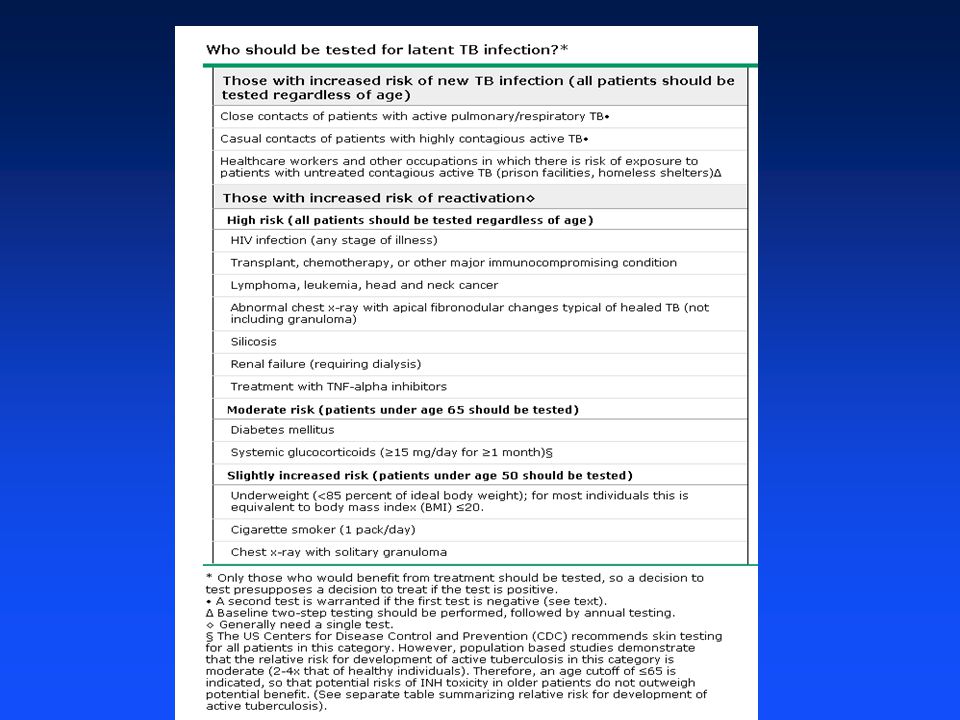
26 –CDC. MMWR 2000;49:1-51. –CDC MMWR 2004;53:683-686. –Note: includes patients taking TNF-α antagonists

27
27 –CDC. MMWR 2003;52:736.

28
900 mg (15 mg/kg) INH 900 mg Rifapentine (RPT) Weekly directly observed therapy (DOT) 12 week duration of therapy “Equal alternative to the 9 month INH regimen” Not recommended o Children < age 2 o HIV receiving ARTs o Pregnant women o INH or RIF resistance 28 INH/RPT DOT Regimen –CDC. MMWR 2011;60:1650-1653.

29
29 LTBI Treatment Myths Must be under 35 years old to treat o Liver disease is the more important factor Patients with BCG vaccination should not be treated o 10 mm or greater reaction should be considered for therapy regardless of BCG Serial liver enzyme tests should be performed for all LTBI patients o Liver enzymes are not routinely done (see next slides) o Clinical monitoring monthly 6 month therapy is the standard regimen o 9 months of INH (isoniazid) is the preferred regimen
 o Clinical monitoring monthly 6 month therapy is the standard regimen o 9 months of INH (isoniazid) is the preferred regimen")
30
30 Patient Instructions Rash Anorexia, nausea, vomiting, or abdominal pain in right upper quadrant Fatigue or weakness Dark urine Persistent numbness in hands or feet –No alcohol! –Instruct patient to report signs or symptoms of adverse drug reactions:

31
31 Monthly Clinical Monitoring Rationale for treatment Adherence with therapy Symptoms of adverse drug reactions Plans to continue treatment –Monthly visits should include a brief physical exam and a review of:

