Download presentation
Presentation is loading. Please wait.

1
IRON 7 mg/1000 cal in diet; 10% absorbed Heme iron absorbed best, Fe 2+ much better than Fe 3+ –Some foods, drugs enhance and some inhibit absorption of ionic iron –Ability to regulate absorption limited Absorption in proximal small intestine Absorption greater if there is erythroid hyperplasia or hypoxia

2
N Engl J Med 2004;350:2383 Regulation of iron uptake and storage. Hepcidin, a peptide produced in the liver, is a key regulator of iron release from villus enterocytes and macrophages. Hepcidin, whose production is upregulated by high plasma iron levels or inflammation, inhibits iron release from these cells and lowers GI absorption. Low iron levels decrease hepcidin production, which in turn stimulates iron absorption and release into the blood. The HFE gene modulates hepcidin production. Mutations in HFE can cause diminished hepcidin release, and can eventually cause iron overload (hereditary hemochromatosis).
..")
3
1 cc of red cells contains about 1 mg iron 1 cc of whole blood contains 0.5 mg iron

4
IRON BALANCE 1-2 mg/day lost via desquamation, GI blood loss in adult Negative iron balance possible in early childhood Menstruation, pregnancy, lactation promote negative balance Positive balance (and eventual iron overload) can occur in inherited disorders (hemochromatosis), or as a result of repeated blood transfusions
 can occur in inherited disorders (hemochromatosis), or as a result of repeated blood transfusions")
5
♂ ♀

8
N Engl J Med 2004;350:2383 Plasma levels of iron are closely regulated to ensure a daily supply of about 20 mg to the bone marrow for incorporation into hemoglobin. Most of the iron in the plasma derives from the continuous breakdown of hemoglobin in senescent red cells by macrophages. 1 to 2 mg per day of iron is also taken up by duodenal enterocytes and transferred to the plasma compartment or, depending on body needs, stored in the enterocytes as ferritin. These stores are eliminated when enterocytes are sloughed at the end of their life cycles; apart from menstrual blood loss, this is the only significant means by which excess body iron is excreted. Iron recycled by macrophages and that absorbed from the gut is loaded onto serum transferrin and delivered primarily to the bone marrow for reincorporation into new red-cell precursors. The remaining body iron (about 1000 mg) is stored, primarily in hepatocytes.
 is stored, primarily in hepatocytes..")
9
IRON TRANSPORT AND STORAGE Absorbed iron oxidized to Fe 3+ form Bound tightly to transferrin in blood –Transferrin = total iron binding capacity (TIBC) –Normally serum iron about 100 μg/dl, TIBC about 300 μg/dl Iron transferred to cells and reduced to Fe 2+ form, then inserted into heme or stored Storage iron (Fe 3+ ) bound to ferritin –Hemosiderin is denatured ferritin –Small amount of ferritin in blood (nanograms)
 –Normally serum iron about 100 μg/dl, TIBC about 300 μg/dl Iron transferred to cells and reduced to Fe 2+ form, then inserted into heme or stored Storage iron (Fe 3+ ) bound to ferritin –Hemosiderin is denatured ferritin –Small amount of ferritin in blood (nanograms)")
11
ASSESSMENT OF BODY IRON Serum iron low in iron deficiency, inflammation TIBC high in iron deficiency, normal or low in inflammation Ferritin low in iron deficiency, increases in inflammation Marrow iron stores absent in iron deficiency Combination of iron deficiency and inflammation makes assessing iron stores difficult

