Download presentation
Presentation is loading. Please wait.

1
Diagnosis of Dementia and Use of Anti-dementia Medications
Prof Philip Morris MB BS, BSc(med), PhD, FRANZCP, FAChAM (RACP) Consultant Psychiatrist/Neuropsychiatrist Medical Advisor – DBMAS NT Medical Director Gold Coast – Tweed Memory Clinic 36 Beryl St, Tweed Heads, NSW, Australia Ph and Suite 2, Level 5, 123 Nerang St, Southport, Qld, Australia Ph
, PhD, FRANZCP, FAChAM (RACP) Consultant Psychiatrist/Neuropsychiatrist. Medical Advisor – DBMAS NT. Medical Director. Gold Coast – Tweed Memory Clinic. 36 Beryl St, Tweed Heads, NSW, Australia. Ph and. Suite 2, Level 5, 123 Nerang St, Southport, Qld, Australia. Ph")
2
Presentation Objectives
1. Recognize and assess significant cognitive impairment in older individuals The 'anatomy' of memory - 'Normal' versus 'Pathological' memory changes with aging - Bedside or office testing of cognitive function 2. Understand the clinical presentation and nature of common dementia syndromes Common dementia clinical syndromes - Alzheimer's disease - Vascular cognitive impairment - Frontotemporal dementia - behavioural, semantic and progressive aphasia types - Dementia with Lewy bodies - Subcortical dementias - Parkinson's disease dementia - Alcohol, traumatic brain injury, multiple sclerosis, motor neuron disease, Huntington'sdisease, AIDS and other dementias - Routine investigations in dementia 3. Determine which patients might benefit from anti-dementia drugs and other psychotropics Target symptoms for medications - Alertness and attention/concentration – Memory – Motivation - Improve speech - Improve mood - Reduce anxiety - Reduce psychotic symptoms - Reduce agitation and aggression Common nootropics and psychotropics in dementia - Acetyl cholinesterase inhibitors - Memantine (NMDA receptor antagonist) – Benzodiazepines – Antidepressants – Antipsychotics - Anticonvulsants and mood stabilizers 4. Appreciate the safety concerns using anti-dementia and psychotropic drugs in older patients Cardiac effects - Sedation and falls - Epileptogenic effects - Increased mortality
 – Benzodiazepines – Antidepressants – Antipsychotics - Anticonvulsants and mood stabilizers. 4. Appreciate the safety concerns using anti-dementia and psychotropic drugs in older patients. Cardiac effects - Sedation and falls - Epileptogenic effects - Increased mortality.")
3
Lateral Brain Motor cortex Somatosensory cortex Pars
opercularis Sensory associative cortex Visual associative cortex Visual cortex Broca’s area Primary Auditory cortex Wernicke’s area

4
Limbic Brain

5
Spatial relations Numbers Word understanding Word production Vision Problem solving Planning Behavioural control Emotion Attention and arousal Memory Emotion (Limbic system - not visible)
")
7
Subjective memory complaints
Disorientation forget time, place, trace of time Disorganization forget appointments, instructions Omission leave things behind, losing things, forgetting lights Repetition asking same question, telling same story All can occur in healthy people! Testing memory – list of words and cues – verbal recall

