Download presentation
Presentation is loading. Please wait.

2
TREATMENT OF T.B. A special problem within the field of chemotherapy. A special problem within the field of chemotherapy.

3
TREATMENT OF T.B. Treatment is often complex and protracted. Treatment is often complex and protracted. Host immune defenses are often variable and inadequate. Host immune defenses are often variable and inadequate.

4
TREATMENT OF T.B. Chemotherapy is probably the keystone in the management of T.B. Chemotherapy is probably the keystone in the management of T.B. Ancillary treatments are used only in special circumstances. Ancillary treatments are used only in special circumstances.

6
TREATMENT OF T.B. Divided into chemoprophylaxis and treatment of active disease. Divided into chemoprophylaxis and treatment of active disease. Careful diagnostic studies must always precede therapy. Careful diagnostic studies must always precede therapy.

8
CHEMOPROPHYLAXIS To prevent clinically active disease in people already infected. To prevent clinically active disease in people already infected. Given only to those who will derive the greatest benefit and the least risk. Given only to those who will derive the greatest benefit and the least risk.

9
CHEMOPROPHYLAXIS Household contacts and close associates who have negative tuberculin tests. Household contacts and close associates who have negative tuberculin tests. Recent converters (preceding 2 yrs). Recent converters (preceding 2 yrs). Positive tuberculin test and underlying disease. Positive tuberculin test and underlying disease.
. Recent converters (preceding 2 yrs). Positive tuberculin test and underlying disease. Positive tuberculin test and underlying disease..")
10
CHEMOPROPHYLAXIS Positive tuberculin test and abnormal chest X-ray. Positive tuberculin test and abnormal chest X-ray. Positive test and under 30. Positive test and under 30. Immunosuppressed patients. Immunosuppressed patients.

11
CHEMOPROPHYLAXIS 300 mg Isoniazid once daily for 6-12 months. 300 mg Isoniazid once daily for 6-12 months.

12
TREATMENT OF ACTIVE T.B. First line drugs (used in the initial treatment of T.B.) : isoniazid, rifampin, streptomycin, ethambutol and pyrazinamide. First line drugs (used in the initial treatment of T.B.) : isoniazid, rifampin, streptomycin, ethambutol and pyrazinamide.
 : isoniazid, rifampin, streptomycin, ethambutol and pyrazinamide. First line drugs (used in the initial treatment of T.B.) : isoniazid, rifampin, streptomycin, ethambutol and pyrazinamide..")
13
TREATMENT OF ACTIVE T.B. Secondary agents: PAS, ethionamide, amikacin, kanamycin, capreomycin, cycloserine, ciprofloxacin, levofloxacin and clofazimine. Secondary agents: PAS, ethionamide, amikacin, kanamycin, capreomycin, cycloserine, ciprofloxacin, levofloxacin and clofazimine.

14
TREATMENT OF ACTIVE T.B. Therapy requires at least two effective drugs concurrently. Therapy requires at least two effective drugs concurrently.

15
TREATMENT OF ACTIVE T.B. If the treatment is appropriate improvement is usually seen within 2 weeks. If the treatment is appropriate improvement is usually seen within 2 weeks. Continue treatment for at least 3-6 mths after the sputum becomes negative. Continue treatment for at least 3-6 mths after the sputum becomes negative.

18
TREATMENT OF ACTIVE T.B. Never use 1 drug and never add a single drug to a failing regimen. Never use 1 drug and never add a single drug to a failing regimen.

19
TREATMENT OF ACTIVE T.B. Minimum length of therapy is 6-9 months. Minimum length of therapy is 6-9 months.

20
TREATMENT OF ACTIVE T.B. Initiation phase of 2 months. Initiation phase of 2 months. Continuation phase of 4-7 months. Continuation phase of 4-7 months.

21
TREATMENT OF ACTIVE T.B. Initial therapy is a 4 drug regimen of INH, rifampin, pyrazinamide and ethambutol. Initial therapy is a 4 drug regimen of INH, rifampin, pyrazinamide and ethambutol. For patients with drug-susceptible disease the pyrazinamide can be discontinued after 2 months. For patients with drug-susceptible disease the pyrazinamide can be discontinued after 2 months. Ethambutol can also be discontinued. Ethambutol can also be discontinued.

