Download presentation
Presentation is loading. Please wait.

1
TRANSITION SERIES Topics for the Advanced EMT CHAPTER Respiratory Emergencies: Airway Resistance Disorders 28

2
Objectives Review the frequency of airway resistance disorders in the U.S. Identify pathophysiological changes due to airway resistance disorders. Relate pathophysiology with assessment findings. Discuss current treatment standards for patients with airway resistance disorders.

3
Introduction Breathing is usually an effortless procedure under autonomic control. Airway resistance disorders are those that make this process difficult for the patient. Many findings of labored breathing are actually the body's attempt at improving breathing adequacy in light of the disease.

4
Epidemiology 2 million ED visits a year due to asthma. 9.5 million people in the United States have been diagnosed with bronchitis. Bronchiolitis is a highly contagious disease common to children under 5 years of age.

5
Pathophysiology Asthma –Most common complaint is respiratory distress. –Extrinsic and Intrinsic asthma. –Basic pathophysiology is narrowing of the bronchioles, overproduction of mucus, and edema.

6
Pathophysiology (cont’d) Asthma (continued) –Collectively, these changes increase the resistance to airflow as the patient tries to breathe.
 Asthma (continued) –Collectively, these changes increase the resistance to airflow as the patient tries to breathe.")
7
Pathophysiology (cont’d) Asthma types –Intrinsic –Extrinsic Pathophysiologic changes –Bronchospasm –Edema –Mucus production
 Asthma types –Intrinsic –Extrinsic Pathophysiologic changes –Bronchospasm –Edema –Mucus production")
8
Pathophysiologic changes in the bronchioles in asthma contribute to higher airway resistance.

9
Pathophysiology (cont’d) Bronchitis –Inflammation of bronchial lining –Thickening of mucosal wall –Changes resistance to airflow
 Bronchitis –Inflammation of bronchial lining –Thickening of mucosal wall –Changes resistance to airflow")
10
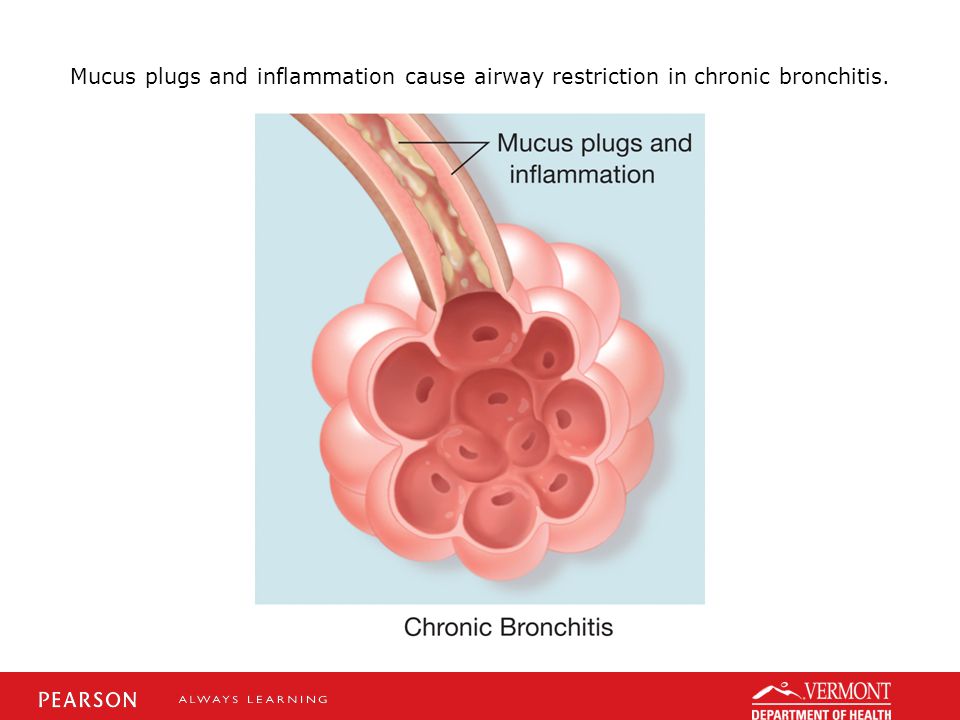
Mucus plugs and inflammation cause airway restriction in chronic bronchitis.

12
Pathophysiology (cont’d) Types of bronchitis –Acute bronchitis Short duration (<3 weeks) Sputum production –Chronic bronchitis COPD disorder Productive cough persisting for 3 consecutive months a year, for at least 2 consecutive years
 Types of bronchitis –Acute bronchitis Short duration (<3 weeks) Sputum production –Chronic bronchitis COPD disorder Productive cough persisting for 3 consecutive months a year, for at least 2 consecutive years")
13
Pathophysiology (cont’d) Bronchiolitis –Diagnosis of younger patients. –Inflammation that results in mucosal edema. –Lumen size of bronchioles decreases. –Airway resistance increases with changes in gas diffusion at the alveolar level.