8
Assessment Memory problems Cortical regions involved
Assessment Memory problems Cortical regions involved Frontal (judgment, reasoning, finances, attention, planning, motivation, impulsivity) Temporal (memory, word finding, remembering names, irritability, misinterpretations) Parietal (disorientation, spatial misjudgment, left- right confusion, dressing apraxias)
 Temporal (memory, word finding, remembering names, irritability, misinterpretations) Parietal (disorientation, spatial misjudgment, left- right confusion, dressing apraxias)")
9
Structure of Memory Memory – 3 Rs: registration (encode - needs attention and arousal), retain (store), and recall (retrieve) Implicit/procedural Declarative/explicit (unconscious) (conscious) (learning of skills and (learning of information) automatic behaviours) Motor/conditioning/priming Working/short term memory (over seconds) (over seconds to minutes) Phonological loop Visuo-spatial sketch pad Long term memory (over days) Semantic memory (knowledge and memory about things) Episodic memory (narrative memories)
 (conscious) (learning of skills and (learning of information) automatic behaviours) Motor/conditioning/priming Working/short term memory (over seconds) (over seconds to minutes) Phonological loop. Visuo-spatial sketch pad. Long term memory (over days) Semantic memory. (knowledge and memory about things) Episodic memory. (narrative memories)")
10
Neuroanatomy of Memory Episodic memory – limbic system and hippocampus Semantic memory – widely distributed in cortex Implicit memory – basal ganglia, cerebellum, spinal cord Disorders of Memory Disorders of working memory - problems with attention and ‘central executive function’ - the ‘scratchpad’ or RAM Disorders of episodic memory - inability to retain new information/material (amnesia) - hippocampus based Disorders of semantic memory (knowledge) - more difficult to erode, less affected by disease Disorders of ‘metamemory’ - inability to judge own memory function - insight
 - hippocampus based. Disorders of semantic memory (knowledge) - more difficult to erode, less affected by disease. Disorders of ‘metamemory’ - inability to judge own memory function - insight.")
11
Subjective cognitive complaints (SCC)
Benign course, forgets names, misplaces things, needs more reminders, reduced concentration and increased distraction, anxiety and depression, excess demand Cognitive impairment not dementia (CIND) also known as mild cognitive impairment (MCI) 1/3 better, 1/3 same, 1/3 worse over two years MCI single domain – amnesic MCI multiple domain – memory, concentration, complex activities (cooking, finances), new learning Early dementia Multi domain impairment plus functional effects and impairments on instrumental ADLs
 also known as mild cognitive impairment (MCI) 1/3 better, 1/3 same, 1/3 worse over two years. MCI single domain – amnesic. MCI multiple domain – memory, concentration, complex activities (cooking, finances), new learning. Early dementia. Multi domain impairment plus functional effects and impairments on instrumental ADLs.")
12
Mild Cognitive Impairment – Sub-types
• Mild Cognitive Impairment (MCI) is considered a transitional state between ‘normal’ cognitive changes of ageing and the earliest clinical presentation of dementia. The original definition of amnestic MCI has empirical support as a prodrome to Alzheimer’s disease with conversion rates of 10-15% per year. • MCI is now recognised as a heterogeneous syndrome and diagnostic criteria have been broadened to include 4 clinical subtypes * Amnestic MCI single domain (aMCI) – memory impairment only * Amnestic MCI multiple domain (maMCI) – impairment in memory + other cognitive domain(s) * Non-amnestic MCI single domain (nMCI) – impairment in a single nonmemory domain * Non-amnestic MCI multiple domain (mnMCI) – impairment in multiple non-memory domains. • Individuals with MCI affecting multiple domains may be more severely cognitively impaired and represent a more advanced prodromal stage.
 is considered a transitional state between ‘normal’ cognitive changes of ageing and the earliest clinical presentation of dementia. The original definition of amnestic MCI has empirical support as a prodrome to Alzheimer’s disease with conversion rates of 10-15% per year. • MCI is now recognised as a heterogeneous syndrome and diagnostic. criteria have been broadened to include 4 clinical subtypes. * Amnestic MCI single domain (aMCI) – memory impairment only. * Amnestic MCI multiple domain (maMCI) – impairment in memory + other cognitive domain(s) * Non-amnestic MCI single domain (nMCI) – impairment in a single nonmemory domain. * Non-amnestic MCI multiple domain (mnMCI) – impairment in multiple. non-memory domains. • Individuals with MCI affecting multiple domains may be more severely. cognitively impaired and represent a more advanced prodromal stage.")
13
Dementia ‘epidemic’ explodes. Main types of dementia
Dementia ‘epidemic’ explodes Main types of dementia Alzheimer’s disease (35%) Vascular dementia (20%) Mixed Alzheimer’s/vascular (20%) Dementia with Lewy bodies (10%) Focal lobar atrophies (frontal variant FTD, semantic dementia, progressive non-fluent aphasia, and motor neuron dementia) (5%) Sub cortical dementias (Parkinson’s disease, progressive supranuclear palsy, multiple system atrophy, Huntington’s disease) (5%) Alcohol related (3%) Head injury (2%) Memory loss a cardinal feature of dementia along with either aphasia, apraxia, agnosia or a disturbance of executive functioning (planning, organizing, sequencing, abstracting)
 Vascular dementia (20%) Mixed Alzheimer’s/vascular (20%) Dementia with Lewy bodies (10%) Focal lobar atrophies (frontal variant FTD, semantic dementia, progressive non-fluent aphasia, and motor neuron dementia) (5%) Sub cortical dementias (Parkinson’s disease, progressive supranuclear palsy, multiple system atrophy, Huntington’s disease) (5%) Alcohol related (3%) Head injury (2%) Memory loss a cardinal feature of dementia along with either aphasia, apraxia, agnosia or a disturbance of executive functioning (planning, organizing, sequencing, abstracting)")
14
Dementia Conditions Most Common Dementias
Less than 1% of the under age 65 population compared with 20% of over 80s individuals Most Common Dementias Alzheimer’s disease Vascular dementia Dementia with Lewy bodies Frontotemporal dementia Most common. Inflammatory plaques of amyloid outside neurones, and deposition of tau tangles inside neurones. Initially concentrated in hippocampus and acetylcholine producing neurones. First causes learning and recent memory problems, and attention difficulties. Early onset Alzheimer’s disease more often inherited (chromosomes 14, 1, and 21 including Down’s syndrome)
")
15
Vascular dementia Multi-infarct dementia and Binswanger’s disease (deep white matter ischemia or subcortical vascular dementia) Vascular risk factors prominent (smoking, high blood pressure, diabetes, high lipids/cholesterol) Early onset may indicate an inherited Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL). Causes migranes, recurrent strokes and dementia. Chromosome 19 NOTCH3 gene mutation. Some early onset vascular dementias are autoimmune conditions affecting blood vessels in brain and may be treatable Memory less affected compared with Alzheimer’s disease. Frontal lobe executive functions, language, emotion and apathy, walking problems and incontinence more prominent. Stepwise deterioration
 Early onset may indicate an inherited Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL). Causes migranes, recurrent strokes and dementia. Chromosome 19 NOTCH3 gene mutation. Some early onset vascular dementias are autoimmune conditions affecting blood vessels in brain and may be treatable. Memory less affected compared with Alzheimer’s disease. Frontal lobe executive functions, language, emotion and apathy, walking problems and incontinence more prominent. Stepwise deterioration.")
16
Differentiating Alzheimer’s disease and vascular dementia
The most important differential diagnosis is between AD and VD, although in some cases AD and VD will overlap. Some key differences between the two diseases are listed on the slide.

