Download presentation
Presentation is loading. Please wait.

1
Metodología y Objetivos
XIII Congreso Latinoamericano de Mastología VIII Congreso Chileno de Mastología Sheraton Santiago, Hotel & Convention Center de Noviembre 2005 SIMPOSIO GENETICA Y CANCER MAMA Estudio TransBIG (MINDACT) Metodología y Objetivos Dr. Alejandro Corvalán R. Departamento Anatomía Patológica, Pontificia Universidad Católica de Chile Grupo Oncológico Cooperativo Chileno de Investigación (GOCCHI)
 Metodología y Objetivos. Dr. Alejandro Corvalán R. Departamento Anatomía Patológica, Pontificia Universidad Católica de Chile. Grupo Oncológico Cooperativo Chileno de Investigación (GOCCHI)")
2
van’t Veer et al., Nature 2002; 155,530-36
positive negative

3
van’t Veer et al., Nature 2002; 155,530-36

4
Metástasis DFS N=34 N=44 St. Gallen 33 (97%) 31 (70%)
Comparación de criterios clínico-patológicos (St. Gallen y NIH) vs perfil genético en recaída (metástasis) y DFS (disease-free survival) en cáncer de mama Metástasis DFS N=34 N=44 St. Gallen 33 (97%) 31 (70%) NIH (94%) 40 (91%) Perfil genético 31 (91%) 12 (27%) van´t Veer et al., Nature 2002, 415:
 vs perfil genético en recaída (metástasis) y DFS (disease-free survival) en cáncer de mama. Metástasis DFS. N=34 N=44. St. Gallen 33 (97%) 31 (70%) NIH 32 (94%) 40 (91%) Perfil genético 31 (91%) 12 (27%) van´t Veer et al., Nature 2002, 415:")
6
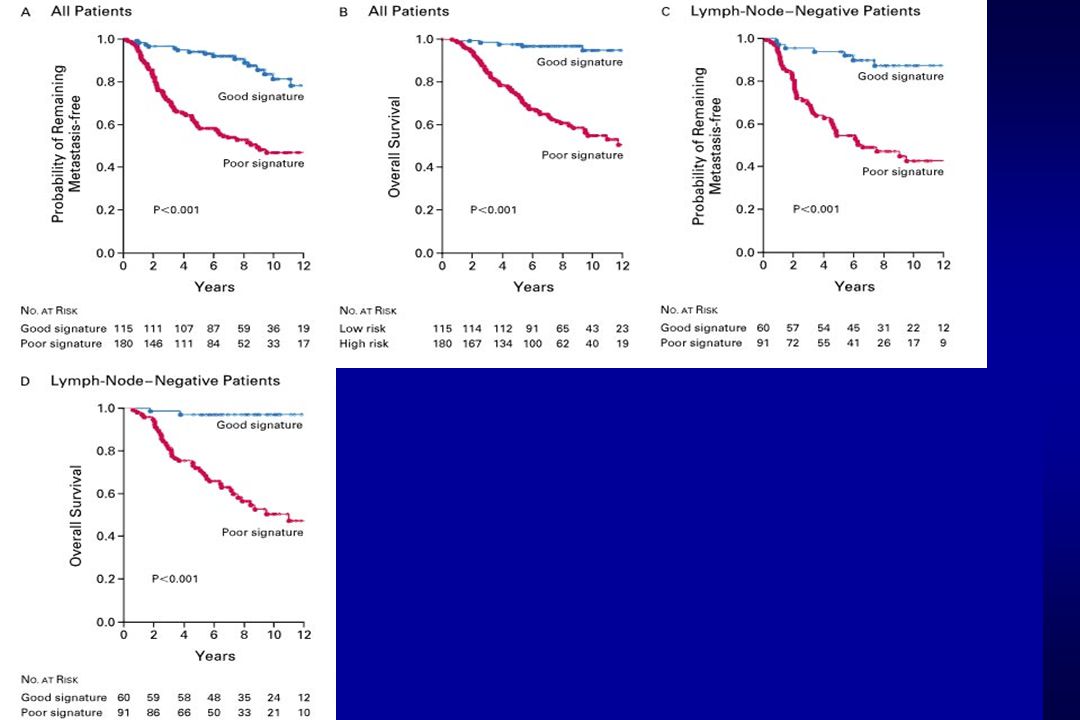
Clasificación de 295 pacientes con carcinoma primario de mama usando perfil de expresión génica asociado a buen y mal pronóstico Estadio II o III de cancer de mama Menores de 53 años 151 con linfonodos positivos 144 con linfonodos negativos