13
TESTS OF IRON STATUS TESTS OF IRON STATUS Practical aspects Low serum ferritin almost always indicates iron deficiency Low serum iron and high TIBC almost always indicate iron deficiency Ferritin > 100 rarely found in iron deficiency –Exception - liver inflammation/necrosis Normal serum iron rarely found in iron deficiency –Exception - iron deficiency recently treated with oral iron When TIBC is low or normal, low serum iron not a reliable indicator of iron deficiency Iron deficiency may be hard to diagnose via blood tests in setting of inflammation (eg, low iron, low TIBC, intermediate ferritin level) –Therapeutic trial of iron +/- EPO a reasonable alternative to marrow biopsy
 –Therapeutic trial of iron +/- EPO a reasonable alternative to marrow biopsy")
14
HYPOPROLIFERATIVE ANEMIA Lower than expected red cell production (erythroid cells in marrow and reticulocytes) for degree of anemia
 for degree of anemia")
15
HYPOPROLIFERATIVE ANEMIA Causes and examples Insufficient iron for hemoglobin synthesis –Iron deficiency Diminished iron release from storage sites –Inflammation Blunted or impaired erythropoietin production –Inflammation, renal failure Inhibition of red cell progenitor proliferation by cytokines –Inflammation Marrow damage –Aplastic anemia, myelophthisic disease

16
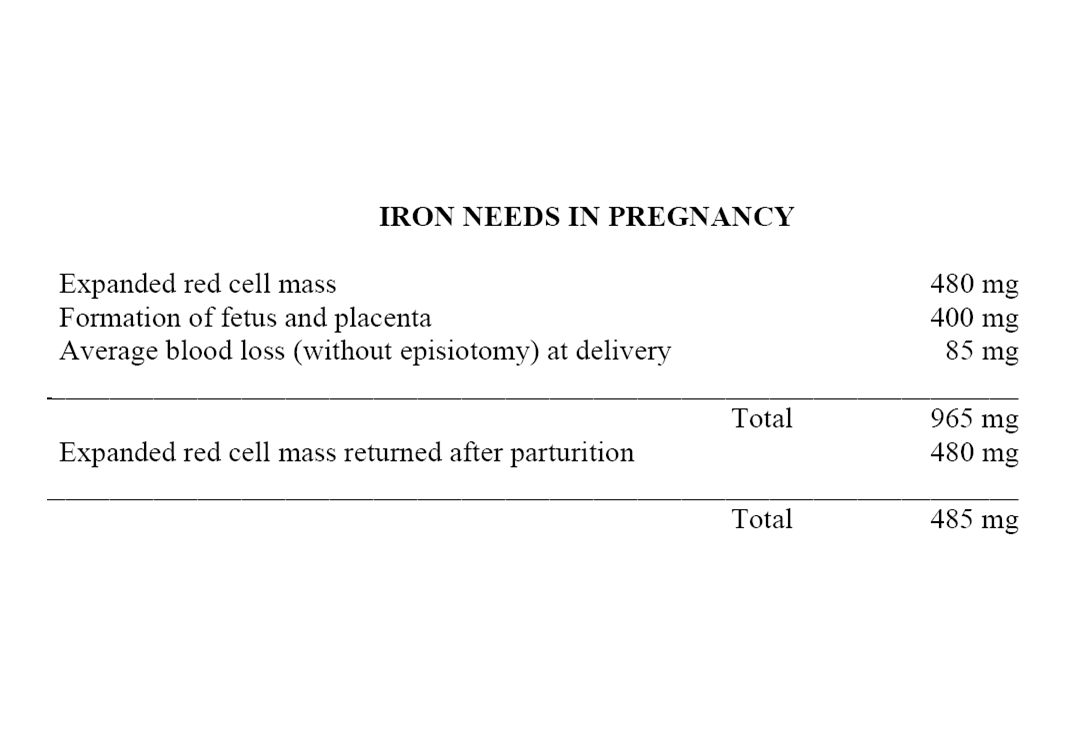
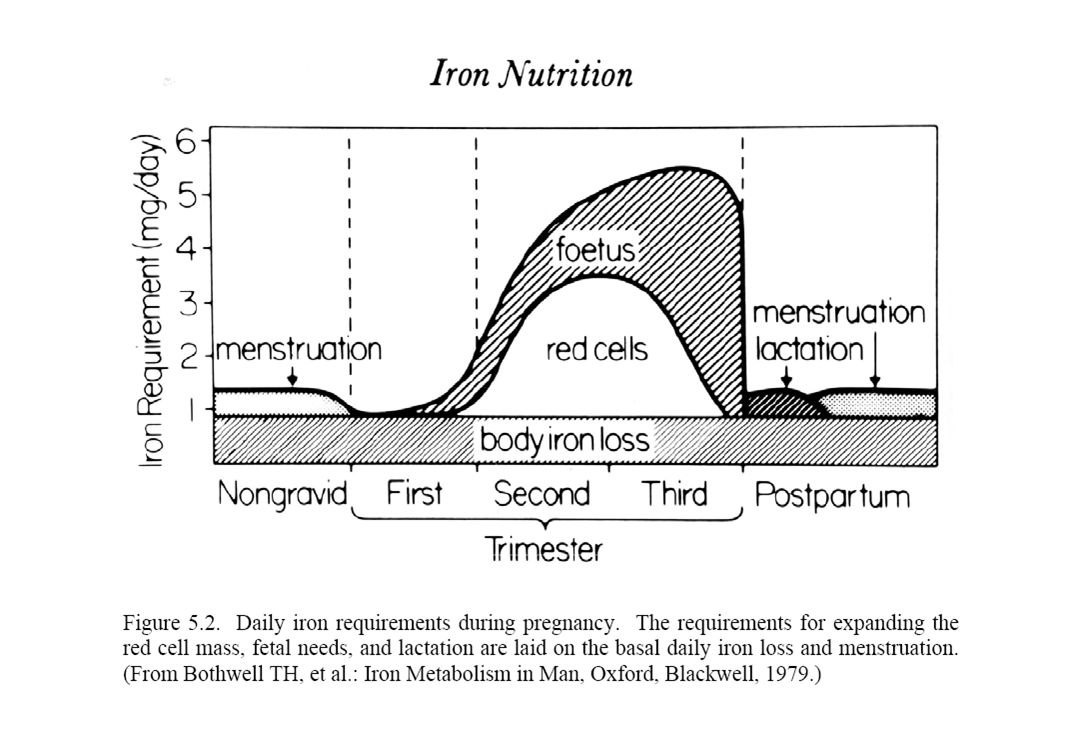
IRON DEFICIENCY Most common cause of anemia Usually due to chronic blood loss –Exceptions: rapidly growing child, malabsorption In young women this is usually due to menstrual blood loss pregnancy In anyone else must rule out GI blood loss –Esophageal disease, hiatal hernia, ulcer, inflammatory bowel disease, angiodysplasia, hemorrhoids, cancer