17
Frontotemporal dementia
Previously known as Pick’s disease Second most common degenerative disease causing dementia in younger adults (after Alzheimer’s disease) More localised damage in frontal or temporal lobes causing changes in personality, language skills, and later memory Pathology includes severe loss of neurones (causing focal atrophy), as well as deposition of tau protein as ‘Pick bodies’ in neurones and accumulation of ubiquitin protein. A small number (20%) of cases are due to chromosome 17 mutations (tau and progranulin genes). Three clinical presentations of frontotemporal dementia Behavioural variant Personality change most distinctive – loss of empathy and warmth, apathy, and disinhibition. Poor judgment, reasoning, planning and organisation. Reduction in conversation, eating changes, decline in self-care and loss of independent ADLs. Progressive aphasia – semantic dementia (fluent) Loss of memory for words, impaired comprehension of word meaning, reading and spelling affected, numerical abilities preserved. Progressive nonfluent aphasia Slow and tortuous production of words causing distortion of speech, wrong words and grammatical errors. Problems with using telephone or talking in groups. Apraxia of hand movements Both types of aphasia can progress to behavioural disturbance
 More localised damage in frontal or temporal lobes causing changes in personality, language skills, and later memory. Pathology includes severe loss of neurones (causing focal atrophy), as well as deposition of tau protein as ‘Pick bodies’ in neurones and accumulation of ubiquitin protein. A small number (20%) of cases are due to chromosome 17 mutations (tau and progranulin genes). Three clinical presentations of frontotemporal dementia. Behavioural variant. Personality change most distinctive – loss of empathy and warmth, apathy, and disinhibition. Poor judgment, reasoning, planning and organisation. Reduction in conversation, eating changes, decline in self-care and loss of independent ADLs. Progressive aphasia – semantic dementia (fluent) Loss of memory for words, impaired comprehension of word meaning, reading and spelling affected, numerical abilities preserved. Progressive nonfluent aphasia. Slow and tortuous production of words causing distortion of speech, wrong words and grammatical errors. Problems with using telephone or talking in groups. Apraxia of hand movements. Both types of aphasia can progress to behavioural disturbance.")
18
Parkinsonian disorders associated with dementia
Parkinson’s disease Pathology of Lewy bodies (clumps of alpha-synuclein protien) in substantia nigra region of brain stem 20% to 40% later develop dementia characterised by difficulties with abstract thought, memory, behavioural regulation and visual hallucinations. Dementia with Lewy bodies Similar pathology to Parkinson’s disease, but in addition plaques and tangles A ‘cross’ between Parkinson’s disease and Alzheimer’s disease – cognitive features of Alzheimer’s disease with movement disorder of Parkinson’s disease (‘Parkinson’s plus’). Vivid visual hallucinations (faces, animals), rapid fluctuations of alertness, and falls are common Attention is impaired more than memory Copying shapes and understanding visual material is affected Sensitive to antipsychotic medication, may respond to ACEIs Progressive supranuclear palsy Rigid Parkinson’s disease, gaze palsy, swallowing problems and frontal dementia Corticobasal degeneration (CBD) Rigidity, bradykinesia, apraxia (‘alien limb’ syndrome), and behavioural variant of frontotemporal dementia
 in substantia nigra region of brain stem. 20% to 40% later develop dementia characterised by difficulties with abstract thought, memory, behavioural regulation and visual hallucinations. Dementia with Lewy bodies. Similar pathology to Parkinson’s disease, but in addition plaques and tangles. A ‘cross’ between Parkinson’s disease and Alzheimer’s disease – cognitive features of Alzheimer’s disease with movement disorder of Parkinson’s disease (‘Parkinson’s plus’). Vivid visual hallucinations (faces, animals), rapid fluctuations of alertness, and falls are common. Attention is impaired more than memory. Copying shapes and understanding visual material is affected. Sensitive to antipsychotic medication, may respond to ACEIs. Progressive supranuclear palsy. Rigid Parkinson’s disease, gaze palsy, swallowing problems and frontal dementia. Corticobasal degeneration (CBD) Rigidity, bradykinesia, apraxia (‘alien limb’ syndrome), and behavioural variant of frontotemporal dementia.")
19
Less Common Early Onset Dementias
Motor Neurone Disease with dementia Huntington’s disease Alcohol related dementia and Korsakoff’s syndrome Multiple sclerosis HIV-related dementia

