Download presentation
Presentation is loading. Please wait.

1
Billing & Reimbursement of Integrated Health Services Presented by: Kathleen Reynolds, LMSW, ACSW Shauna Reitmeier, MSW

2
Overview What are the current issues your PBHCI initiative is facing in regards to Billing and Reimbursement Provide your organization with key steps it can take to maximize its Billing and Reimbursement opportunities in the following situations –Partnering models –Stand Alone Models Future steps related to billing and reimbursement Training and Technical Assistance for grantees

3
Expections of the Grant to Bill for Third Party Reimbursements If you are serving individuals who have Medicaid, Medicare or other third party payers, you should be billing the third party payer for those services and including that revenue as part of your PBHCI budget This is critical to financial sustainability once the grant period ends. Who bills for what service, when is a critical discussion needed for everyone to have?

4
Stand Alone Models In many states CMHC needs to apply for a new Medicaid # to bill for Primary Care Services Must apply first for Medicare # to get the Medicaid # Exception: In Ohio, CMHC’s with Risperdal license can bill for primary care Accreditation Considerations Depending on accrediting body (Joint Commission, CARF, NCQA) your organization may need to become accredited as an ambulatory care facility to provide physical health services. This whole process can take 2-3 years

5
Partner Models FQHC/CHC bill by encounter rates. Receive the same amount of funding for a 10 minutes visit as they do for a 1hour visit Contracting with FQHC/CHC’s Leasing Options for staff Psychiatrists Consulting Psychiatrist Model (Regional MHC Indiana) LICSW/LMSW Offset cost for Indigent population FQHC/CHC receive federal funds to cover the cost of indigent CMHC can provide Case Management
 LICSW/LMSW Offset cost for Indigent population FQHC/CHC receive federal funds to cover the cost of indigent CMHC can provide Case Management.")
6
Partner Model (cont.) 340B Pharmacy benefits Individual receiving services enrolled in FQHC/CHC Broader formulary Significantly reduced rate FQHC/CHC apply for change of scope Mirror scope of primary location to the new CMHC location Original scope has to include Behavioral Health or apply to have it included Allows for FQHC to bill for primary care services not able to be billed by CMHC Consumer needs to be enrolled with the FQHC/CHC
 340B Pharmacy benefits Individual receiving services enrolled in FQHC/CHC Broader formulary Significantly reduced rate FQHC/CHC apply for change of scope Mirror scope of primary location to the new CMHC location Original scope has to include Behavioral Health or apply to have it included Allows for FQHC to bill for primary care services not able to be billed by CMHC Consumer needs to be enrolled with the FQHC/CHC")
7
Uninsured FQHC/CHC federal funding to cover uninsured Increased # of insured can help offset cost of uninsured State Health Plans Discuss the ability to add a Behavioral Health Benefit Partner with Universities to be Student Teaching location 3 rd year medical students Nurse Practitioners Masters of Social Work

8
Basic Principles of Billing and Reimbursement Key pieces of information an organization needs to know to maximize reimbursable services –Medicaid Provider billing type (FQHC/CHC, CMHC or other) A successful bill requires three key pieces of information –CPT Codes (Current Procedural Terminology) –Diagnosis of the individual –Licensure and Credential of practitioner
 A successful bill requires three key pieces of information –CPT Codes (Current Procedural Terminology) –Diagnosis of the individual –Licensure and Credential of practitioner")
9
Interim Financing & Billing Worksheets These worksheets are designed to help agencies understand the series of factors to consider in their state, when billing for integrated health services using the public safety net system. –Type of Agency (FQHC/CHC, CMHC) –Funding Source (Medicare, Medicaid) –CPT Code –Diagnosis –Practitioner Discipline & Credential The worksheets are posted on the CIHS website under Finance as they are completed www.samhsa.integration.gov
 –Funding Source (Medicare, Medicaid) –CPT Code –Diagnosis –Practitioner Discipline & Credential The worksheets are posted on the CIHS website under Finance as they are completed")
10
Basic Principles of Billing and Reimbursement (con’t) CPT Codes (Current Procedural Terminology) –Evaluation and Management Codes (E&M) Is generally billed by an FQHC or Medical Facility and must have a physical health diagnosis –Health & Behavior Assessment Codes (HAB) Can only be billed by an FQHC or Medical Facility and must have an accompanying physical health diagnosis Used to identify the psychological, behavioral, emotional, cognitive and social factors important to the prevention, treatment, or management of physical health problems. The focus is not on mental health, but on the biopsychosocial factors important to physical health problems and treatments. Depending on the state the E&M and HAB codes can be billed on the same day

