Download presentation
Presentation is loading. Please wait.

24
Let’s review

25
Regulation of Acid-Base Balance Buffering systems neutralize acids & bases & include lungs & renals Buffer—substance or a group of substances that can absorb or release H+ to correct an acid- base imbalance Arterial pH indirect measurement of H+ ion

26
Regulation of Acid-Base Balance pH reflection of balance between CO2 (lungs) & HCO3- (renal) Acidosis –Increased amount of H+ ions –Normal pH 7.35-7.45 –pH = 7 is neutral –pH < 7 is acid –pH > 7 is alkaline
 & HCO3- (renal) Acidosis –Increased amount of H+ ions –Normal pH –pH = 7 is neutral –pH < 7 is acid –pH > 7 is alkaline")
27
Regulation of Acid-Base Balance AB balance exists when the rate at which the body produces acid or bases = the rate at which the acids or bases are excreted Normal hydrogen ion level is necessary to maintain cell membrane integrity & speed of cellular enzymatic actions

28
Acid-Base Regulators Chemical regulation –Largest chemical buffer in ECF is carbonic acid/bicarb buffer system –First buffer system to react –Reacts in seconds –Lungs control excretion of carbon dioxide

29
Acid-Base Regulators Kidneys control excretion of hydrogen & bicarbonate ions ECF becomes more acidic pH decreases ECF receives more base substances, pH rises

30
Acid-Base Regulators Biological Regulation –Occurs after chemical buffering –Occurs hydrogen ions are absorbed or released by cells –Hydrogen ion + charged & must be exchanged with another + charged ion—frequently K+ Conditions that produce excess acid H+ ion enter cell potassium ion leaves cell enters ECF elevated K+ levels

31
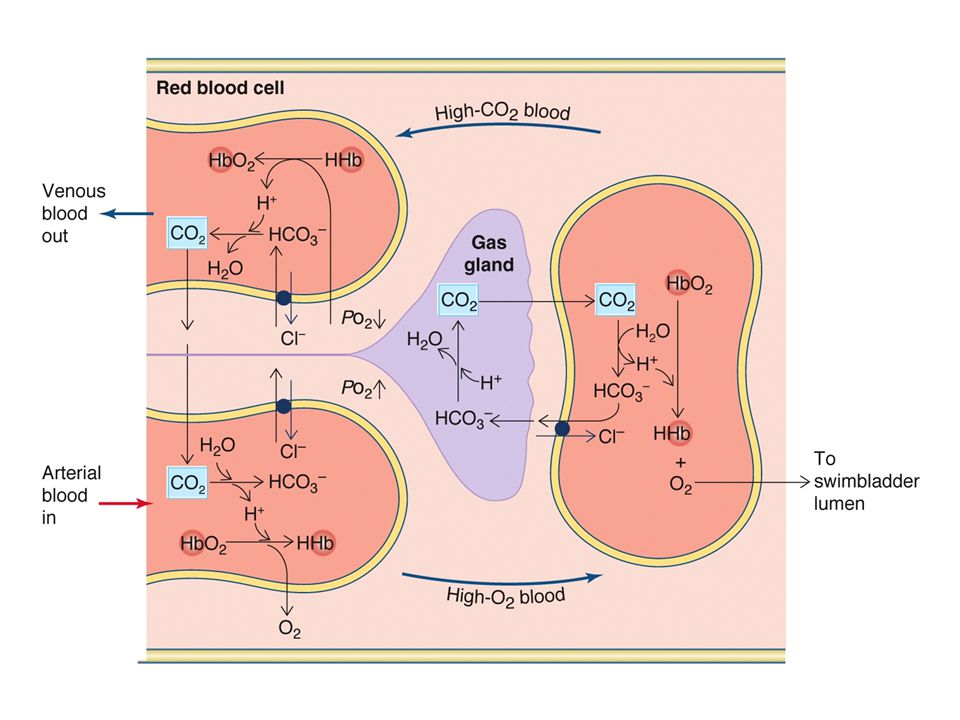
Acid-Base Regulators Biological buffer –Hemoglobin- oxyhemoglobin system –CO2 diffuses to RBC forms carbonic acid dissociates to H+ & HCO3+ ions H+ ions attach to hemoglobin HCO3+ available for buffering Chloride shift in RBCs –Bld oxygenated in lungs, bicarb diffuses into cell chloride travels from hemoglobin to plasma to maintain electrical neutrality