32
32 Baseline Laboratory Monitoring Baseline liver function tests (e.g., AST, ALT, and bilirubin) are not necessary except for patients with the following risk factors: HIV infection History of liver disease Alcoholism Pregnancy or in early postpartum period
 are not necessary except for patients with the following risk factors: HIV infection History of liver disease Alcoholism Pregnancy or in early postpartum period")
33
33 Continued Laboratory Monitoring Repeat laboratory monitoring if patient has: Abnormal baseline results Current or recent pregnancy High risk for adverse reactions Symptoms of adverse reaction Liver enlargement or tenderness during examination

34
34 Adverse Effects of Medications: Isoniazid (INH) 10-20% have elevated liver enzymes o Up to 5 times normal o Usually return to normal even if rx is continued Clinical hepatitis in 0.1% Peripheral neuropathy in 0.2% o More common with liver disease, diabetes o Rx with Vitamin B6 (Pyridoxine)
 10-20% have elevated liver enzymes o Up to 5 times normal o Usually return to normal even if rx is continued Clinical hepatitis in 0.1% Peripheral neuropathy in 0.2% o More common with liver disease, diabetes o Rx with Vitamin B6 (Pyridoxine)")
35
35 Adverse Effects of Medications: Rifampin (RIF) Hepatotoxicity in 0.6% Cutaneous reactions in 6% GI symptoms rarely severe Orange discoloration of body fluids Drug interactions (warfarin, OCPs, phenytoin) Contraindicated in HIV-infected individuals on certain PIs or NNRTIs o Substitute with Rifabutin
 Hepatotoxicity in 0.6% Cutaneous reactions in 6% GI symptoms rarely severe Orange discoloration of body fluids Drug interactions (warfarin, OCPs, phenytoin) Contraindicated in HIV-infected individuals on certain PIs or NNRTIs o Substitute with Rifabutin")
36
36 Adherence LTBI therapy not compulsory (active TB is) Adherence is abysmal (up to 50% complete therapy) o Therapeutic alliance o Don’t treat (or test!) low-risk patients Ways to improve adherence o Improve access for patient o Good information and education o 270 doses in 365 days for INH o Alternate regimens (intermittent, RIF) o Ensure continuity of care through PCS o Treat as soon as possible (during deployments, in basic training)
 Adherence is abysmal (up to 50% complete therapy) o Therapeutic alliance o Don’t treat (or test!) low-risk patients Ways to improve adherence o Improve access for patient o Good information and education o 270 doses in 365 days for INH o Alternate regimens (intermittent, RIF) o Ensure continuity of care through PCS o Treat as soon as possible (during deployments, in basic training)")
37
37 Who handles these cases? Civilian: public health/primary care partnership o Most county health departments offer therapy free of charge Military: Usually referred to Preventive Medicine o Can be ID, pulmonology, or primary care o Public health nurses usually do monthly clinical follow-up In the field (e.g. predeployment test is positive) o Many elect to defer therapy until after deployment o Depends on comfort level, available resources, and closeness of contact
 o Many elect to defer therapy until after deployment o Depends on comfort level, available resources, and closeness of contact.")
38
38 Other important management issues Directly observed therapy (DOT) o Standard of care for Active TB o May be used for LTBI, but uncommon o Refer to Preventive Medicine Disease reporting o Active TB is a reportable disease, LTBI is not o Positive TST or IGRA must be documented in an electronic registry (ALTHA, MEDPROS, etc) o Reportable diseases are reported to Preventive Medicine both in Garrison and Deployment
 o Standard of care for Active TB o May be used for LTBI, but uncommon o Refer to Preventive Medicine Disease reporting o Active TB is a reportable disease, LTBI is not o Positive TST or IGRA must be documented in an electronic registry (ALTHA, MEDPROS, etc) o Reportable diseases are reported to Preventive Medicine both in Garrison and Deployment")
Similar presentations












 is an infectious disease caused by the bacterium: “Mycobacterium tuberculosis”>")






>")






 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")