8

13
MINDACT Microarray In Node negative Disease may Avoid Chemotherapy
DESIGN UPDATE New design-MINDACT_FINAL_ Feb2005

14
TRANSLATING MOLECULAR KNOWLEDGE INTO EARLY BREAST CANCER MANAGEMENT

15
TRANSBIG TRANSBIG: International research network founded in EU supported Network of Excellence Aim: To integrate, strengthen and facilitate translational and clinical breast cancer research Total cost: € 24 million (EU contribution: € 7 million) 1st project: MINDACT clinical trial (Microarray for Node Negative Disease may Avoid Chemotherapy)
 1st project: MINDACT clinical trial (Microarray for Node Negative Disease may Avoid Chemotherapy)")
16
Australia/New Zealand
TRANSBIG: PARTNERS = Official partners European Union (Austria, Belgium, Denmark, France, Germany, Greece, Ireland, Italy, Luxemburg, The Netherlands, Portugal, Sweden and United Kingdom) + Turkey & Switzerland = Third party countries likely to participate Canada National Cancer Institute of Canada (NCIC), Clinical Trials Group (CTG) Russia Cancer Research Centre Chile Chilean Cooperative Group for Oncologic Research (GOCCHI) TRANSBIG current participating countries- with potential involvement of Canada and Australia in its trials Australia/New Zealand Australian New Zealand Breast Cancer Trials Group (ANZ BCTG) 39 PARTNERS, 21 COUNTRIES
 + Turkey & Switzerland. = Third party countries likely to participate. Canada. National Cancer Institute of. Canada (NCIC), Clinical Trials Group (CTG) Russia. Cancer Research Centre. Chile. Chilean Cooperative Group for Oncologic Research (GOCCHI) TRANSBIG current participating countries- with potential involvement of Canada and Australia in its trials. Australia/New Zealand. Australian New Zealand Breast Cancer Trials Group (ANZ BCTG) 39 PARTNERS, 21 COUNTRIES.")
17
TRANSBIG APPROACH: TRANSLATIONAL RESEARCH
Gene analysis “translated“ into tools to determine best clinical treatment « Tailors » treatment: individual patient individual tumour individual treatment AVOIDS OVERTREATMENT

18
TRANSBIG APPROACH: TRANSLATIONAL RESEARCH
Gene analysis “translated“ into tools to determine best clinical treatment « Tailors » treatment: individual patient individual tumour individual treatment AVOIDS OVERTREATMENT

19
WHAT IS MINDACT? Study based on a 70-gene "genetic signature" identified by the Netherlands Cancer Institute Hypothesis: The analysis of thousands of tumours with the genetic signature can lead to better understanding of breast cancer and treatment required for the individual Aim: Validate the hypothesis on 5000 women over 3 years Outcome: Save women from unnecessary treatment Develop new areas of medical research

20
Assess clinical risk and genomic risk
MINDACT – 6000 patients Assess clinical risk and genomic risk

21
Assess clinical risk and genomic risk
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK Clinical and Genomic BOTH LOW RISK N=3300 55% N=600 10%

22
Assess clinical risk and genomic risk
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK Clinical and Genomic BOTH LOW RISK N=3300 55% N=600 10% Chemotherapy ± 4350 patients No Chemotherapy ± 1650 patients

23
DISCORDANT Clinical and Genomic Risks Clinical and Genomic
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK DISCORDANT Clinical and Genomic Risks Clinical and Genomic BOTH LOW RISK N=2100 35% Chemotherapy ± 4350 patients No Chemotherapy ± 1650 patients