18
Atrophic glossitis “Spoon nails” Iron deficiency

19
Absent iron storesNormal iron stores

20
IRON DEFICIENCY ANEMIA Treatment Oral ferrous salts –Some patients have GI side effects Oral iron-polysaccharide complex IV iron dextran –If oral iron not absorbed or not tolerated –Slight risk of anaphylaxis Should see increased hemoglobin within 2-3 weeks

21
IRON OVERLOAD Hereditary hemochromatosis –Autosomal recessive, HFE gene; genotype common but low penetrance Other inherited disorders –Mutations in other genes that regulate iron metabolism –Africans, African-Americans Chronic ineffective erythropoiesis –Thalassemia Repeated transfusion –Toxicity after about 100 Units

22
IRON OVERLOAD Increased serum iron and high transferrin saturation (90%+ in hemochromatosis) Very high serum ferritin Increased liver and marrow iron –Quantitation of liver iron best indicator of severity DNA test available for hereditary HC
 Very high serum ferritin Increased liver and marrow iron –Quantitation of liver iron best indicator of severity DNA test available for hereditary HC")
23
IRON OVERLOAD Clinical consequences Cirrhosis, hepatocellular carcinoma Cardiomyopathy, heart failure Endocrine failure (esp diabetes) Arthropathy Treatment of hereditary HC by phlebotomy prevents these problems and can reverse early tissue damage
 Arthropathy Treatment of hereditary HC by phlebotomy prevents these problems and can reverse early tissue damage")
Similar presentations




>")
/ HYPOCHROMIC &/or (NORMO)/ MICROCYTIC ANEMIAS 1. Disorders of iron utilization a. iron deficiency b. anemia of.>")
