32
Acid-Base Regulators Physiological regulation –Lungs & kidneys –If diseased is no longer effective for regulation –Lungs adapt rapidly to imbalance –Increased H+ & CO2 ions stimulate respiration Metabolic acidosis resp increase greater amt CO2 exhaled decreased acidic level

33
Acid-Base Regulators Physiological Regulation –Kidneys take a few hrs to several days to regulate acid-base balance –Inc or dec HCO3+ production –Certain amino acids in renal tubules change to ammonia NH3- & excreted by kidneys

34
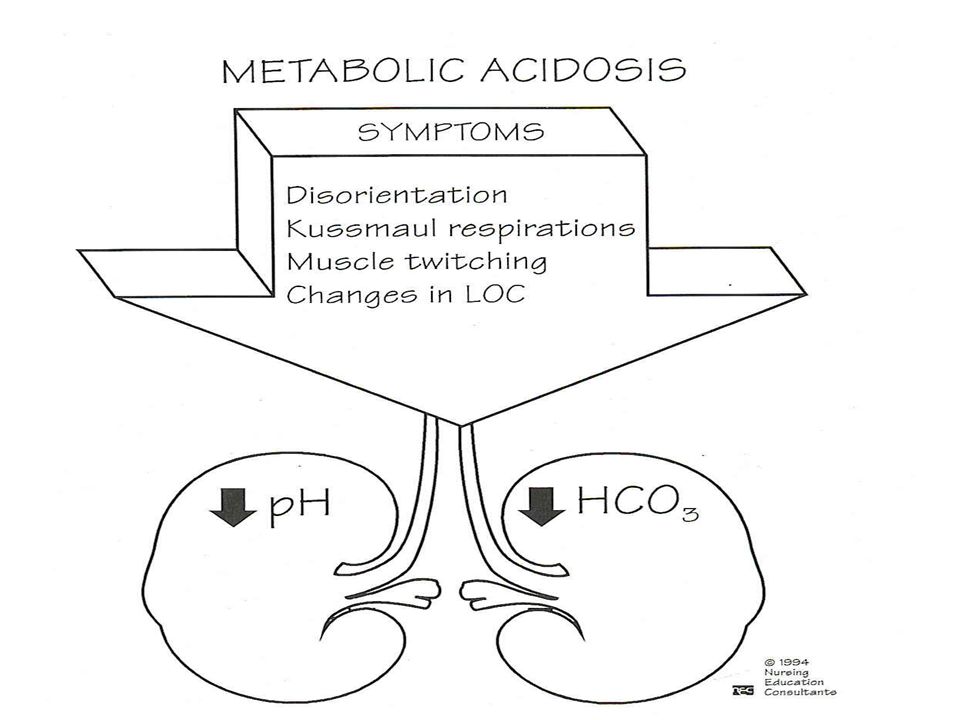
Acidosis

35
Acid-Base Balance Acid-base balance is regulated by the body’s ability to maintain arterial pH 7.35-7.45 Checked by ABGs Deviation from normal value indicates experiencing an acid- base imbalance

36
Breakdown of ABGs pH –Measures H+ ions concentration in body fluids –Slight change can be life threatening –Acidic—increase in H+ ions –Alkaline—decrease in H+ ions