22
TREATMENT OF ACTIVE T.B. Combining daily therapy with intermittent therapy. Combining daily therapy with intermittent therapy.

23
INTERMITTENT THERAPY Daily therapy for 2 weeks (INH, rifampin, pyrazinamide and streptomycin) followed by therapy 2 times a week for six weeks. Then INH + Rifampin 2x weekly for 16 weeks. Daily therapy for 2 weeks (INH, rifampin, pyrazinamide and streptomycin) followed by therapy 2 times a week for six weeks. Then INH + Rifampin 2x weekly for 16 weeks.
 followed by therapy 2 times a week for six weeks. Then INH + Rifampin 2x weekly for 16 weeks..")
24
DOT

25
DIRECTLY OBSERVED THERAPY (DOT) DIRECTLY OBSERVED THERAPY (DOT) Now recommended for all patients. Now recommended for all patients.

26
DRUG RESISTANCE Major cause is inadequate therapy. Major cause is inadequate therapy. Treatment is difficult and requires good laboratory support and experience with the less frequently used drugs. Treatment is difficult and requires good laboratory support and experience with the less frequently used drugs.

27
MULTIPLE DRUG RESISTANT T.B. Combined resistance to at least INH and rifampin. Combined resistance to at least INH and rifampin. Caused by improper treatment, inadequate drug supplies, or poor patient supervision. Caused by improper treatment, inadequate drug supplies, or poor patient supervision.

28
MULTIPLE DRUG RESISTANT T.B. Patients face chronic disability and death and represent an infectious hazard for the community. Patients face chronic disability and death and represent an infectious hazard for the community.

29
MULTIPLE DRUG RESISTANT T.B. High cure rates have been obtained but require prompt recognition, rapid and accurate susceptibility results and early administration of an individualized retreatment regimen. High cure rates have been obtained but require prompt recognition, rapid and accurate susceptibility results and early administration of an individualized retreatment regimen.

30
MULTIPLE DRUG RESISTANT T.B. Regimens are usually based on a quinolone and an injectable agent (e.g.aminoglycoside) supplemented with other second line drugs. Regimens are usually based on a quinolone and an injectable agent (e.g.aminoglycoside) supplemented with other second line drugs.
 supplemented with other second line drugs. Regimens are usually based on a quinolone and an injectable agent (e.g.aminoglycoside) supplemented with other second line drugs..")
31
MULTIPLE DRUG RESISTANT T.B. DOT is crucial. DOT is crucial. Therapy is often prolonged (24 mths.), expensive and has multiple adverse effects. Therapy is often prolonged (24 mths.), expensive and has multiple adverse effects. Prevention is therefore very important. Prevention is therefore very important.
, expensive and has multiple adverse effects. Therapy is often prolonged (24 mths.), expensive and has multiple adverse effects. Prevention is therefore very important. Prevention is therefore very important..")
32
TREATMENT OF HIV- RELATED TB Possibility of increased drug toxicity and possible drug-drug interactions (rifamycins plus PI and/or NNRI). Possibility of increased drug toxicity and possible drug-drug interactions (rifamycins plus PI and/or NNRI).
..")
33
NONTUBERCULOUS MYCOBACTERIA Atypical mycobacterial infections. Atypical mycobacterial infections. Resistant to many of the commonly used drugs. Resistant to many of the commonly used drugs. Examine for sensitivity and treat on this basis. Examine for sensitivity and treat on this basis. Increased in AIDS (e.g. MAC). Increased in AIDS (e.g. MAC).
. Increased in AIDS (e.g. MAC)..")
34
MECHANISM OF ACTION OF ANTITUBERCULOSIS AGENTS Drugs which interfere with mycolic acid synthesis Drugs which interfere with mycolic acid synthesis Drugs which inhibit nucleic acid synthesis Drugs which inhibit nucleic acid synthesis Drugs inhibiting protein synthesis Drugs inhibiting protein synthesis

35
respiratory-research.com/.ETH

36
Peptidoglycan Porin Arabinogalactan Mycolic Acid Lipid of intermediate length Lipid with C14-C18 acids MYCOBACTERIAL CELL WALL

37
ISONIAZID-MECHANISM OF ACTION Interferes with biosynthesis of cell wall mycolic acids. Interferes with biosynthesis of cell wall mycolic acids. Mycolate depleted cell walls are structurally weak. Mycolate depleted cell walls are structurally weak.

