Download presentation
Presentation is loading. Please wait.

1
Prevention of Surgical Site Infections
William A. Rutala, Ph.D., M.P.H. UNC Health Care System and UNC School of Medicine, Chapel Hill, NC

2
Disclosure This educational activity is brought to you, in part, by Advanced Sterilization Products (ASP) and Ethicon. The speaker receives an honorarium from ASP and Ethicon and must present information in compliance with FDA requirements applicable to ASP.
 and Ethicon. The speaker receives an honorarium from ASP and Ethicon and must present information in compliance with FDA requirements applicable to ASP.")
3
TOPICS Epidemiology of healthcare associated infections (HAI)
Review the morbidity, mortality, and economic consequences of HAIs Discuss the risk factors and etiology of SSIs Provide strategies to prevent SSIs National initiatives to prevent SSIs

4
Healthcare-Associated Infections (HAIs)
HAIs are those that develop in the hospital that were neither incubating nor present at the time of admission 40 million persons hospitalized annually in US; 5% or 2M will develop a HAI Morbidity and mortality (90,000 deaths); 6th leading cause of death in the US Variable prolongation of hospital stay $5-10 billion/year
; 6th leading cause of death in the US. Variable prolongation of hospital stay. $5-10 billion/year.")
5
Impact of Healthcare-Associated Infections

6
Cost Estimates for Specific Healthcare-Associated Infections
HAI type Weight-Adjusted Cost per HAI Mean + SE Range of Published Estimates of Cost per HAI VAP 25, ,132 8,682-31,316 BSI 23, ,184 6,908-37,260 SSI 10, ,249 2,527-29,367 CA-UTI 2005 US dollars Anderson DJ, et al. ICHE 2007;28:

7
UNC Hospitals Selected HAIs and Estimated Cost
HAI type UNC Cases, 2006 Estimated Cost, $ VAP 85 2,131,120 BSI 297 6,902,874 SSI 266 2,777,838 CA-UTI 311 235,738 Total 959 12,047,570 Total cost estimated by multiplying number of cases at UNC Hospitals by mean cost derived from Duke meta-analysis

8
Most Prevalent [Animated slide-mouse click once]
The issues of HAI are probably already being dealt with by your organization. I would like to help you get a better grip on the economic benefits of reducing these infections. It’s best to start breaking down the picture of HAIs. According to the Centers for Disease Control, hospital-acquired infections manifest mostly as urinary-tract infections, surgical site infections, and primary bloodstream infections, with the remaining infections falling under other categories. References 1. Weinstein RA. Emerg Infect Dis. 1998;4(3): 2. CDC, NNIS Semiannual Report, Dec 2000. Weinstein RA. Emerg Infect Dis. 1998;4(3): CDC, NNIS Semiannual Report, Dec 2000. 8
![Most Prevalent [Animated slide-mouse click once]](http://slideplayer.com/slide/4383620/14/images/8/Most+Prevalent+%5BAnimated+slide-mouse+click+once%5D.jpg "The issues of HAI are probably already being dealt with by your organization. I would like to help you get a better grip on the economic benefits of reducing these infections. It’s best to start breaking down the picture of HAIs. According to the Centers for Disease Control, hospital-acquired infections manifest mostly as urinary-tract infections, surgical site infections, and primary bloodstream infections, with the remaining infections falling under other categories. References. 1. Weinstein RA. Emerg Infect Dis. 1998;4(3): CDC, NNIS Semiannual Report, Dec Weinstein RA. Emerg Infect Dis. 1998;4(3): CDC, NNIS Semiannual Report, Dec")
9
Surgical Site Infection
[Animated slide—mouse click to bring up pictures] 9

10
Surgical Site Infection
SSIs third most common HAI, accounting for 14-16% of HAIs Among surgical patients, SSIs were most common accounting for ~40% of healthcare-associated infections 67% incisional infections (confined to incision) 33% organ/space infections Increase an average of 7 days to each hospitalization Increase >$10,000 (2005 $) to each hospitalization Appropriate preoperative administration of antibiotics and other prevention measures are effective in preventing infection Postoperative surgical site infection, or SSI, is a major cause of patient injury, mortality, and health care cost:1,2 An estimated 2.6% of nearly 30 million operations are complicated by SSIs each year. SSIs account for about 40% of all nosocomial infections among surgical patients in the United States. Each infection is estimated to increase a hospital stay by an average of 7 days and add over $3,000 in charges (1992 data). Appropriate preoperative administration of antibiotics is effective in preventing infection. References Surgical Site Infections. Institute for Healthcare Improvement. Available at: Accessed on February 1, 2007. Odom-Forren J. Preventing surgical site infections. Nursing ;36(6):58-63. Surgical Site Infections. Available at: Odom-Forren J. Nursing ;36(6):58-63. 10
 33% organ/space infections. Increase an average of 7 days to each hospitalization. Increase >$10,000 (2005 $) to each hospitalization. Appropriate preoperative administration of antibiotics and other prevention measures are effective in preventing infection. Postoperative surgical site infection, or SSI, is a major cause of patient injury, mortality, and health care cost:1,2. An estimated 2.6% of nearly 30 million operations are complicated by SSIs each year. SSIs account for about 40% of all nosocomial infections among surgical patients in the United States. Each infection is estimated to increase a hospital stay by an average of 7 days and add over $3,000 in charges (1992 data). Appropriate preoperative administration of antibiotics is effective in preventing infection. References. Surgical Site Infections. Institute for Healthcare Improvement. Available at: Accessed on February 1, Odom-Forren J. Preventing surgical site infections. Nursing ;36(6): Surgical Site Infections. Available at: Odom-Forren J. Nursing ;36(6):")
11
Surgical Site Infection
Advances in infection control practices Improved operating room ventilation Sterilization methods Barriers Surgical technique Antimicrobial prophylaxis