37
ABGs PaCO2 Partial pressure of carbon dioxide in arterial bld Reflection of depth of pulmonary ventilation Normal 35-45 mm Hg **Hyperventilation PaCO2 < 35 mm Hg Carbon dioxide is exhaled & amt dec

38
ABGs **hypoventilation –PaCO2 is > 45 mm Hg –Less carbon dioxide is exhaled –Increasing concentration of carbon dioxide

39
ABGs PaO2 Parital pressure of O2 in arterial bld Normal 80-100 mm Hg N0 primary role in A-B regulation when normall PaO2 < 60 causes anaerobic metabolism— produces lactic acid— metabolic acidosis

40
ABGs Oxygen Saturation –When hemoglobin is saturated with O2 –Normall 95-99% –Changes in temp,PaCO2 & pH affect oxygen

41
ABGs Base Excess –Amt of blood buffer –Normal +/- 2 mEq/L –High value—alkalosis Citrate excess from rapid blood transfusions IV HCO3 infusion DKA\ Ingestion large amt bicarb solutions (antacids)
")
42
ABGs Base excess –Low value—acidosis Lg amts of bicarb ion excretion ie: diarrhea –

43
ABGs Bicarbonate –Major renal component –Kidneys excrete & retain to maintain normal balance –Principal buffer ECF –Normal 22-26 mEq/L –Metabolic acidosis < 22 mEq/L –Metabolic alkalosis > 26 mEq/L

44
Acid-Base Imbalances Either respiratory or metabolic, depend on their underlying cause Corrects AB imbalances through process known as compensation

45
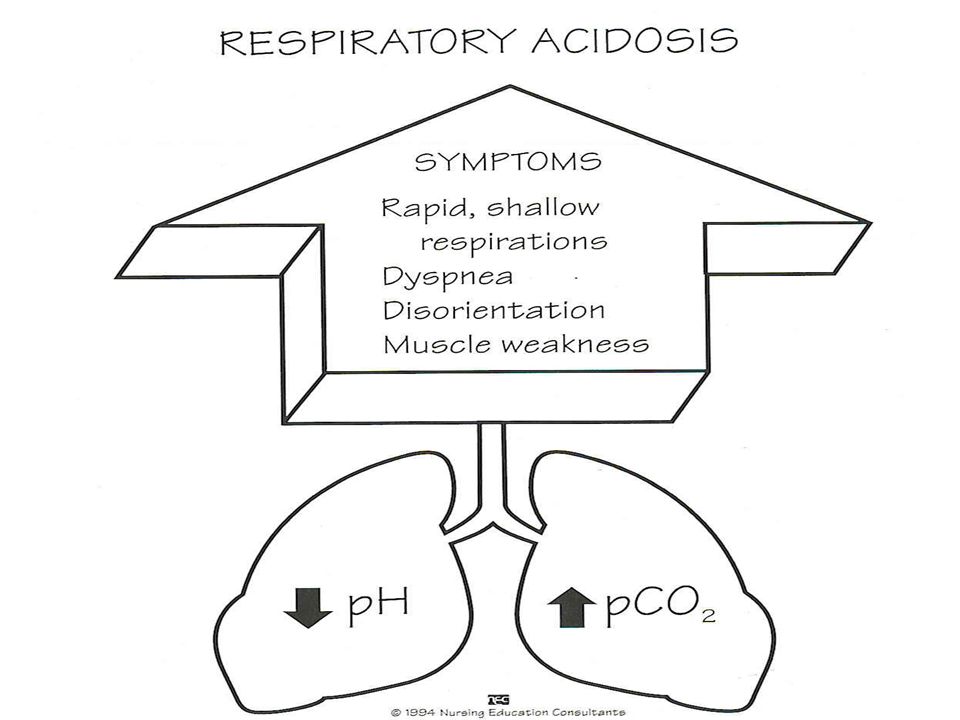
Respiratory Acidosis pH < 7.35 PaCO2 >45 mm Hg PaO2 < 80 mm Hg Bicarb level normal if uncompensated Bicarb level > 26 mEq/L if compensated Hypoventilation CSF & brain cells become acidic neurological changes hypoxemia further neurological impairment Hyperkalemia & hypercalcemia can occur Kidneys hold to bicarb & release hydrogen ions UA—may take 24 hrs