38
Isoniazid(Prodrug) Active Form Catalase/Peroxidase katG
 Active Form Catalase/Peroxidase katG")
39
INH MECHANISM OF ACTION InhA gene encodes an enoyl-ACP reductase of fatty acid synthase II which converts 2 -unsaturated to saturated fatty acids on the pathway to mycolic acid biosynthesis. InhA gene encodes an enoyl-ACP reductase of fatty acid synthase II which converts 2 -unsaturated to saturated fatty acids on the pathway to mycolic acid biosynthesis. Activated INH inhibits this enzyme. Activated INH inhibits this enzyme.

40
Peptidoglycan Porin Arabinogalactan Mycolic Acid Lipid of intermediate length Lipid with C14-C18 acids Mycobacterial Cell Wall INH

41
RESISTANCE Mutations in the katG gene can lead to loss of catalase-peroxidase activity. Mutations in the katG gene can lead to loss of catalase-peroxidase activity. Resistance also maps to mutations in four other genes including inhA Resistance also maps to mutations in four other genes including inhA

42
RESISTANCE Overall incidence of resistance is higher in certain ethnic groups such as African Americans, Mexican Americans and Indochinese refugees. Overall incidence of resistance is higher in certain ethnic groups such as African Americans, Mexican Americans and Indochinese refugees.

43
ETHAMBUTOL-MECHANISM OF ACTION It is not bactericidal. It is not bactericidal. Inhibits synthesis of the mycobacterial cell wall. Inhibits synthesis of the mycobacterial cell wall.

44
MECHANISM OF ACTION It is an inhibitor of mycobacterial arabinosyl transferases (encoded by the embAB genes). It is an inhibitor of mycobacterial arabinosyl transferases (encoded by the embAB genes). Arabinoglycan an essential component of the cell wall. Arabinoglycan an essential component of the cell wall.
. Arabinoglycan an essential component of the cell wall. Arabinoglycan an essential component of the cell wall..")
45
Peptidoglycan Porin Arabinogalactan Mycolic Acid Lipid of intermediate length Lipid with C14-C18 acids MYCOBACTERIAL CELL WALL Ethambutol

46
RESISTANCE Mutations in the emb genes. Mutations in the emb genes.

47
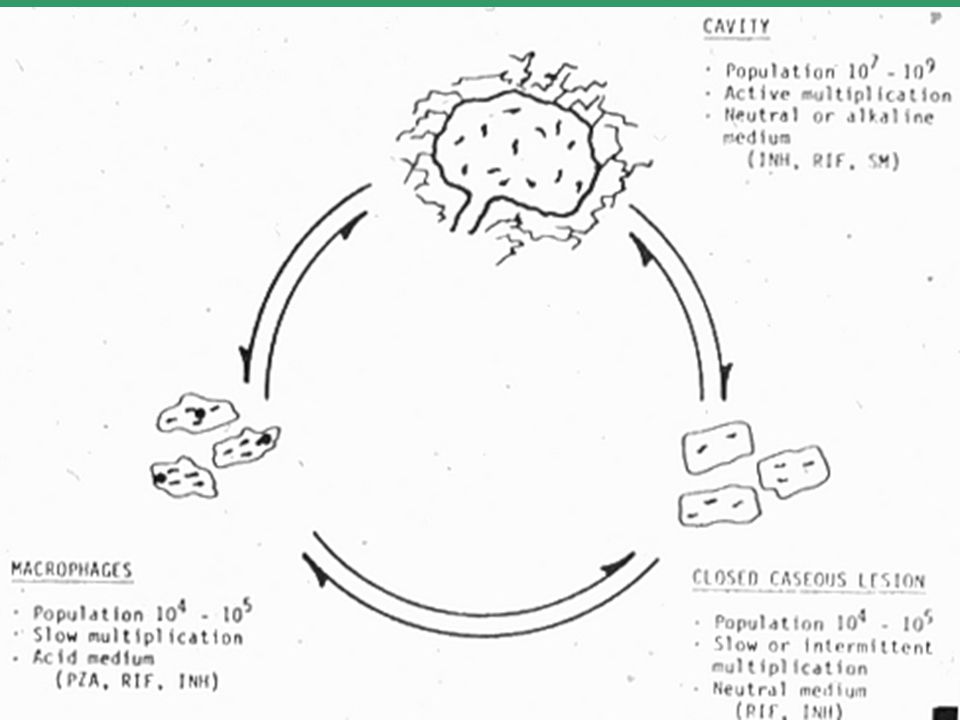
PYRAZINAMIDE-MECHANISM OF ACTION PZA PZA POA (pyrazinoic acid) pyrazinamidase Occurs mostly in the liver.
 pyrazinamidase Occurs mostly in the liver.")
48
MECHANISM OF ACTION Inhibits fatty acid synthetase I of Mycobacterium tuberculosis. Inhibits fatty acid synthetase I of Mycobacterium tuberculosis.

