Download presentation
Presentation is loading. Please wait.

1
GYNAECOLOGICAL HISTORY AND EXAMINATION

2
LECTURE OVERVIEW Taking a gynaecological history ABCD(I)F
Abdominal/ pelvic pain Bleeding Contraception Discharge and itch (E) Incontinence and prolapse Fertility Performing a gynaecological examination Abdominal palpation Speculum examination of vulva/ vagina/cervix Bimanual palpation of uterus and adnexae Approach to common gynaecological symtoms
 Incontinence and prolapse. Fertility. Performing a gynaecological examination. Abdominal palpation. Speculum examination of vulva/ vagina/cervix. Bimanual palpation of uterus and adnexae. Approach to common gynaecological symtoms.")
3
GYNAECOLOGICAL HISTORY
Age Past medical, surgical, gynaecological history Medications Allergies Family History Social History

4
GYNAECOLOGICAL HISTORY
Past Obstetric History Have you ever been pregnant before? Spontaneous abortions, terminations of pregnancy, ongoing pregnancies, living children What happened in those pregnancies? Spontaneous, duration of pregnancy, type of labour and delivery, outcome, complications

5
GYNAECOLOGICAL HISTORY
Abdominal pelvic pain Bleeding Contraception Discharge (itch) Incontinence and prolapse Fertility Screening history
 Incontinence and prolapse. Fertility. Screening history.")
6
(1) PELVIC PAIN What causes pain? Ovulation Dysmenorrhoea
ovarian cysts, particularly if complicated (THINRIM) torsion, haemorrhage, infection, necrosis, rupture, malignant change endometriosis infection PID, tubo-ovarian abscess complication of pregnancy miscarriage, ectopic pregnancy
 torsion, haemorrhage, infection, necrosis, rupture, malignant change. endometriosis. infection. PID, tubo-ovarian abscess. complication of pregnancy. miscarriage, ectopic pregnancy.")
7
(1) PELVIC PAIN Pain with periods (dysmenorrhoea)
Pain with sex (dyspareunia) Pain at other times Site of pain, radiation sudden or gradual associated symptoms fever, discharge LNMP
 Pain at other times. Site of pain, radiation. sudden or gradual. associated symptoms. fever, discharge. LNMP.")
8
(2) BLEEDING Menstrual history menarche
cycle length and regularity (5/28) midcycle bleeding/pain/mucus change excessively heavy or painful LNMP Abnormal bleeding Abnormal menstrual bleeding Abnormal non menstrual bleeding intermenstrual bleeding, post coital bleeding, postmenopausal bleeding
 midcycle bleeding/pain/mucus change. excessively heavy or painful. LNMP. Abnormal bleeding. Abnormal menstrual bleeding. Abnormal non menstrual bleeding. intermenstrual bleeding, post coital bleeding, postmenopausal bleeding.")
9
(2) BLEEDING What causes abnormal menstrual bleeding?
‘Dysfunctional bleeding’ (ie abnormal menstrual bleeding in response to reproductive hormones) ovulatory anovulatory Uterine pathology which increases surface area of endometrium polyps fibroids Coagulopathy
 ovulatory. anovulatory. Uterine pathology which increases surface area of endometrium. polyps. fibroids. Coagulopathy.")
10
(2) BLEEDING What causes non-menstrual bleeding? Post coital bleeding
cervical lesion (polyp, cervicitis, cancer) Intermenstrual bleeding midcycle bleeding cervical/ uterine malignancy Postmenopausal bleeding endometrial hyperplasia atrophic endometrium
 Intermenstrual bleeding. midcycle bleeding. cervical/ uterine malignancy. Postmenopausal bleeding. endometrial hyperplasia. atrophic endometrium.")
11
(3) DISCHARGE AND ITCH What causes discharge? physiological discharge
tubal infection (PID)/ malignancy uterine infection/malignancy cervical infection/malignancy vaginal infection (vaginitis, vaginosis) vulval infection/ malignancy Physiological discharge + bacterial vaginosis and vaginitis + UGT infection = 95% of presentations with discharge
/ malignancy. uterine infection/malignancy. cervical infection/malignancy. vaginal infection (vaginitis, vaginosis) vulval infection/ malignancy. Physiological discharge + bacterial vaginosis and vaginitis + UGT infection = 95% of presentations with discharge.")
12
(3) DISCHARGE AND ITCH Nature of discharge amount
colour (bloody, offensive, yellow, brown) offensive relationship to period Associated symptoms vulval burning and itch, urinary frequency
 offensive. relationship to period. Associated symptoms. vulval burning and itch, urinary frequency.")
13
(4) CONTRACEPTION AND FERTILITY
Type of contraception, side-effects, compliance, complications including breakthrough pregnancies Fertility number of pregnancies time taken to get pregnant Infertility duration sexual history history of anovulation, tubal disease or surgery, male factor