46
Respiratory Acidosis Causes Hypoventilation resulting primary respiratory problems –Chest wall injury –Respiratory failure –Cystic fibrosis –Pneumonia –Atelectasis (obstruction of small airways often caused by mucus) Hypoventilation resulting from factors other than resp system –Obesity –Head injury –Drug overdose (OD) with resp depressant –Paralysis of resp muscles caused by neurological alterations
 Hypoventilation resulting from factors other than resp system –Obesity –Head injury –Drug overdose (OD) with resp depressant –Paralysis of resp muscles caused by neurological alterations")
48
Respiratory Acidosis S/S Convulsion Coma Muscular twitching Confusion Dizziness Lethargy HA Warm flushed skin Ventricular dysrhythmia

49
Respiratory Alkalosis pH >7.45 PaCO2 <35 mm Hg PaO2 normal HCO3 nl if short-lived or uncompensated HCO3 <22 mm Hg if compensated Begins outside resp system ie: anxiety, panic attack OR within resp system ie: initial phase of asthma attack Body does not usually compensate because pH returns to nl before kidneys can respond

50
Respiratory Alkalosis Causes Salicylate overdoes Anxiety Hypermetabolic states ie: fever, exercise CNS disorders ie: head injury, infections Asthma Pneumonia Inappropriate vent settings S/S Confusion Dizziness Convulsions Coma Tachypnea Numbness/tingling of extremities dysrhythmias

52
Metabolic Acidosis High acid content of bld Loss of HCO3 pH <7.35 PaCO2 normal if uncompensated <35 mm Hg if compensated PaO2 normal or increased HCO3 < 22 mEq/L O2 Sat normal

54
Metabolic Alkalosis pH >7.45 PaCO2 normal if uncompensated PaCO2 >45 mm Hg if compensated (occurs by decreasing RR & no renal disease) PaO2 normal HCO3 > 26 mEq/L Causes –Excessive vomiting –Prolong gastric sx –Excess aldosterone –Hypokalemia –Hypercalcemia –Use of drugs ie: steriods, diuretics, sodium bicarb
 PaO2 normal HCO3 > 26 mEq/L Causes –Excessive vomiting –Prolong gastric sx –Excess aldosterone –Hypokalemia –Hypercalcemia –Use of drugs ie: steriods, diuretics, sodium bicarb")
56
Question Interpret the following ABGs: –pH? –PCO2 ? mm Hg –PO2 ? mm Hg –HCO3 ? mEq/L –O2 Sat ? %

57
Normal blood gas in an artery for humans: pH 7.35–7.45 PaCO2 35–45 mmHg PaO2 80–100 mmHg HCO3− 22–26 mmol/L

Similar presentations






















![1 Acid and Base Balance and Imbalance. 2 pH Review pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic;](/14/4450368/big_thumb.jpg "1 Acid and Base Balance and Imbalance. 2 pH Review pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic;>")




 Assistant Prof. in Pathology Al Maarefa College.>")
![1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.](/15/4651316/big_thumb.jpg "1. pH = - log [H + ] H + is really a proton Range is from 0 - 14 If [H + ] is high, the solution is acidic; pH < 7 If [H + ] is low, the solution.>")





![Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.](/20/5962628/big_thumb.jpg "Renal Acid-Base Balance. Acid An acid is when hydrogen ions accumulate in a solution. It becomes more acidic [H+] increases = more acidity CO 2 is an.>")

 concentration. More H + = more acidic = lower.>")
 *Most Common Bases E.g bicarbonate (HCO3-) *Most.>")