20
Rare Causes of Younger Onset Dementia
Creutzfeldt-Jacob disease (CJD) Dementia after head injury Dementia in Down syndrome Homocystinuria Vasculitis Wilson’s disease Porphyria Adrenoleukodystrophy Lipid storage diseases Mitochondrial disorders Dentatorubralpallidoluysian atrophy (DRPLA) Neuroacanthocytosis
 Dementia after head injury. Dementia in Down syndrome. Homocystinuria. Vasculitis. Wilson’s disease. Porphyria. Adrenoleukodystrophy. Lipid storage diseases. Mitochondrial disorders. Dentatorubralpallidoluysian atrophy (DRPLA) Neuroacanthocytosis.")
21
History taking questions
Recent narrative memory, past narrative memory, people's names, names items, learning problems, forgetting things and appointments, word finding problems, comprehension and expression problems, semantic difficulties, topographical disorientation, R/L disorientation, dressing and other apraxias, gait problems, posture, EPS, involuntary movements, incontinence, confusion episodes, mood and affect, psychotic symptoms, motivation and passivity, personality changes, agitation, aggression, planning and sequencing problems, sleep, appetite, weight, ADLs, cooking, shopping, driving

22
The Clinical Problem Age Related Changes or Subjective Cognitive Complaints (SCC) Vs Mild Cognitive Impairment (MCI) or Cognitive Impairment Not Dementia (CIND) Early Dementia?
 or Cognitive Impairment Not Dementia (CIND) Early Dementia")
23
Beyond the Mini Mental State Exam
Beyond the Mini Mental State Exam? The Addenbrooke’s Cognitive Examination