14
(5) PROLAPSE AND INCONTINENCE
Vulval lump, dragging pain or pressure Incontinence urinary stress urgency faecal incontinence or soiling flatus incontinence

16
GNAECOLOGICAL EXAMINATION
Explain examination Allow patient privacy to change Chaperone Ensure patient is draped, and room is warm and comfortable

17
GNAECOLOGICAL EXAMINATION
General examination H&N, breasts, cardiorespiratory, abdominal, periphery Abdominal palpation Inspection external genitalia Speculum examination vagina/cervix Bimanual palpation of uterus and adnexae

18
Inspection Hair distribution Vulval skin
Look at the perineum for scars/tears Gently part labia – inspect urethra Look for discharge, prolapse, ulcers, warts Hair extending towards umbilicus and onto inner thigh can be associated with disorders of androgen excess and clitoromegaly. Vulva can be a site of chronic skin conditions such as eczema, psoriasis, Lichen sclerosis and warts, cysts of the Bartholin’s gland and cancers. Ulceration may imply herpes, syphilis, trauma or malignancy. Perineal scars maybe secondary to childbirth.

19
Pelvic Examination Empty bladder! Vaginal Cervix Uterus Adnexa Rectal
Wash hands, gloves, warm vaginal speculum with warm water, obtain specimens as needed (Pap smear, cultures) Vaginal Lesions, discharge Cervix Cervical excitation, os open/closed, Polyps, erosions, etc... Uterus Size, shape, regularity, tenderness, position, mobility Adnexa Masses, tenderness, ovaries Rectal Mass, tenderness, blood
 Vaginal. Lesions, discharge. Cervix. Cervical excitation, os open/closed, Polyps, erosions, etc... Uterus. Size, shape, regularity, tenderness, position, mobility. Adnexa. Masses, tenderness, ovaries. Rectal. Mass, tenderness, blood.")
20
Insertion Use lubricant and warm speculum if possible
Hold speculum in dominant hand Part labia with nondominant hand Slowly insert and open speculum blades to visualize the cervix.

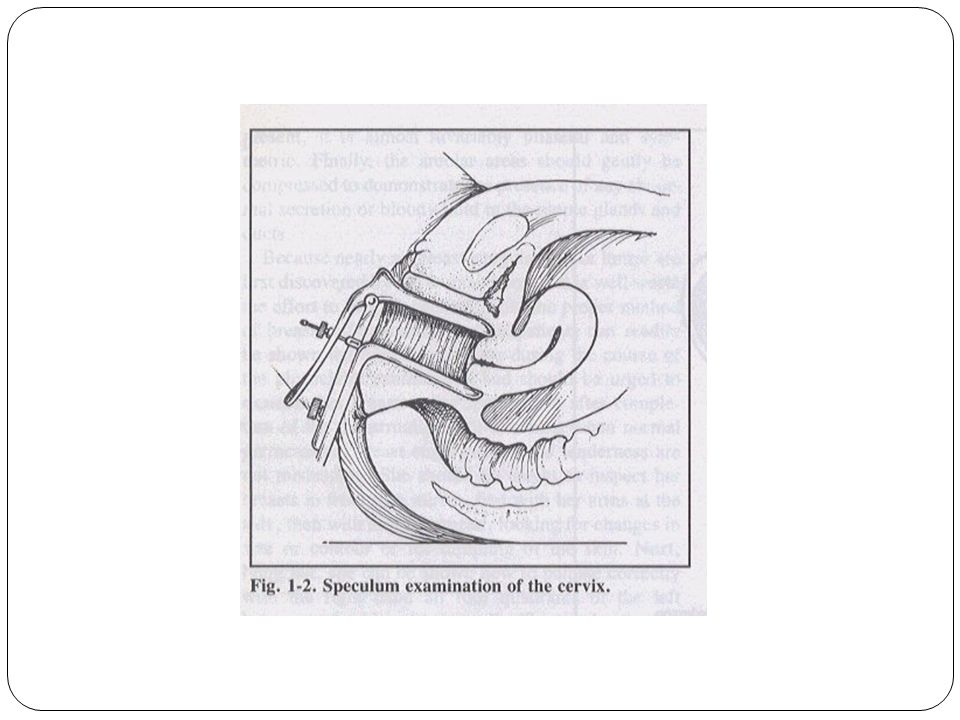
21
Visualisation of Cervix
Inspect for: Discharge Warts Tumours Size of cervical os Bleeding

23
Taking a cervical smear
Following insertion of bivalve speculum Equipment prepared before examination begins: gloves Aylesbury spatula Confirm name, DOB, hosp number etc Label frosted end of slide Fixative agent Position equipment