49
Short chain fatty acid precursors Pyrazinamide

50
RESISTANCE Mutations in the pncA gene which results in impairment in the conversion of PZA to its active form. Mutations in the pncA gene which results in impairment in the conversion of PZA to its active form.

51
DRUGS INHIBITING NUCLEIC ACID SYNTHESIS Rifampin Rifampin

52
respiratory-research.com/.ETH

53
RESISTANCE Results from an alteration in the polymerase enzyme (mutation in the rpoB gene). Results from an alteration in the polymerase enzyme (mutation in the rpoB gene).
..")
54
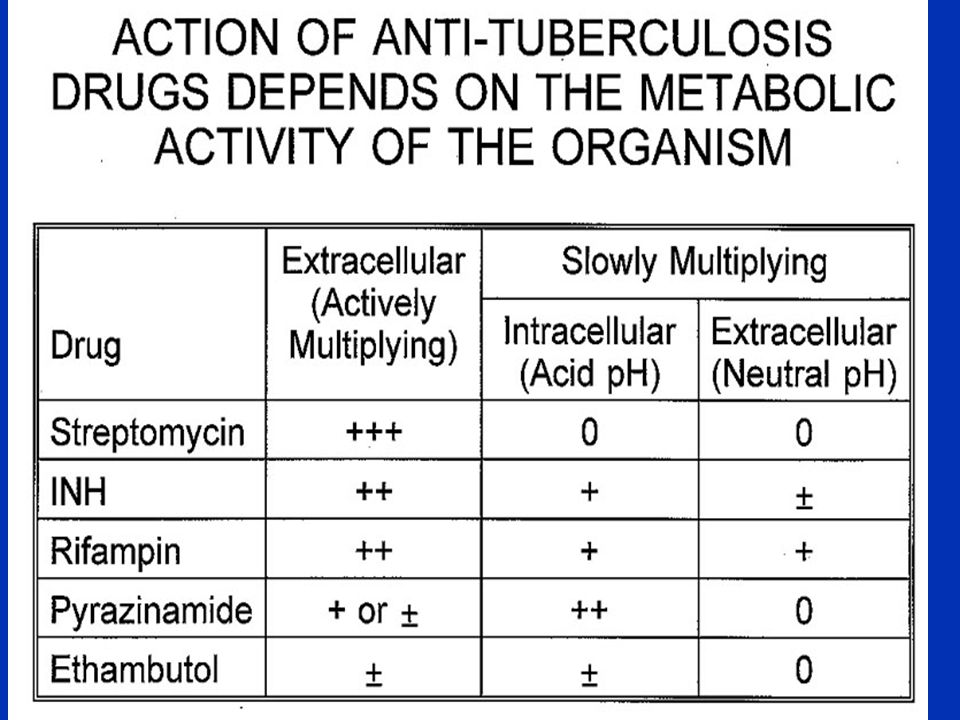
STREPTOMYCIN-ANTI TB ACTIVITY Most strains of M.Tuberculosis are sensitive. Most strains of M.Tuberculosis are sensitive. Bactericidal only against the extracellular tuberculosis bacilli. Bactericidal only against the extracellular tuberculosis bacilli. Overall only suppressive. Overall only suppressive.