24
DISCORDANT Clinical and Genomic Risks Clinical and Genomic
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK DISCORDANT Clinical and Genomic Risks Clinical and Genomic BOTH LOW RISK Clinical HIGH RISK Genomic LOW RISK N=1680 80% Chemotherapy ± 4350 patients No Chemotherapy ± 1650 patients

25
DISCORDANT Clinical and Genomic Risks Clinical and Genomic
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK DISCORDANT Clinical and Genomic Risks Clinical and Genomic BOTH LOW RISK Clinical HIGH RISK Genomic LOW RISK Genomic HIGH RISK Clinical LOW RISK N=1680 80% N=420 20% Chemotherapy ± 4350 patients No Chemotherapy ± 1650 patients

26
RANDOMIZE decision-making
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK DISCORDANT Clinical and Genomic Risks Clinical and Genomic BOTH LOW RISK Clinical HIGH RISK Genomic LOW RISK Genomic HIGH RISK Clinical LOW RISK RANDOMIZE decision-making Chemotherapy ± 4350 patients No Chemotherapy ± 1650 patients

27
RANDOMIZE decision-making Use clinical risk Use genomic risk
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK DISCORDANT Clinical and Genomic Risks Clinical and Genomic BOTH LOW RISK Clinical HIGH RISK Genomic LOW RISK Genomic HIGH RISK Clinical LOW RISK RANDOMIZE decision-making Use clinical risk Use genomic risk Chemotherapy ± 4350 patients No Chemotherapy ± 1650 patients

28
RANDOMIZE decision-making Use clinical risk Use genomic risk
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK DISCORDANT Clinical and Genomic Risks Clinical and Genomic BOTH LOW RISK Clinical HIGH RISK Genomic LOW RISK Genomic HIGH RISK Clinical LOW RISK RANDOMIZE decision-making Use clinical risk Use genomic risk High risk Low risk N=840 80% Chemotherapy ± 4350 patients N=210 20% No Chemotherapy ± 1650 patients

29
RANDOMIZE decision-making Use clinical risk Use genomic risk
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK DISCORDANT Clinical and Genomic Risks Clinical and Genomic BOTH LOW RISK Clinical HIGH RISK Genomic LOW RISK Genomic HIGH RISK Clinical LOW RISK RANDOMIZE decision-making Use clinical risk Use genomic risk N=840 80% High risk Low risk Chemotherapy ± 4350 patients N=210 20% No Chemotherapy ± 1650 patients

30
RANDOMIZE decision-making Use clinical risk Use genomic risk
MINDACT – 6000 patients Assess clinical risk and genomic risk Clinical and Genomic BOTH HIGH RISK DISCORDANT Clinical and Genomic Risks Clinical and Genomic BOTH LOW RISK N=3300 55% N=600 10% Clinical HIGH RISK Genomic LOW RISK Genomic HIGH RISK Clinical LOW RISK N=1680 80% RANDOMIZE decision-making N=420 20% Use clinical risk Use genomic risk N=840 80% High risk Low risk High risk Low risk Chemotherapy ± 4350 patients N=210 20% No Chemotherapy ± 1650 patients N=840 80% N=210 20%