24
Int J Geriatr Psychiatry 2006; 21: 1078–1085.
The Addenbrooke’s Cognitive Examination Revised (ACE-R): a brief cognitive test battery for dementia screening Eneida Mioshi1,2, Kate Dawson2, Joanna Mitchell2, Robert Arnold1 and John R. Hodges1,2* 1MRC Cognition and Brain Sciences Unit, Cambridge, UK 2University of Cambridge Department of Clinical Neurosciences, Addenbrooke’s Hospital, Cambridge, UK SUMMARY There is a clear need for brief, but sensitive and specific, cognitive screening instruments as evidenced by the popularity of the Addenbrooke’s Cognitive Examination (ACE). Objectives We aimed to validate an improved revision (the ACE-R) which incorporates five sub-domain scores (orientation/attention, memory, verbal fluency, language and visuo-spatial). Methods Standard tests for evaluating dementia screening tests were applied. A total of 241 subjects participated in this study (Alzheimer’s disease=67, frontotemporal dementia=55, dementia of Lewy Bodies=20; mild cognitive impairment–MCI=36; controls=63). Results Reliability of the ACE-R was very good (alpha coefficient=0.8). Correlation with the Clinical Dementia Scale was significant (r=0.321, p <0.001). Two cut-offs were defined (88: sensitivity=0.94, specificity=0.89; 82: Sensitivity=0.84, specificity=1.0). Likelihood ratios of dementia were generated for scores between 88 and 82: at a cut-off of 82 the likelihood of dementia is 100:1. A comparison of individual age and education matched groups of MCI, AD and controls placed the MCI group performance between controls and AD and revealed MCI patients to be impaired in areas other than memory (attention/orientation, verbal fluency and language). Conclusions The ACE-R accomplishes standards of a valid dementia screening test, sensitive to early cognitive dysfunction.
: a brief cognitive test battery for dementia screening. Eneida Mioshi1,2, Kate Dawson2, Joanna Mitchell2, Robert Arnold1 and John R. Hodges1,2* 1MRC Cognition and Brain Sciences Unit, Cambridge, UK. 2University of Cambridge Department of Clinical Neurosciences, Addenbrooke’s Hospital, Cambridge, UK. SUMMARY. There is a clear need for brief, but sensitive and specific, cognitive screening instruments as evidenced by the popularity of the Addenbrooke’s Cognitive Examination (ACE). Objectives. We aimed to validate an improved revision (the ACE-R) which incorporates five sub-domain scores. (orientation/attention, memory, verbal fluency, language and visuo-spatial). Methods. Standard tests for evaluating dementia screening tests were applied. A total of 241 subjects participated in this study (Alzheimer’s disease=67, frontotemporal dementia=55, dementia of Lewy Bodies=20; mild cognitive impairment–MCI=36; controls=63). Results. Reliability of the ACE-R was very good (alpha coefficient=0.8). Correlation with the Clinical Dementia Scale. was significant (r=0.321, p <0.001). Two cut-offs were defined (88: sensitivity=0.94, specificity=0.89; 82: Sensitivity=0.84, specificity=1.0). Likelihood ratios of dementia were generated for scores between 88 and 82: at a cut-off of 82 the likelihood of dementia is 100:1. A comparison of individual age and education matched groups of MCI, AD and controls placed the MCI group performance between controls and AD and revealed MCI patients to be impaired in areas other than memory (attention/orientation, verbal fluency and language). Conclusions. The ACE-R accomplishes standards of a valid dementia screening test, sensitive to early cognitive. dysfunction.")
25
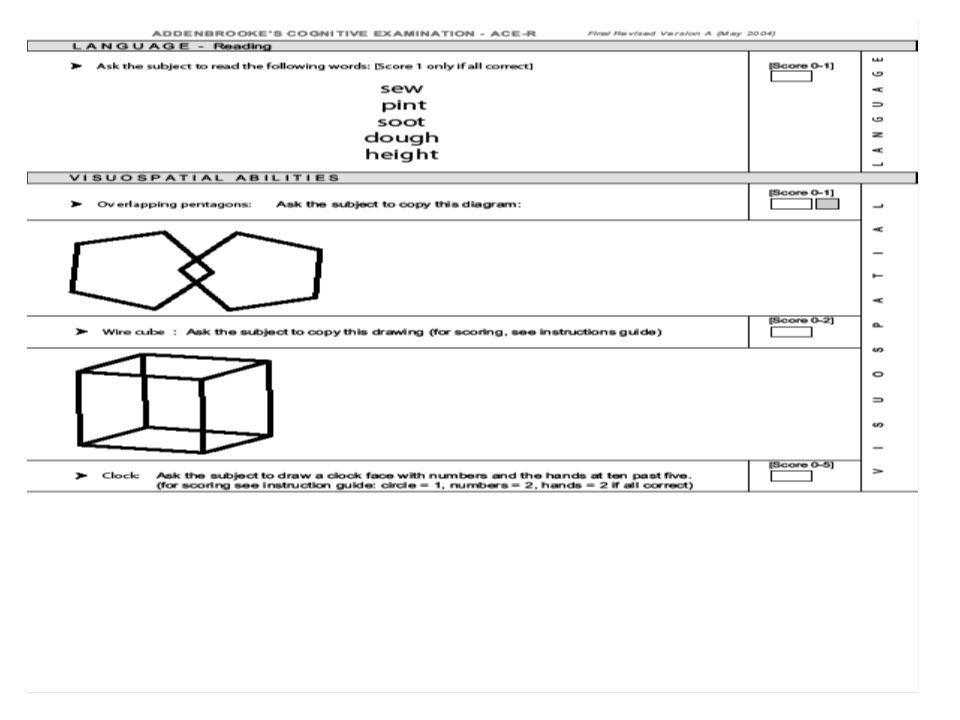
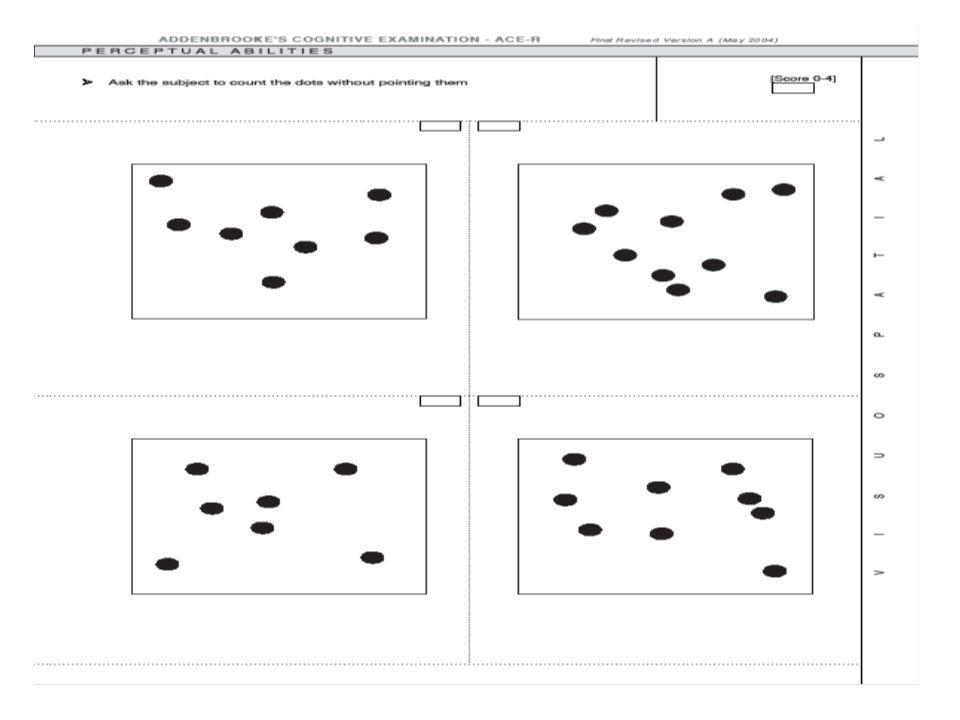
ADDENBROOKE'S COGNITIVE EXAMINATION - ACE-R
