Download presentation
Presentation is loading. Please wait.

1
Pediatric Respiratory Emergencies Part 2 Mohammed Al Faifi, MD. Pediatric Emergency Consultant Department of Emergency Medicine King Faisal Specialist Hospital & Research Centre Riyadh, KSA KUWAIT, Oct. 2011

2
Topics to be covered Bronchiolitis Bronchiolitis Croup Croup

3
2005 National Hospital Ambulatory Medical Care Survey 2005 National Hospital Ambulatory Medical Care Survey a nationally representative sample of USA patients was analyzed a nationally representative sample of USA patients was analyzed Data on visits to EDs by children Data on visits to EDs by children – 1 -19 years of age with moderate/severe Asthma – 1 -19 years of age with moderate/severe Asthma – 3 months to 2 years of age with Bronchiolitis – 3 months to 2 years of age with Bronchiolitis – 3 months to 3 years of age with Croup – 3 months to 3 years of age with Croup Knapp et al. Pediatrics 2008

4
ResultsResults CorticosteroidsAntibioticsRadiographs 69% of the 405,000 visits for moderate/ severe asthma 31% of the estimated 317,000 annual croup visits 53% of the estimated 228,000 annual visits for bronchiolitis 72% of bronchiolitis visits 32% of croup visits Knapp et al. Pediatrics 2008

5
ConclusionsConclusions Physicians treating children with Physicians treating children with Asthma, Asthma, bronchiolitis bronchiolitis croup croup In USA Emergency Departments are under using known effective treatments and overusing ineffective or unproven therapies and diagnostic tests. Knapp et al. Pediatrics 2008

6
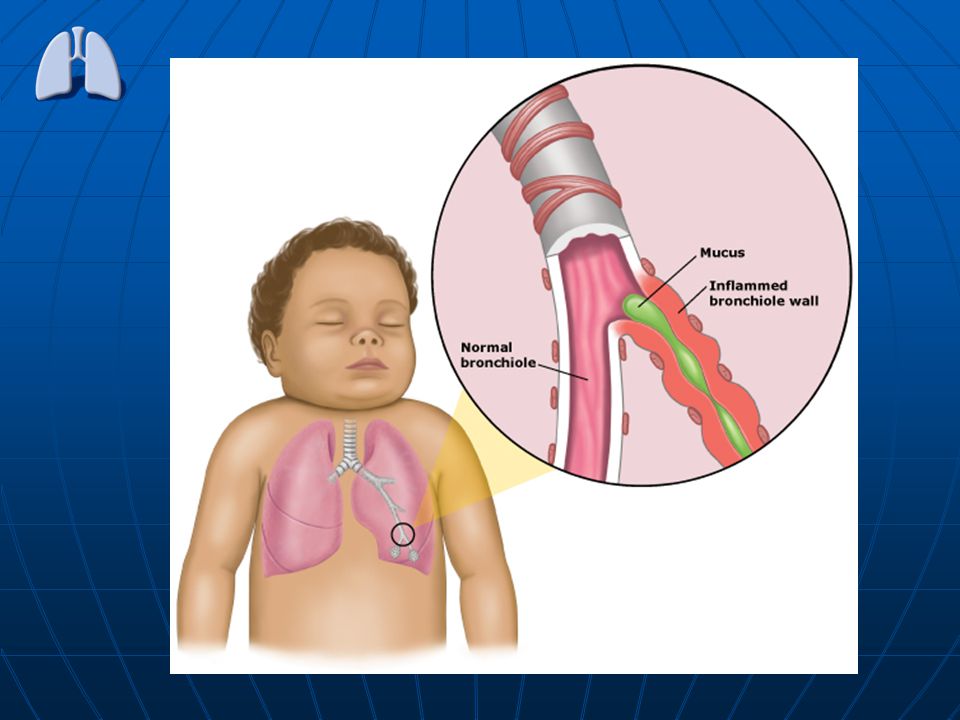
A 5-month-old presents with cough for 2 days A 5-month-old presents with cough for 2 days Preceded by a URI, his feeding has decreased and his Preceded by a URI, his feeding has decreased and his cough interrupts sleep, Temp. 38° at home. Normal PMHx. Case No. 1

7
Temp 38.5°, RR 60, SaO 2 94% in room air Temp 38.5°, RR 60, SaO 2 94% in room air Mild rhinorrhea, air entry good, Mild rhinorrhea, air entry good, wheezing in all fields wheezing in all fields Well Hydrated, feeds well Well Hydrated, feeds well No grunting or retractions No grunting or retractions This is a classic case of This is a classic case of On Exam: Bronchiolitis

