Download presentation
Presentation is loading. Please wait.

1
Prepared by: Dr.Mohamed Al-Shekhani.

2
Diagnosis:

3
Etiology:

16
DIAGNOSIS:

17
Etiology:

18
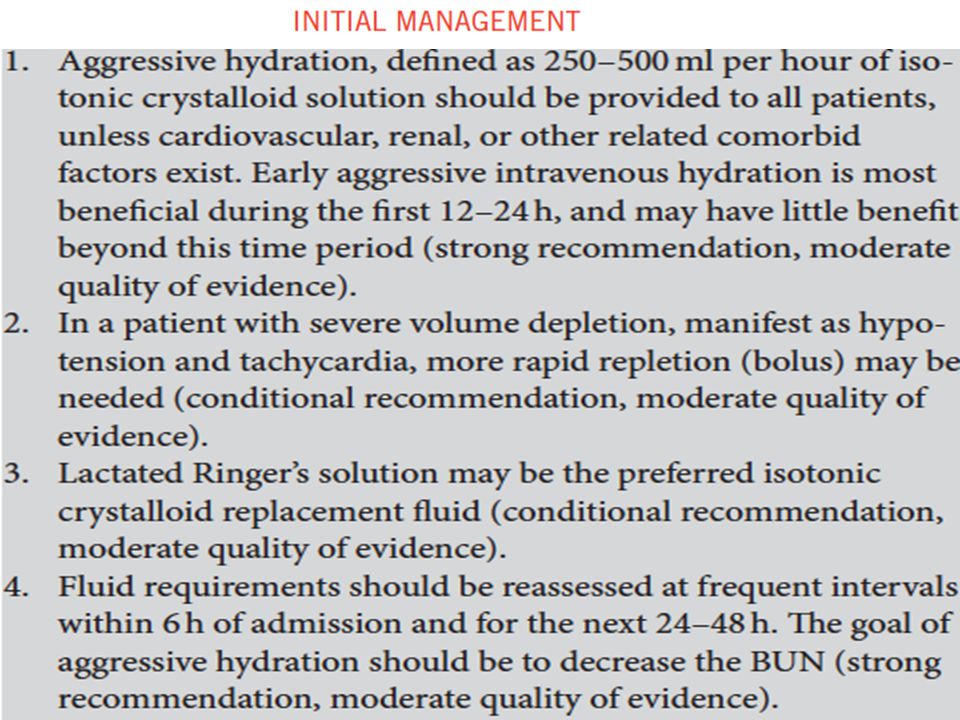
Initial management:

19
ERCP in AP:

20
Antibiotics in AP:

21
Nutrition in AP:

22
Surgery in AP:

23
BO4Qs1: 1. Which one of the following is a required finding for the diagnosis of acute pancreatitis (AP)? A. Severe mid-abdominal pain B. E levated serum amylase between *1 – 3 ULN. C. Abnormal appearance of the pancreas on CT imaging D. Exclusion of peptic ulcer disease on normal upper endoscopy
. A. Severe mid-abdominal pain B. E levated serum amylase between *1 – 3 ULN. C. Abnormal appearance of the pancreas on CT imaging D. Exclusion of peptic ulcer disease on normal upper endoscopy.")
24
BO4Qs1: 1. Which one of the following is a required finding for the diagnosis of acute pancreatitis (AP)? A. Severe mid-abdominal pain B. E levated serum amylase between *1 – 3 ULN. C. Abnormal appearance of the pancreas on CT imaging D. Exclusion of peptic ulcer disease on normal upper endoscopy
. A. Severe mid-abdominal pain B. E levated serum amylase between *1 – 3 ULN. C. Abnormal appearance of the pancreas on CT imaging D. Exclusion of peptic ulcer disease on normal upper endoscopy.")
25
BO4Qs2: 2. Which one of the following statements is true regarding gallstone-associated AP? A. ERCP is contraindicated in patients with AP & cholangitis. B. Cholecystectomy should be delayed for 4–6 weeks in patients with AP and gallstones in the gallbladder. C. Pancreatic duct stents lower the risk of severe post- ERCP pancreatitis in high-risk patients. D. All patients with AP and gallstones should be given antibiotics to prevent the development of pancreatic necrosis.

26
BO4Qs2: 2. Which one of the following statements is true regarding gallstone-associated AP? A. ERCP is contraindicated in patients with AP & cholangitis. B. Cholecystectomy should be delayed for 4–6 weeks in patients with AP and gallstones in the gallbladder. C. Pancreatic duct stents lower the risk of severe post- ERCP pancreatitis in high-risk patients. D. All patients with AP and gallstones should be given antibiotics to prevent the development of pancreatic necrosis.