Prof John Hodges (Prince of Wales Hospital Randwick, NSW) Revised Version A (May 2004) - Australian Version Orientation (time and place)* Registration (three words)* Attention and concentration (“world” backwards, serial 7s)* Memory - recall (three words)* Memory - anterograde memory (learning name and address) Memory - retrograde memory (recent and past historical figures) Verbal fluency - letter P [phonemic fluency] and animals [semantic fluency] Language - comprehension (follow written instruction and three stage command)* Language – writing (sentence)* Language – repetition (words and phrases)* Language - naming (pictures) Language - comprehension (pictures) Language - reading (words) Visuo-spatial abilities (copying figures* and clock drawing) Visuo-spatial perceptual abilities (count dots and identify letters) Memory - recall (name and address) Memory - recognition (name and address) Overall score (max 100; below mid 80s suggests dementia) *Includes MMSE score (max 30; below mid 20s suggests dementia)
 Revised Version A (May 2004) - Australian Version. Orientation (time and place)* Registration (three words)* Attention and concentration ( world backwards, serial 7s)* Memory - recall (three words)* Memory - anterograde memory (learning name and address) Memory - retrograde memory (recent and past historical figures) Verbal fluency - letter P [phonemic fluency] and animals [semantic fluency] Language - comprehension (follow written instruction and three stage command)* Language – writing (sentence)* Language – repetition (words and phrases)* Language - naming (pictures) Language - comprehension (pictures) Language - reading (words) Visuo-spatial abilities (copying figures* and clock drawing) Visuo-spatial perceptual abilities (count dots and identify letters) Memory - recall (name and address) Memory - recognition (name and address) Overall score (max 100; below mid 80s suggests dementia) *Includes MMSE score (max 30; below mid 20s suggests dementia)")
32
Neuropsychological Testing
Refer to Neuropsychologist Pen and paper testing, up to 4 hours, but can be reduced to 2 hours Can be expensive Or Touch-screen, computer-based neuropsychological testing Brain Resource Company (BRC) Integneuro program No keyboard skills required Takes about 1.5 hours Best for patients with MMSE score 25 and above Some patients need assistance
 Integneuro program. No keyboard skills required. Takes about 1.5 hours. Best for patients with MMSE score 25 and above. Some patients need assistance.")
34
Memory Clinic Program Initial Consultation The initial consultation involves a medical review, a mental health assessment, and a memory and cognitive screening evaluation. Investigations Further comprehensive assessment procedures include a touch screen, computer-based diagnostic and baseline neuropsychological assessment of memory and cognitive function, laboratory blood tests, EEG/QEEG, ECG, structural & functional brain imaging tests (CT/MRI, SPECT, Doppler carotid ultrasound), and interviews with family or carer. Second Consultation At a second consultation the results of all tests are reviewed with the patient (and family/carer) and a diagnosis determined. A personalized management plan is then developed. Memory Rehabilitation Program A unique 12-session (24 hours total) Memory Rehabilitation Program is offered to reduce risk factors for memory loss and to enhance protective factors for preserving memory function. Follow-up Assessment of clinical and cognitive status. At further consultations the plan is monitored and reviewed in collaboration with the GP/local doctor.
, and interviews with family or carer. Second Consultation. At a second consultation the results of all tests are reviewed with the patient (and family/carer) and a diagnosis determined. A personalized management plan is then developed. Memory Rehabilitation Program. A unique 12-session (24 hours total) Memory Rehabilitation Program is offered to reduce risk factors for memory loss and to enhance protective factors for preserving memory function. Follow-up. Assessment of clinical and cognitive status. At further consultations the plan is monitored and reviewed in collaboration with the GP/local doctor.")
35
MRI brain saggital view