55
RESISTANCE Major problem with streptomycin use in T.B. Major problem with streptomycin use in T.B. Combination therapy will delay or prevent resistance. Combination therapy will delay or prevent resistance.

56
THERAPEUTIC USES IN T.B. It is used in drug resistant disease. It is used in drug resistant disease. More serious forms of T.B. (disseminated T.B. or meningitis). More serious forms of T.B. (disseminated T.B. or meningitis).
. More serious forms of T.B. (disseminated T.B. or meningitis)..")
57
N C NH 2 o C o N ISONIAZID NICOTINAMIDE N C OH o NICOTINICACID o C NHNH 2

58
ANTITUBERCULAR ACTIVITY Bactericidal vs actively growing tubercle bacilli. Bactericidal vs actively growing tubercle bacilli. Also bactericidal vs intracellular bacteria. Also bactericidal vs intracellular bacteria. Poor activity against atypical organisms. Poor activity against atypical organisms.

59
ABSORPTION AND DISTRIBUTION Readily absorbed when given orally or parenterally (food and Al +++ decrease absorption). Readily absorbed when given orally or parenterally (food and Al +++ decrease absorption). INH diffuses well into all body fluids and cells including the CNS. INH diffuses well into all body fluids and cells including the CNS.
. INH diffuses well into all body fluids and cells including the CNS. INH diffuses well into all body fluids and cells including the CNS..")
60
DISTRIBUTION Penetrates cells with ease and is effective against organisms growing within cells. Penetrates cells with ease and is effective against organisms growing within cells.

61
METABOLISM Primary route is by acetylation. Primary route is by acetylation. Genetic heterogeneity with regard to the rate of acetylation. There are “slow” and “rapid” acetylators. Genetic heterogeneity with regard to the rate of acetylation. There are “slow” and “rapid” acetylators. Among American and northern European pops. 50-65% are slow acetylators. Among American and northern European pops. 50-65% are slow acetylators.

62
METABOLISM Rapid acetylation is an autosomal dominant trait. Rapid acetylation is an autosomal dominant trait.

63
METABOLISM More rapid clearance of INH by rapid acetylators is of no therapeutic consequence when given daily. More rapid clearance of INH by rapid acetylators is of no therapeutic consequence when given daily. Subtherapeutic concn’s may occur if INH is given to rapid acetylators as a once-weekly dose. Subtherapeutic concn’s may occur if INH is given to rapid acetylators as a once-weekly dose.

64
METABOLISM Slow acetylators may be more susceptible to toxic side effects related to higher blood levels of INH whereas rapid acetylators have a higher frequency of hepatotoxicity. Slow acetylators may be more susceptible to toxic side effects related to higher blood levels of INH whereas rapid acetylators have a higher frequency of hepatotoxicity.

65
Isoniazid Peripheral Neuropathy Acute Seizures Hydrazine Acetyl INH Isonicotinic Acid Acetyl Hydrazine Diacetyl Hydrazine (nontoxic) (nontoxic) Reactive Metabolite Hepatic Necrosis Acetylated Acetylated Hydrolyzed MicrosomalOxidation MicrosomalOxidation (nontoxic)
 (nontoxic) Reactive Metabolite Hepatic Necrosis Acetylated Acetylated Hydrolyzed MicrosomalOxidation MicrosomalOxidation (nontoxic)")
66
EXCRETION 75-95% of a dose is excreted in the urine in 24 hrs., mostly as metabolites. 75-95% of a dose is excreted in the urine in 24 hrs., mostly as metabolites.

67
THERAPEUTIC STATUS Most important drug for all types of T.B. Most important drug for all types of T.B. Chemoprophylaxis. Chemoprophylaxis.