27
BO4Qs3: 3. Which one of the following statements is true regarding nutrition in AP? A. In mild AP, nasojejunal feeding decreases the risk of progression to more severe AP. B. In severe AP, RCTs have clearly shown NJ feeding to be superior to NGT feeding. C. Parenteral nutrition is indicated in severe AP. D. Low-fat solid diets are equal to liquid diets in mild AP.

28
BO4Qs3: 3. Which one of the following statements is true regarding nutrition in AP? A. In mild AP, nasojejunal feeding decreases the risk of progression to more severe AP. B. In severe AP, RCTs have clearly shown NJ feeding to be superior to NGT feeding. C. Parenteral nutrition is indicated in severe AP. D. Low-fat solid diets are equal to liquid diets in mild AP.

29
BO4Qs4: 4. Which one of the following quantities is considered the cut-off for small versus large gallstones? A. > 5 mm B. > 8 mm C. > 10 mm D. > 12 mm

30
BO4Qs4: 4. Which one of the following quantities is considered the cut-off for small versus large gallstones? A. > 5 mm B. > 8 mm C. > 10 mm D. > 12 mm?

31
BO4Qs5: 3. Which one of the following is an indication for deep cannulation of the pancreatic duct during ERCP? A. Acute biliary pancreatitis B. Chronic pancreatitis with symptomatic stricture C. Sphincter of Oddi manometry D. Suspected cholangiocarcinoma

32
BO4Qs5: 3. Which one of the following is an indication for deep cannulation of the pancreatic duct during ERCP? A. Acute biliary pancreatitis B. Chronic pancreatitis with symptomatic stricture C. Sphincter of Oddi manometry D. Suspected cholangiocarcinoma

33
BO4Qs6: 3. CECT or MRI in AP is indicated in all these situations except ? A. As initial evaluation. B. When the diagnosis is unclear. C. To evaluate local complications. D. When is no early clinical improvement.

34
BO4Qs6: 3. CECT or MRI in AP is indicated in all these situations except ? A. As initial evaluation. B. When the diagnosis is unclear. C. To evaluate local complications. D. When is no early clinical improvement.

35
BO4Qs7: 3. The preferred fluid replacement therapy in AP is? A. Normal saline. B. Glucose saline. C. Colloides. D. Ringer lactate. E. Albumin.

36
BO4Qs7: 3. The preferred fluid replacement therapy in AP is? A. Normal saline. B. Glucose saline. C. Colloides. D. Ringer lactate. E. Albumin.

37
BO4Qs8: 3. Severe AP is defined when there is? A. Local complications. B. Transient Organ failure. C. Persistent organ failure. D. A&C. E. C.

38
BO4Qs8: 3. Severe AP is defined when there is? A. Local complications. B. Transient Organ failure. C. Persistent organ failure. D. A&C. E. C.

39
BO4Qs9: 3. In the absence of gall stones & alcohol abuse, hypertriglyceridemia is considered causative of AP is the level is above? A. 500. B. 600. C. 800. D. 900. E. 1000.

40
BO4Qs9: 3. In the absence of gall stones & alcohol abuse, hypertriglyceridemia is considered causative of AP is the level is above? A. 500. B. 600. C. 800. D. 900. E. 1000.

41
BO4Qs10: 3. Genetic testing for heriditary AP is indicated when there is family history of pancreatic disease & the age is less than? A. 50. B. 40. C. 30. D.50. E. 20.

42
BO4Qs10: 3. Genetic testing for heriditary AP is indicated when there is family history of pancreatic disease & the age is less than? A. 50. B. 40. C. 30. D.50. E. 20.

43
BO4Qs11: 3. The risks & benefits of routine EUS in finding a cause of idiopathic AP are? A. Clear. B. Unclear. C.Well established. D. More Risky. E. None of the above.

44
BO4Qs11: 3. The risks & benefits of routine EUS in finding a cause of idiopathic AP are? A. Clear. B. Unclear. C.Well established. D. More Risky. E. None of the above.

Similar presentations
























![GI Endoscopy ~ BASIC ~ ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS EOSINOPHILIC ESOPHAGITIS IN CHILDREN [LECTURE] EOSINOPHILIC.](/20/5943603/big_thumb.jpg "GI Endoscopy ~ BASIC ~ ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS EOSINOPHILIC ESOPHAGITIS IN CHILDREN [LECTURE] EOSINOPHILIC.>")





,FACS,Associted Prof.Umm- Alqura university.>")