31
PRIMARY TEST This test has 80% power
Dataset: the patients who have a low risk gene prognosis signature and high risk clinical-pathologic criteria, and who were randomized to receive no chemotherapy. Expected size: 840 Null hypothesis: 5-year DMFS = 92% will be tested. Assuming: 3 years accrual 6 years total duration (3 to 6 years follow up per patient) two-sided test at 95% confidence level true 5-year DMFS = 95% This test has 80% power
 two-sided test at 95% confidence level. true 5-year DMFS = 95% This test has 80% power.")
32
TRANSBIG : STANDARDISATION/ VALIDATION PHASE
Jules Bordet Institute Brussels Karolinska Institute Stockholm Gustave Roussy Institute Paris NKI Radcliffe Hospital Oxford Collection of frozen samples of BC patients with 5 year f-up Node (-) = 400 KEY QUESTIONS TO BE ANSWERED Validation Transferability Reproducibility Are results reproducible across laboratories and platforms? Part of the standardization and validation phase will also ensure that the signature is reproducible in other laboratories with the same technology. This phase will also refine the reproducibility and quality control of the technique developed by Netherlands Cancer Institute (NKI). Additionally, whilst MINDACT will be performed using the NKI Agilent platform on the dedicated “Breast Cancer prognosis” array, parallel studies will be conducted using the Affymetrix platform to find a signature that is applicable in as many laboratories as possible. These phases will be strictly, according to validation protocols outlining the procedures required and the definition of appropriate validation “a priori”. Is the prognostic value of the 70 gene signature confirmed ? Is the 70 gene signature transferable onto the Affymetrix platform?
 = 400. KEY QUESTIONS TO BE ANSWERED. Validation. Transferability. Reproducibility. Are results reproducible across. laboratories. and platforms Part of the standardization and validation phase will also ensure that the signature is reproducible in other laboratories with the same technology. This phase will also refine the reproducibility and quality control of the technique developed by Netherlands Cancer Institute (NKI). Additionally, whilst MINDACT will be performed using the NKI Agilent platform on the dedicated Breast Cancer prognosis array, parallel studies will be conducted using the Affymetrix platform to find a signature that is applicable in as many laboratories as possible. These phases will be strictly, according to validation protocols outlining the procedures required and the definition of appropriate validation a priori . Is the prognostic value of the 70 gene signature confirmed Is the 70 gene signature transferable onto the Affymetrix platform")
33
on behalf of the TRANSBIG CONSORTIUM
SABCS, Dec. 8, 2004 MULTI-CENTER EXTERNAL VALIDATION STUDY OF THE AMSTERDAM 70-GENE PROGNOSTIC SIGNATURE IN NODE NEGATIVE UNTREATED BREAST CANCER INTERIM ANALYSIS MJ Piccart, S Loi, L Van’t Veer, M Saghastchian-d’Assignies, A Glas, P Ellis, A Harris, J Bergh, R Lidereau, D Sgroi, E Rutgers, G Viale, C Sotiriou, M Delorenzi, J Bogaerts, P Therasse, M Amakrane, F Cardoso, M Buyse on behalf of the TRANSBIG CONSORTIUM Partially funded by the European Commission’s Framework VI Programme

34
PATIENT POPULATIONS : GENE SIGNATURE RISKS Original Amsterdam series
Validation series N = 291 Original Amsterdam series N = 151 Low risk (n=109) 37% Low risk (n=60) 40% High risk (n=182) 63% High risk (n=91) 60%
 37% Low risk. (n=60) 40% High risk. (n=182) 63% High risk. (n=91) 60%")
35
CLINICAL RISK CLASSIFICATIONS
Validation series Amsterdam series 1. St Gallen criteria 2. Nottingham Prognostic Index 3. Adjuvant ! Online (P. Ravdin)
")
36
ADJUVANT! ONLINE FOR BREAST CANCER
Threshold for Clinical Low Risk = Predicted 10-year survival probability at least equal to x % with x varying from 60% to 95% If x=90% Low risk: n=45 (15%) High risk: n=246 (85%)
 High risk: n=246 (85%)")
37
Levels of evidence for biomarkers studies
Independent validation study on archive material High powered clinical trial specifically addressing the gene signature’s utility MINDACT Amsterdam gene-expression prognostic signature N=78 Other populations Internal + external quality assurance Level 5 and 4 Level 3 Level 1 Levels of evidence for biomarkers studies MINDACT is expected to begin recruitment in Currently several laboratories are involved in a “standardisation and validation” phase. This is a retrospective genomic analysis using over 300 archival samples from 4 other hospitals and countries. This step is crucial to ensure the Dutch 70-gene signature is reproducible and applicable across different populations in other countries. The “validation and standardization” phase will provide a “go/no go” decision step regarding MINDACT. The ultimate validation however is the prospective, multi-centre randomised clinical trial. E.U. GRANT, 6th Framework Programme

38
@

39
The TRANSBIG consortium is grateful to the European Community for the support it has provided under its Framework Programme VI. The European Community is not responsible for any of the views presented here, nor is it liable for any use that may be made of the information contained herein.

40
GRACIAS

Similar presentations












>")







 1 Concordance of HER2 Central Assessment.>")