68
CONTRAINDICATIONS Liver disease Liver disease

69
DRUG INTERACTIONS Aluminum salts. Aluminum salts. INH inhibits cytochrome P-450 enzymes. INH inhibits cytochrome P-450 enzymes. INH is a potential inhibitor of MAO and diamine oxidase (histaminase). INH is a potential inhibitor of MAO and diamine oxidase (histaminase). Induces Cytochrome P4502E1 (acetaminophen). Induces Cytochrome P4502E1 (acetaminophen).
. INH is a potential inhibitor of MAO and diamine oxidase (histaminase). Induces Cytochrome P4502E1 (acetaminophen). Induces Cytochrome P4502E1 (acetaminophen)..")
70
ETHAMBUTOL- ANTIMICROBIAL ACTIVITY Nearly all strains of Mycobacterium tuberculosis are sensitive. Nearly all strains of Mycobacterium tuberculosis are sensitive. A few atypical organisms are also sensitive (MAC). A few atypical organisms are also sensitive (MAC).
. A few atypical organisms are also sensitive (MAC)..")
71
PHARMACOKINETICS Well absorbed from the GI Tract. Well absorbed from the GI Tract. Mostly excreted unchanged in the urine. Mostly excreted unchanged in the urine.

72
THERAPEUTIC STATUS Initial treatment of TB. Initial treatment of TB. Used to treat MAC infections in certain combinations. Used to treat MAC infections in certain combinations.

73
RIFAMPIN (Rifampicin) Semi-synthetic derivative of one of the rifamycins, a group of complex macrocyclic antibiotics. Semi-synthetic derivative of one of the rifamycins, a group of complex macrocyclic antibiotics.

74
RIFAMPIN-ANTI T.B. ACTIVITY Mycobacterium tuberculosis as well as several atypical organisms. Mycobacterium tuberculosis as well as several atypical organisms. Bactericidal against extracellular cavitary bacilli and to organisms in closed lesions. Bactericidal against extracellular cavitary bacilli and to organisms in closed lesions. Some non-Mycobacterial bacteria and some viruses. Some non-Mycobacterial bacteria and some viruses.

75
PHARMACOKINETICS Well absorbed from the GI tract. Well absorbed from the GI tract. Widely distributed throughout the body including the CNS. Widely distributed throughout the body including the CNS.

76
Rifampin Rifampin Deacetylation

77
PHARMACOKINETICS Induces its own metabolism. Induces its own metabolism. About 1/3 of the drug is excreted in urine, and 2/3 in the intestine. About 1/3 of the drug is excreted in urine, and 2/3 in the intestine. Adjust dose with decreased liver function. Adjust dose with decreased liver function.

78
THERAPEUTIC STATUS Used in combination with INH for the initial treatment of T.B., in the retreatment of T.B. and in intermittent therapy. Used in combination with INH for the initial treatment of T.B., in the retreatment of T.B. and in intermittent therapy.

79
THERAPEUTIC STATUS Possible alternative to INH to prevent T.B (with pyrazinamide)? Possible alternative to INH to prevent T.B (with pyrazinamide)? Used to treat atypical mycobacterial infections. Used to treat atypical mycobacterial infections.
. Used to treat atypical mycobacterial infections. Used to treat atypical mycobacterial infections..")
80
Protease inhibitors Azoles

81
RIFAPENTINE AND RIFABUTIN Rifabutin-better activity vs MAC than rifampin; less an inducer of cytochrome P-450 enzymes Rifabutin-better activity vs MAC than rifampin; less an inducer of cytochrome P-450 enzymes Rifapentine-long acting analog. Rifapentine-long acting analog.

82
N C NH 2 o N C o N C o N OH PYRAZINAMIDE NICOTINAMIDE PYRAZINOIC ACID N

83
ANTIBACTERIAL ACTIVITY Eliminates bacilli that are growing at slightly acidic pH. Eliminates bacilli that are growing at slightly acidic pH.

84
PHARMACOKINETICS Well absorbed from the GI tract. Well absorbed from the GI tract. Excreted primarily through the kidney. Excreted primarily through the kidney.