12
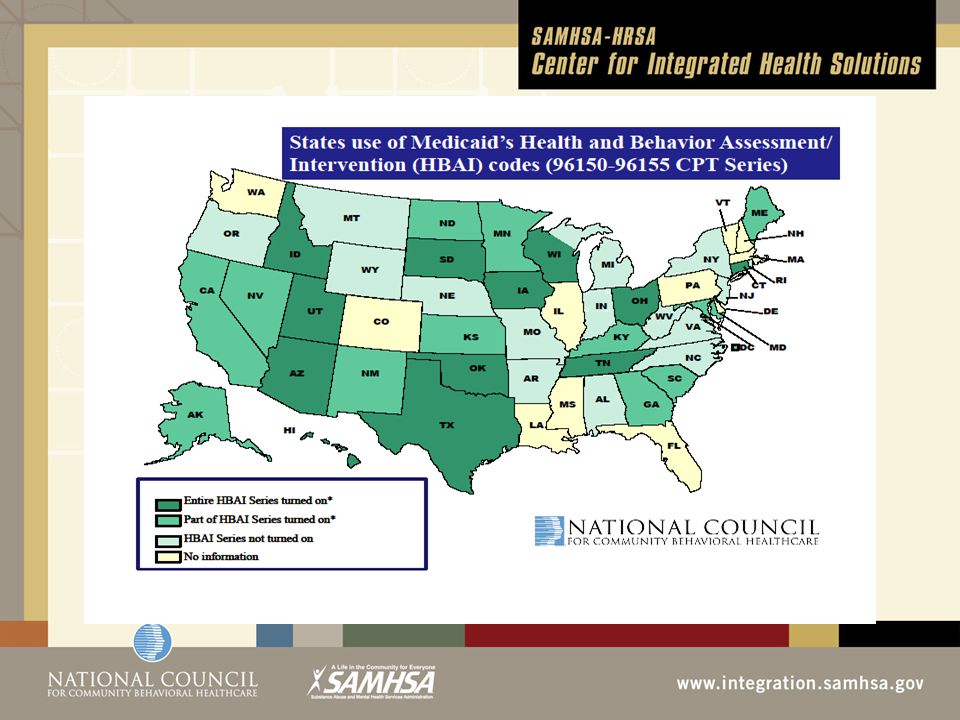
The Health and Behavior Assessment/Intervention Codes (96000 Series) Approved CPT Codes for use with Medicare right now Some states are using them now for Medicaid State Medicaid programs need to “turn on the codes” for use Behavioral Health Services “Ancillary to” a physical health diagnosis Diabetes COPD Chronic Pain
 Approved CPT Codes for use with Medicare right now Some states are using them now for Medicaid State Medicaid programs need to turn on the codes for use Behavioral Health Services Ancillary to a physical health diagnosis Diabetes COPD Chronic Pain")
13
Basic Principles of Billing and Reimbursement (cont.) CPT Codes (Current Procedural Terminology) –Behavioral Health Codes 908xx series (MH & SU) Traditional behavioral codes by an acceptable licensed and credentialed practitioner for that state and setting (Physician, Nurse Practitioner, Masters Social Worker, PhD Psychologist) –Telemedicine (usually the same code as face to face service with a modifier) Typically these services are billable by an acceptable licensed and credentialed practitioner for that state and setting –Case Management Can only be billed by an acceptable licensed and credentialed practitioner for that state and setting Generally a CMHC service
 CPT Codes (Current Procedural Terminology) –Behavioral Health Codes 908xx series (MH & SU) Traditional behavioral codes by an acceptable licensed and credentialed practitioner for that state and setting (Physician, Nurse Practitioner, Masters Social Worker, PhD Psychologist) –Telemedicine (usually the same code as face to face service with a modifier) Typically these services are billable by an acceptable licensed and credentialed practitioner for that state and setting –Case Management Can only be billed by an acceptable licensed and credentialed practitioner for that state and setting Generally a CMHC service")
15
Two Services in One Day Myth: The federal government prohibits this or Medicaid won’t pay for this! Reality: This is a state by state Medicaid issue, not a federal rule or regulation – Georgia does not allow two services in one day to be billed Federal Citations: ◦ Medicare will cover a physical health and mental health visit same day/same provider – CFR Title 42 Volume 2, Part 405. Section 405.2463 ◦ Medicaid confirmation received from Peggy Clark, (CMS/CMSO) – “In terms of FQHC’s/RHC’s there are no applicable, current (federal) Medicaid regulations, but some States follow Medicare requirements pertaining to same day billing. In terms of same day billing in the Community Mental Health Centers and Outpatient Hospital setting, there are no specific Medicaid statutes or regulations on this matter.
 – In terms of FQHC’s/RHC’s there are no applicable, current (federal) Medicaid regulations, but some States follow Medicare requirements pertaining to same day billing. In terms of same day billing in the Community Mental Health Centers and Outpatient Hospital setting, there are no specific Medicaid statutes or regulations on this matter..")
16
Two Services in one Day Currently billable in some states by one provider Two providers bill for the services they provide on the same day – Contractual Business Model Behavioral Health Provider bills for BH service under their provider number Primary Care bills for their services under their provider number

17
Next Steps & Questions COHORT 1 Grantees (to start with Cohort 2&3 to rollout next year) Availability to work with CIHS to develop Sustainability Plan Administrative Clinical Financial March – September monthly special interest/learning community calls related to financing based on Billing Basics, Partner or Stand Alone models
 Availability to work with CIHS to develop Sustainability Plan Administrative Clinical Financial March – September monthly special interest/learning community calls related to financing based on Billing Basics, Partner or Stand Alone models")
18
CONTACT INFORMATION Kathy Reynolds, LMSW, ACSW kathyr@thenationalcouncil.org 202-684-7457 x 241 Shauna Reitmeier, MSW shaunar@thenationalcouncil.org 202-684-7457 x 271

Similar presentations