24
Taking a Cervical smear
Rest point of spatula within the os and rotate clockwise 360° then rotate 360° anti- clockwise. Exert light pressure (pencil). Ensure contact with cervix throughout.
. Ensure contact with cervix throughout.")
25
Concluding Cervical Smear
REMOVE the speculum! Ensure patient comfort/safety Spread both sides of the spatula onto the slide. Perform similar procedure for cytobrush Spray fixative immediately onto the labelled slide surface

26
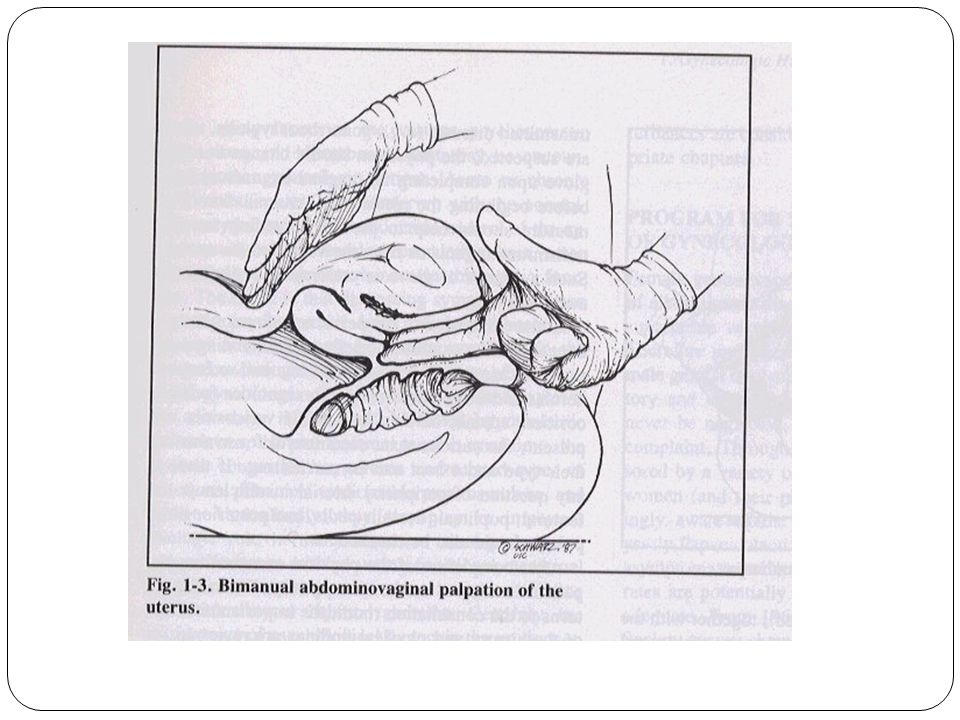
Bimanual Examination Separate labia with gloved left hand
Slowly insert index finger and middle finger into vagina then palpate cervix Left hand then palpates uterus and adnexa abdominally

29
Univalve Speculum Positioning
Position patient in the left lateral position Left leg extended Right Knee drawn up to chest Hold back anterior vaginal wall with lubricated speculum

30
Hx of presenting complaint Past Obstetric Hx (gravity, parity)
Dear Dr, Thank you for seeing Mary Smith who has problematic vaginal bleeding. Age Hx of presenting complaint Past Obstetric Hx (gravity, parity) Past gynae Hx PMHx, PSHx, PGHx Medications, Allergies FHx, SHx
 Past gynae Hx. PMHx, PSHx, PGHx. Medications, Allergies. FHx, SHx.")
31
Dear Dr, Thank you for seeing Mary Smith who has problematic vaginal bleeding.
History of bleeding menstrual cycle; ? ovulating amount LNMP contraception sinister features: post coital, intermenstrual, post menopausal bleeding associated symptoms pain, symptoms of anaemia Remainder of gynae history discharge, prolapse, incontinence, POHx, fertility, PAP, breasts

32
Dear Dr, Thank you for seeing Mary Smith who has problematic vaginal bleeding.
O/Ex: general examination pallor abdominal palpation ?enlarged or tender uterus speculum examination blood coming from os normal vagina and cervix Bimanual examination size of uterus adnexal pathology

33
Ix will depend on Hx and Ex, but may involve:
Dear Dr, Thank you for seeing Mary Smith who has problematic vaginal bleeding. Ix will depend on Hx and Ex, but may involve: hCG PAP smear FBE Fe studies Coagulation profile Ultrasound Endometrial sampling Hysteroscopy, D&C

34
SUMMARY How to take a ‘general’ gynaecological history (A,B,C,D,I/P,F)
Reproductive screening How to take a ‘targetted’ history of a specific presenting complaint such as bleeding, pain, discharge, prolapse and incontinence, infertility 3 parts of gynaecological examination abdominal palpation speculum examination bimanual examination Combining history and examination features to come up with a differential diagnosis, and plan investigations

Similar presentations


 During the exam, a health care provider.>")


