85
THERAPEUTIC USES Important component of short-term (6 month) multiple-drug therapy of TB. Important component of short-term (6 month) multiple-drug therapy of TB. Preventative therapy in combination with rifampin when INH resistance is suspected. Preventative therapy in combination with rifampin when INH resistance is suspected.
 multiple-drug therapy of TB. Preventative therapy in combination with rifampin when INH resistance is suspected. Preventative therapy in combination with rifampin when INH resistance is suspected..")
86
FIXED-DOSE COMBINATIONS They are strongly encouraged for adults who are self-administering their medications. They are strongly encouraged for adults who are self-administering their medications. Enhance adherence, may reduce inappropriate monotherapy and may prevent drug resistance. Enhance adherence, may reduce inappropriate monotherapy and may prevent drug resistance.

87
FIXED-DOSE COMBINATIONS Fixed-dose combinations are available as Rifamate (INH +rifampin) and Rifater (INH +rifampin +pyrazinamide). Fixed-dose combinations are available as Rifamate (INH +rifampin) and Rifater (INH +rifampin +pyrazinamide).
 and Rifater (INH +rifampin +pyrazinamide)..")
88
ADVERSE EFFECTS OF ANTITUBERCULOSIS DRUGS

89
GI DISTRESS AND UPSET Most anti TB drugs are irritating to the GI tract-INH, rifampin, pyrazinamide Most anti TB drugs are irritating to the GI tract-INH, rifampin, pyrazinamide

90
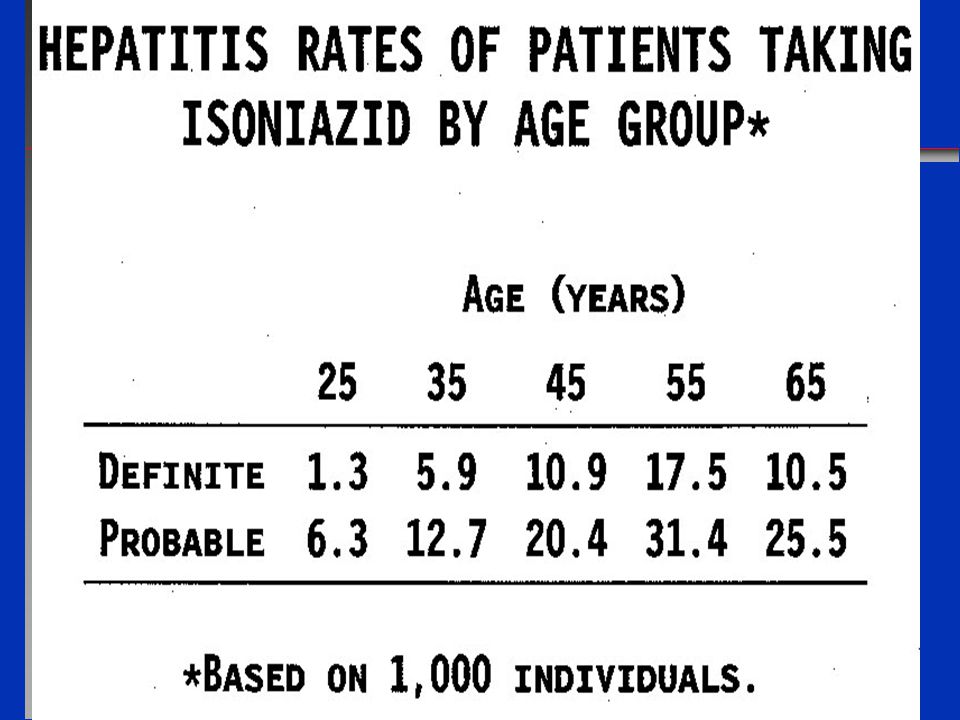
ISONIAZID-HEPATOTOXICITY

91
Liver enzymes

92
HEPATOTOXICITY Hepatitis is the most severe toxicity. Hepatitis is the most severe toxicity.

95
Isoniazid Peripheral Neuropathy Acute Seizures Hydrazine Acetyl INH Isonicotinic Acid Acetyl Hydrazine Diacetyl Hydrazine (nontoxic) (nontoxic) Reactive Metabolite Hepatic Necrosis Acetylated Acetylated Hydrolyzed MicrosomalOxidation MicrosomalOxidation (nontoxic)
 (nontoxic) Reactive Metabolite Hepatic Necrosis Acetylated Acetylated Hydrolyzed MicrosomalOxidation MicrosomalOxidation (nontoxic)")
96
RIFAMPIN Jaundice Jaundice