36
MRI brain trans-axial or cross-sectional view

37
Brain atrophy – general and hippocampus – coronal view

38
MRI trans-axial view – deep white matter ischemia

41
Providing a rationale for treatment: Dementia
The diagram on the slide, or a similar diagram, could be used as a tool when providing a treatment rationale for dementia.

42
Effects of treatment on target symptoms
Antidepressant agents are helpful in managing depressive symptoms in patients with dementia. Antipsychotic agents are useful in managing psychotic symptoms and associated behavioural disturbance. Atypical antipsychotic agents are preferred due to reduced risk of adverse side effects. Care should be taken to exclude patients with DLB.

43
Cognitive Enhancing Drugs - Nootropics
Acetyl cholinesterase inhibitors Donepezil Glamtamine Rivastigmine NMDA receptor agonist Memantine

44
Acetylcholinsterase Inhibitors (AChEIs)
Evidence from studies indicate: AChEIs are effective in the treatment of mild to moderate AD 40-50% of patients show improvement in cognitive symptoms and delay in progression of illness Improvement in non-cognitive symptoms (apathy, hallucinations, behaviour disturbance) are reported Benefits last between 6 months to 2 years eg. Donepezil 5mg nocte to start, 10mg after one month N-methyl-D-aspartate (NMDA)-receptor antagonist - Memantine Block glutamate toxicity Effective in moderate - severe AD Combination therapy – AChEIs plus Memantine
 are reported. Benefits last between 6 months to 2 years. eg. Donepezil 5mg nocte to start, 10mg after one month. N-methyl-D-aspartate (NMDA)-receptor antagonist - Memantine. Block glutamate toxicity. Effective in moderate - severe AD. Combination therapy – AChEIs plus Memantine.")
45
Acetylcholinsterase Inhibitors (AChEIs)
Evidence from studies indicate: AChEIs are effective in the treatment of mild to moderate AD 40-50% of patients show improvement in cognitive symptoms and delay in progression of illness Improvement in non-cognitive symptoms (apathy, hallucinations, behaviour disturbance) are reported Benefits last between 6 months to 2 years
 are reported. Benefits last between 6 months to 2 years.")
46
Management of Dementia with Lewy Bodies
Patients demonstrate neuroleptic sensitivity AChEIs have been shown to improve cognition, psychotic symptoms and neuropsychiatric symptoms in some patients with DLB Evidence is accumulating for the use of AChEIs as first-line pharmacological treatment of cognitive dysfunction, apathy, psychosis and agitation in some patients (McKeith, 2002, p. 146) If DLB is suspected, patients should be referred for specialist assessment. Patients demonstrate neuroleptic sensitivity, so specialist advice should be sought before prescribing antipsychotic agents to patients who present with features of dementia, depression and fluctuating cognition. AChEIs have been shown to improve cognition, psychotic symptoms and neuropsychiatric symptoms in some patients with DLB. Evidence is also accumulating for the use of AChEIs as first-line pharmacological treatment of cognitive dysfunction, apathy, psychosis and agitation in some patients. (McKeith, 2002, p. 146)
 If DLB is suspected, patients should be referred for specialist assessment. Patients demonstrate neuroleptic sensitivity, so specialist advice should be sought before prescribing antipsychotic agents to patients who present with features of dementia, depression and fluctuating cognition. AChEIs have been shown to improve cognition, psychotic symptoms and neuropsychiatric symptoms in some patients with DLB. Evidence is also accumulating for the use of AChEIs as first-line pharmacological treatment of cognitive dysfunction, apathy, psychosis and agitation in some patients. (McKeith, 2002, p. 146)")
47
Frontotemporal dementia – associated features
Patients with FTD may present with slowness and apathy or restlessness, overactivity, distractibility and disinhibition Neurological signs of Parkinsonism, rigidity, dyspraxia, dysarthria, tremor or ocular problems occur with disease progression Pharmacological treatments are limited; there have been reports of some symptomatic response to SSRIs, possibly AChEIs Patients with FTD may present with slowness and apathy or restlessness, overactivity, distractibility and disinhibition. Neurological signs of Parkinsonism, rigidity, dyspraxia, dysarthria, tremor or ocular problems occur with disease progression. Pharmacological treatments are limited; although there have been reports of some symptomatic response to SSRIs.