9
Diagnosis.Diagnosis. May be necessary for bed placement May be necessary for bed placement Not all bronchiolitis is RSV (metapneumovirus, para virus) Not all bronchiolitis is RSV (metapneumovirus, para virus) Yet may decrease likelihood of bacteremia Yet may decrease likelihood of bacteremia (but not UTI ) (but not UTI ) RSV wash
 Not all bronchiolitis is RSV (metapneumovirus, para virus) Yet may decrease likelihood of bacteremia Yet may decrease likelihood of bacteremia (but not UTI ) (but not UTI ) RSV wash.")
10
Febrile infants with confirmed viral infections are at lower risk for SBI than those in whom a viral infection is not identified Viral diagnostic data can positively contribute to the management of febrile infants, especially those who are classified as High risk. Peditrics Vol. 113: 1662, 2004

11
Differential Diagnosis Gastroesophageal reflux disease Gastroesophageal reflux disease Tracheoesophageal fistula Tracheoesophageal fistula Tracheomalacia Tracheomalacia Vascular ring Vascular ring Cystic fibrosis & immunodeficiency Cystic fibrosis & immunodeficiency CHD CHD Foreign body aspiration. Foreign body aspiration.

12
CXR CXR Diagnosis,

13
Evaluation of the utility of radiography in acute bronchiolitis. A prospective study of 265 children aged 2 to 23 months who presented to the ED with bronchiolitis analyzed use of routine radiography in patients with a simple form of the disease (defined in a child as coryza, cough, and respiratory distress accompanying a first episode of wheezing without underlying illness). A prospective study of 265 children aged 2 to 23 months who presented to the ED with bronchiolitis analyzed use of routine radiography in patients with a simple form of the disease (defined in a child as coryza, cough, and respiratory distress accompanying a first episode of wheezing without underlying illness). Schuh S, et al. J Pediatr. 2007
. A prospective study of 265 children aged 2 to 23 months who presented to the ED with bronchiolitis analyzed use of routine radiography in patients with a simple form of the disease (defined in a child as coryza, cough, and respiratory distress accompanying a first episode of wheezing without underlying illness). Schuh S, et al. J Pediatr")
14
ResultResult The findings were consistent with bronchiolitis except in only 2 cases, and in neither case did the findings change short-term management. The findings were consistent with bronchiolitis except in only 2 cases, and in neither case did the findings change short-term management. Schuh S, et al. J Pediatr. 2007

15
HIGH RISK Premature birth (< 35-37 weeks & younger age (< 6-12 weeks of life) Premature birth (< 35-37 weeks & younger age (< 6-12 weeks of life) Full term and younger than 1 month, Full term and younger than 1 month, Bronchopulmonary, cystic fibrosis Bronchopulmonary, cystic fibrosis (CHD), and immune deficiency disease (CHD), and immune deficiency disease Child’s parents or a clinician had already witnessed an apnea episode Child’s parents or a clinician had already witnessed an apnea episode
 Premature birth (< weeks & younger age (< 6-12 weeks of life) Full term and younger than 1 month, Full term and younger than 1 month, Bronchopulmonary, cystic fibrosis Bronchopulmonary, cystic fibrosis (CHD), and immune deficiency disease (CHD), and immune deficiency disease Child’s parents or a clinician had already witnessed an apnea episode Child’s parents or a clinician had already witnessed an apnea episode")
16
ManagementManagement Nasal Suction Beta 2 Agonists – Clinical trials, meta-analyses & systematic – Clinical trials, meta-analyses & systematic reviews (2000-2004) showed some reviews (2000-2004) showed some differences in short term benefits (oxygen, differences in short term benefits (oxygen, RR) yet no difference in clinically meaningful RR) yet no difference in clinically meaningful outcomes (admission, length of stay) outcomes (admission, length of stay) – Yet some will respond. – Yet some will respond.

17
Bronchodilators for bronchiolitis. A Cochrane review of bronchodilators other than epinephrine found that the agents produce small, short-term improvements but do not affect rate of hospitalization or length of hospital A Cochrane review of bronchodilators other than epinephrine found that the agents produce small, short-term improvements but do not affect rate of hospitalization or length of hospital Cochrane Database Syst Rev. 2006;(3)
.")
18
Epinephrine and Bronchiolitis A meta-analysis suggested a decrease in clinical symptoms when compared with either placebo A meta-analysis suggested a decrease in clinical symptoms when compared with either placebo Hartling L, et al. Arch Pediatr Adolesc Med. 2003;157;957-64.