97
PYRAZINAMIDE Hepatotoxicity is common and can be serious Hepatotoxicity is common and can be serious

98
NEUROTOXICITY

99
NEUROTOXICITY Peripheral neuritis is common (without pyridoxine). Peripheral neuritis is common (without pyridoxine). CNS effects of various types can occur (convulsions,ataxia). CNS effects of various types can occur (convulsions,ataxia).
. CNS effects of various types can occur (convulsions,ataxia). CNS effects of various types can occur (convulsions,ataxia)..")
100
OCULAR TOXICITY

101
ETHAMBUTOL Optic Neuritis and color blindness. Optic Neuritis and color blindness. Base-line and monthly vision tests. Base-line and monthly vision tests.

102
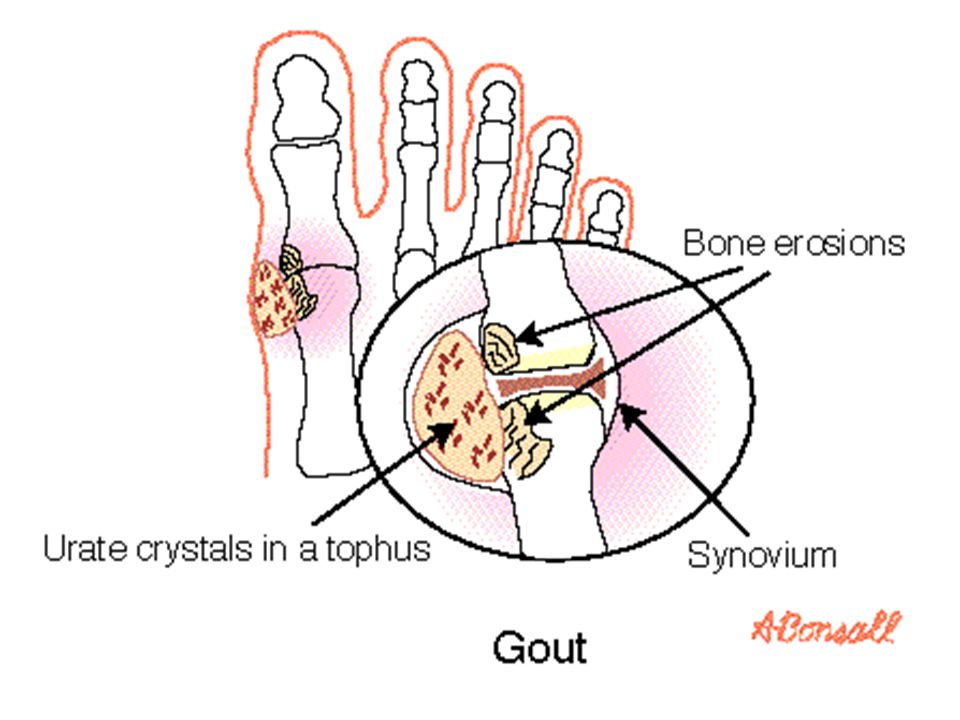
HYPERURICEMIA Pyrazinamide Pyrazinamide

104
HIGH DOSE INTERMITTENT THERAPY Additional toxicities especially with rifampin Additional toxicities especially with rifampin

105
ADVERSE EFFECTS Orange - pink color is imparted to saliva, tears and other body fluids. Orange - pink color is imparted to saliva, tears and other body fluids.

Similar presentations



, M. Sc. In Pharm (Pharmacology)>")














 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")
>")

 effects. Hepatitis.>")