48
Acetyl cholinesterase inhibitors Memantine Atypical antipsychotics
Safety Concerns Acetyl cholinesterase inhibitors Memantine Atypical antipsychotics

49
Memory Rehabilitation Program
Lifestyle Interventions** [ ] Exercise - 30 min walking (or equivalent) per day five days a week [ ] Resistance strength exercises three times a week for 20 min [ ] Reduce weight, BMI and abdominal girth [ ] Diet – low saturated fat Mediterranean style diet (colored vegetables, monounsaturated oils, lots of fish, garlic) [ ] Reduce alcohol (max. 2 standard drinks per day), no tobacco, no drugs [ ] Social interaction [ ] Intellectual stimulation [ ] Active leisure pursuits [ ] Protect the head Nutrient Supplements [ ] Mega-folate (5 mg per day) [ ] Multivitamins (antioxidants [vitamins A, D, C, E], B-group vitamins [B1, B2, B3, B6, B12], and trace elements [copper, iodine, manganese, phosphate, selenium]) [ ] Omega 3 fish oil capsules (DHA long chain type) Memory and Cognition Training** [ ] Memory aids and techniques (books, guides) [ ] Computer-based and counselor-guided memory training programs Stress Management** [ ] Stress reduction, increase resilience, and manage depression and anxiety Community Organizations [ ] Alzheimer’s Australia (Living with Memory Loss courses) Ph Medical Interventions [ ] Low dose aspirin (or other blood thinner) [ ] Blood pressure control [ ] Anti-cholesterol and anti-triglyceride medications (satins) Memory enhancing medications (nootropics) [ ] Acetyl-cholinesterase inhibitor drugs [ ] Memantine [ ] Others Accommodation and home care support [ ] ACAT assessment ** Included in the Memory Rehabilitation Program
 per day five days a week. [ ] Resistance strength exercises three times a week for 20 min. [ ] Reduce weight, BMI and abdominal girth. [ ] Diet – low saturated fat Mediterranean style diet (colored vegetables, monounsaturated oils, lots of fish, garlic) [ ] Reduce alcohol (max. 2 standard drinks per day), no tobacco, no drugs. [ ] Social interaction. [ ] Intellectual stimulation. [ ] Active leisure pursuits. [ ] Protect the head. Nutrient Supplements. [ ] Mega-folate (5 mg per day) [ ] Multivitamins (antioxidants [vitamins A, D, C, E], B-group vitamins [B1, B2, B3, B6, B12], and trace elements [copper, iodine, manganese, phosphate, selenium]) [ ] Omega 3 fish oil capsules (DHA long chain type) Memory and Cognition Training** [ ] Memory aids and techniques (books, guides) [ ] Computer-based and counselor-guided memory training programs. Stress Management** [ ] Stress reduction, increase resilience, and manage depression and anxiety. Community Organizations. [ ] Alzheimer’s Australia (Living with Memory Loss courses) Ph Medical Interventions. [ ] Low dose aspirin (or other blood thinner) [ ] Blood pressure control. [ ] Anti-cholesterol and anti-triglyceride medications (satins) Memory enhancing medications (nootropics) [ ] Acetyl-cholinesterase inhibitor drugs. [ ] Memantine. [ ] Others. Accommodation and home care support. [ ] ACAT assessment. ** Included in the Memory Rehabilitation Program.")
Similar presentations







>")


, PhD, FRANZCP, FAChAM (RACP)>")