14
Assessment Findings General assessment findings –Common to most patients with dyspnea Tachypnea, prolonged exhalation, wheezes Accessory muscle use Tripod positioning and retractions Nasal flaring, mouth breathing Changes in pulse oximetry and vitals Skin change and mental status changes

15
Assessment Findings (cont’d) Additional findings with asthma –Progressive dyspnea –Nonproductive cough –Wheezing on auscultation –URI findings –Chest tightness –History of asthma –Prescribed MDI or nebulizer
 Additional findings with asthma –Progressive dyspnea –Nonproductive cough –Wheezing on auscultation –URI findings –Chest tightness –History of asthma –Prescribed MDI or nebulizer")
16
Assessment Findings (cont’d) Additional findings with acute bronchitis –Productive cough –Sore throat –Edematous nasal mucosa –Malaise, fatigue, muscle aches –Occasionally fever, nausea/vomiting
 Additional findings with acute bronchitis –Productive cough –Sore throat –Edematous nasal mucosa –Malaise, fatigue, muscle aches –Occasionally fever, nausea/vomiting")
17
Assessment Findings (cont’d) Additional findings with chronic bronchitis –Typically overweight –Cyanotic complexion –Vigorous productive cough –Coarse rhonchi on auscultation –Possible wheezing on auscultation
 Additional findings with chronic bronchitis –Typically overweight –Cyanotic complexion –Vigorous productive cough –Coarse rhonchi on auscultation –Possible wheezing on auscultation")
18
Assessment Findings (cont’d) Additional findings with bronchiolitis –More common to infants and children –Infants tend to be more “fussy” –Hx of recent URI –Onset over 2-5 days –Nonproductive cough –Fever –Possible diffuse wheezing
 Additional findings with bronchiolitis –More common to infants and children –Infants tend to be more fussy –Hx of recent URI –Onset over 2-5 days –Nonproductive cough –Fever –Possible diffuse wheezing")
19
Findings for Respiratory Airway Disorders

20
Emergency Medical Care Patient positioning. Ensure airway adequacy. Provide oxygen based on ventilatory need. –NRB mask at 15 lpm with adequate breathing. –PPV with 15 lpm oxygen with inadequate breathing.

21
Emergency Medical Care (cont’d) Administer an inhaled beta-2-specific agonist if warranted
 Administer an inhaled beta-2-specific agonist if warranted")
22
Case Study While you are having dinner on shift at a local restaurant, a female holding a young child bursts into the restaurant. She states she saw the ambulance in the parking lot and stopped. She states she was rushing her child to the hospital for trouble breathing. She is carrying an MDI, but was afraid to use it.

23
Case Study (cont’d) Scene Size-Up –You are in a restaurant having dinner, the scene is safe. –Patient is 4-5 years old, appears limp. –Mother is present with patient's newly prescribed medication. –NOI appears to be respiratory distress. –Your partner runs to the ambulance to grab the “jump bag.”

24
Case Study (cont’d) Primary Assessment Findings –Patient moans with loud verbal stimuli. –Airway patent, breathing fast and labored. –Peripheral pulse is tachycardic. –Accessory muscle and nasal flaring noted. –Limp muscle tone, ashen skin color.

25
Case Study (cont’d) Is this patient a high or low priority? Why? Why is the pulse tachycardic and tachypneic? What is causing the nasal flaring and retractions?

26
Case Study (cont’d) Medical History –Mother states the child was diagnosed yesterday with “respiratory problem” by pediatrician. Medications –Physician prescribed MDI (filled today). Allergies –None per the patient's mother.
. Allergies –None per the patient s mother..")
27
Case Study (cont’d) Pertinent Secondary Assessment Findings –Objective respiratory distress noted. –Coarse inspiratory and expiratory wheezing. –Absent alveolar breath sounds. –Pulse oximeter reads 84% on room air.

28
Case Study (cont’d) Pertinent Secondary Assessment Findings –Slight JVD noted. –Skin ashen, cool, diaphoretic. –Peripheral pulse present at 138/min, respirations are 46/min.

29
Case Study (cont’d) What pathologic change is causing the abnormal breath sounds? What respiratory condition does this patient likely have? What would be three assessment findings that could confirm your suspicion?

30
Case Study (cont’d) How would you best ascertain if this patient is breathing adequately? Why would this patient be prescribed this medication by the pediatrician? Given this patient’s presentation, would it be beneficial to give the drug?

31
Case Study (cont’d) Care provided: –Positioned supine on wheeled cot. –PPV initiated with high-flow oxygen. –Administered a beta-2-specific agonist. –Expeditious transport to the hospital.

32
Case Study (cont’d) If the patient improves, what would be the expected findings with: –Vital signs –Pulse oximeter –Breath sounds –Degree of respiratory distress
 If the patient improves, what would be the expected findings with: –Vital signs –Pulse oximeter –Breath sounds –Degree of respiratory distress")
33
Case Study (cont’d) What would be the likely assessment findings should the patient continue to deteriorate despite treatment?
 What would be the likely assessment findings should the patient continue to deteriorate despite treatment")
34
Summary Lower airway diseases many times will present with very similar findings. The goal is to match the patient's history with the summation of clinical findings to arrive at the correct field impression.

35
Summary (cont’d) Regardless, though, any patient that is breathing inadequately needs to be ventilated no matter what the disease etiology is.
 Regardless, though, any patient that is breathing inadequately needs to be ventilated no matter what the disease etiology is.")
Similar presentations













. In 1995, asthma hospitalizations.>")