19
Ipratropium bromide At this point, use of anticholinergic agents―either alone or in combination with beta-adrenergic agents―for viral bronchiolitis is not justified in the ED

20
Bronchiolitis & Steroids Corticosteroids Corticosteroids – 2004 Cochrane Review, 13 trials, 1200 children – 2004 Cochrane Review, 13 trials, 1200 children No difference in admission rates, no benefits compared to placebo No difference in admission rates, no benefits compared to placebo – PECARN multicenter trial – PECARN multicenter trial Compared Dexamethasone and placebo in ED patients with Compared Dexamethasone and placebo in ED patients with bronchiolitis bronchiolitis No difference in admission at 4 hours No difference in admission at 4 hours

21
Bronchiolitis & Steroids 70 children, 3 winters, one center 70 children, 3 winters, one center 2-23 months, first wheezing with distress and URI 2-23 months, first wheezing with distress and URI Dexamethasone (36) vs. placebo (34) Dexamethasone (36) vs. placebo (34) Dexamethasone group Dexamethasone group – More improved clinical score – More improved clinical score – Few hospitalizations (19% vs 44%) – Few hospitalizations (19% vs 44%) Schuh et al. J Pediatr 2002 Schuh et al. J Pediatr 2002
 Dexamethasone (36) vs. placebo (34) Dexamethasone group Dexamethasone group – More improved clinical score – More improved clinical score – Few hospitalizations (19% vs 44%) – Few hospitalizations (19% vs 44%) Schuh et al. J Pediatr 2002 Schuh et al. J Pediatr")
22
Dexamethasone for Bronchiolitis, A Multicenter, Randomized, Controlled Trial: The study compare single dose of oral dexamethasone (1 mg per The study compare single dose of oral dexamethasone (1 mg per kilogram of body weight) with placebo in 600 children (age range, 2 kilogram of body weight) with placebo in 600 children (age range, 2 to 12 months) with a first episode of wheezing diagnosed in the to 12 months) with a first episode of wheezing diagnosed in the ED as moderate-to-severe bronchiolitis. ED as moderate-to-severe bronchiolitis. 20 emergency departments during the months of November through April over a 3-year period 20 emergency departments during the months of November through April over a 3-year period NEJM 2007; 357:331-9 NEJM 2007; 357:331-9

23
Epinephrine and Dexamethasone in Children with Bronchiolitis Multicenter, double-blind, placebo-controlled trial 800 infants (6 weeks to 12 months of age) with bronchiolitis randomly assigned to one of four study groups 800 infants (6 weeks to 12 months of age) with bronchiolitis randomly assigned to one of four study groups The primary outcome was hospital admission within 7 days after the day of enrollment (the initial visit to the emergency department) The primary outcome was hospital admission within 7 days after the day of enrollment (the initial visit to the emergency department) N Engl J Med 2009; 360:2079-2089 Hospital Admissions by the 7th day 34 infants (17.1%) in the epinephrine- dexamethasone group 47 (23.7%) in the epinephrine group 51 (25.6%) in the dexamethasone group 53 (26.4%) in the placebo group
 with bronchiolitis randomly assigned to one of four study groups 800 infants (6 weeks to 12 months of age) with bronchiolitis randomly assigned to one of four study groups The primary outcome was hospital admission within 7 days after the day of enrollment (the initial visit to the emergency department) The primary outcome was hospital admission within 7 days after the day of enrollment (the initial visit to the emergency department) N Engl J Med 2009; 360: Hospital Admissions by the 7th day 34 infants (17.1%) in the epinephrine- dexamethasone group 47 (23.7%) in the epinephrine group 51 (25.6%) in the dexamethasone group 53 (26.4%) in the placebo group")
24
ConclusionsConclusions Among infants with bronchiolitis treated in the ED, combined therapy with Dexamethasone and Epinephrine may significantly reduce hospital admissions, Admission Criteria: Admission Criteria: Hypoxemia and poor feeding Less than 34 weeks Heart disease Atelectasis Less than 2 months,

25
A 3-year-old with cough at 2 AM, The child had a URI for 2 days and then began to cough, with hoarseness and stridor. In the ED he is febrile (38°), running around the room, without stridor at rest. No drooling No drooling Lungs clear Lungs clear Case No. 2
, running around the room, without stridor at rest. No drooling No drooling Lungs clear Lungs clear Case No. 2.")
26
CXR CXR NO NO

27
Mist therapy??? Mist therapy??? Corticosteroids Corticosteroids – Effective in moderate to severe croup—PO / IM – Effective in moderate to severe croup—PO / IM – Dexamethasone (0.15 - 0.6 mg/kg) PO/ IM – Dexamethasone (0.15 - 0.6 mg/kg) PO/ IM Aerosolized Racemic epinephrine Aerosolized Racemic epinephrine – No rebound---reserve for kids with stridor at rest – No rebound---reserve for kids with stridor at rest If clinically fine after 2 hours may, send home Treatment Options:
 PO/ IM – Dexamethasone ( mg/kg) PO/ IM Aerosolized Racemic epinephrine Aerosolized Racemic epinephrine – No rebound---reserve for kids with stridor at rest – No rebound---reserve for kids with stridor at rest If clinically fine after 2 hours may, send home Treatment Options:.")
Similar presentations









, ranging in severity: Acute bronchitis - an acute respiratory tract infection in.>")