12
I use this slide to describe the factors associated for antimicrobial use in the hospital (immunosuppression, acuity of illness, devices, hospital staff, etc) and that we as clinicians tend to prescribe for the individual patient and lose sight of our influence on the ecology of the microbes of the community
 and that we as clinicians tend to prescribe for the individual patient and lose sight of our influence on the ecology of the microbes of the community")
13
Challenges in the Prevention and Management of Surgical Site Infections
Changing population of hospital patients Increased severity of illness Increased numbers of surgical patients who are elderly Increased numbers of chronic, debilitating or immunocompromising underlying diseases Shorter duration of hospitalization Increased numbers of prosthetic implant and organ transplant operations performed Public reporting of infection rates/proportions Growing frequency of antimicrobial-resistant pathogens Non-reimbursement for “medical errors”-CMS Lack of compliance with hand hygiene

14
Clinical and Economic Impact
Procedure/Device Devices/yr* Infections/yr Avg. cost Mortality* CARDIO Heart valves 85,000 3,400 $50,000 High Vascular grafts 450,000 16,000 $40,000 Moderate Pacemaker/ICD 300,000 12,000 $35,000 LV assist dev. 700 280 NEURO CNS shunt 40,000 2400 The next two slides present numbers of devices implanted by therapeutic area, as well as estimated infections per year, costs, and mortality. Substantial morbidity, mortality, and costs are associated with infections that occur when microbial colonization is not prevented or adequately treated. Average costs include the estimated cost of combined medical and surgical treatment associated with infections. References 1. Darouiche RO. Treatment of infections associated with surgical implants N Engl J Med Apr 1;350(14): 2. Darouiche RO. Device-associated infections: a macroproblem that starts with microadherence. Clin Infect Dis. 2001;33(9): Adapted from: Darouiche RO. N Engl J Med. 2004;350: *Darouiche RO. Clin Infec Dis. 2001;38: 14
: Darouiche RO. Device-associated infections: a macroproblem that starts with microadherence. Clin Infect Dis. 2001;33(9): Adapted from: Darouiche RO. N Engl J Med. 2004;350: *Darouiche RO. Clin Infec Dis. 2001;38:")
15
Clinical and Economic Impact
Procedure/Device Devices/yr* Infections/yr Avg. cost Mortality* ORTHOPEDIC Joint prosthesis 600,000 12,000 $30,000 Low Fracture fixator 2,000,000 100,000 $15,000 PLASTIC Breast implant 130,000 2600 $20,000 UROLOGICAL Penile implant 15,000 450 $35,000 Per Dr. Rabih Darouiche on 4/22/07, the number of breast and penile implants are on the increase due to the introduction of Viagra® and Cialis®. Adapted from: Darouiche RO. N Engl J Med. 2004;350: *Darouiche RO. Clin Infec Dis. 2001;38: 15

16
SSI: Pathogenesis Risk of surgical site infections =
Dose of bacterial contamination x virulence (toxins) Resistance of the host
 Resistance of the host.")
17
SSI: Primary Risk Factors
Endogenous microorganisms Skin-dwelling microorganisms Most common source S aureus most common isolate Fecal flora (gnr) when incisions are near the perineum or groin Exogenous microorganisms Surgical personnel (members of surgical team) OR environment (including air) All tools, instruments, and materials Most surgical site infections (SSIs) are caused by skin-dwelling microorganisms from the patient. Staphylococcus aureus is the most common isolate associated with the development of surgical site infections. Exogenous sources of pathogens that contribute to surgical site infection include surgical personnel, particularly surgical team members, who carry microorganisms on their person. The operating room environment, including the air itself, may be contaminated with microorganism that are transferred to the patient. All tools, instruments, and materials brought into the sterile field may harbor pathogens if they are not adequately sterilized. Reference Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 17
 when incisions are near the perineum or groin. Exogenous microorganisms. Surgical personnel (members of surgical team) OR environment (including air) All tools, instruments, and materials. Most surgical site infections (SSIs) are caused by skin-dwelling microorganisms from the patient. Staphylococcus aureus is the most common isolate associated with the development of surgical site infections. Exogenous sources of pathogens that contribute to surgical site infection include surgical personnel, particularly surgical team members, who carry microorganisms on their person. The operating room environment, including the air itself, may be contaminated with microorganism that are transferred to the patient. All tools, instruments, and materials brought into the sterile field may harbor pathogens if they are not adequately sterilized. Reference. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4):")
18
SSI: Microbiology (NNIS, 1996)
")
19
PATHOGENS ASSOCIATED WITH SSIs: NHSN, 2006-2007
Hidron AI, et al. ICHE 2008;29:

21
To Reduce the Risk of Surgical Site Infection
A simple but realistic approach must be applied with the awareness that the risk of SSIs is influenced by characteristics of the patient, operation, personnel and hospital Postoperative surgical site infection, or SSI, is a major cause of patient injury, mortality, and health care cost:1,2 An estimated 2.6% of nearly 30 million operations are complicated by SSIs each year. SSIs account for about 40% of all nosocomial infections among surgical patients in the United States. Each infection is estimated to increase a hospital stay by an average of 7 days and add over $3,000 in charges (1992 data). Appropriate preoperative administration of antibiotics is effective in preventing infection. References Surgical Site Infections. Institute for Healthcare Improvement. Available at: Accessed on February 1, 2007. Odom-Forren J. Preventing surgical site infections. Nursing ;36(6):58-63. Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 21
. Appropriate preoperative administration of antibiotics is effective in preventing infection. References. Surgical Site Infections. Institute for Healthcare Improvement. Available at: Accessed on February 1, Odom-Forren J. Preventing surgical site infections. Nursing ;36(6): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4):")
22
CDC: SSI Recommendations, 1999
Definitions IA: Strongly recommended for all hospitals and strongly supported by experimental or epidemiologic studies IB: Strongly recommended for all hospitals and viewed as effective by experts II: Suggested for implementation in many hospitals; suggestive clinical or epidemiologic studies, strong theoretical rationale

23
SSI: CDC Guidelines Patient characteristics Preoperative issues
Intra-operative issues Postoperative issues [[animated slide—mouse click for each text box]] The Guidelines for Prevention of Surgical Site Infection developed by the Hospital Infection Control Practices Advisory Committee of the CDC underscores the risk to patients of morbidity and mortality associated with surgical site infections (SSI). Risks associated with SSIs fall into the following categories: Patient characteristics Operative characteristics, including preoperative, intraoperative, and postoperative factors Primary modifiable risks are described in the next slides. Reference Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 23
. Risks associated with SSIs fall into the following categories: Patient characteristics. Operative characteristics, including preoperative, intraoperative, and postoperative factors. Primary modifiable risks are described in the next slides. Reference. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4):")
24
SSI: CDC Guidelines Patient characteristics/risk factor
Preoperative issues Intra-operative issues Postoperative issues [[animated slide—mouse click for each text box]] The Guidelines for Prevention of Surgical Site Infection developed by the Hospital Infection Control Practices Advisory Committee of the CDC underscores the risk to patients of morbidity and mortality associated with surgical site infections (SSI). Risks associated with SSIs fall into the following categories: Patient characteristics Operative characteristics, including preoperative, intraoperative, and postoperative factors Primary modifiable risks are described in the next slides. Reference Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 24
. Risks associated with SSIs fall into the following categories: Patient characteristics. Operative characteristics, including preoperative, intraoperative, and postoperative factors. Primary modifiable risks are described in the next slides. Reference. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4):")
25
Risk and Prevention in SSIs
Risk Factor-a variable that has a significant independent association with the development of SSI after a specific operation Postoperative surgical site infection, or SSI, is a major cause of patient injury, mortality, and health care cost:1,2 An estimated 2.6% of nearly 30 million operations are complicated by SSIs each year. SSIs account for about 40% of all nosocomial infections among surgical patients in the United States. Each infection is estimated to increase a hospital stay by an average of 7 days and add over $3,000 in charges (1992 data). Appropriate preoperative administration of antibiotics is effective in preventing infection. References Surgical Site Infections. Institute for Healthcare Improvement. Available at: Accessed on February 1, 2007. Odom-Forren J. Preventing surgical site infections. Nursing ;36(6):58-63. 25
. Appropriate preoperative administration of antibiotics is effective in preventing infection. References. Surgical Site Infections. Institute for Healthcare Improvement. Available at: Accessed on February 1, Odom-Forren J. Preventing surgical site infections. Nursing ;36(6):")
26
SSI: Intrinsic/Patient Risk Factors
Age-extremes Nutritional status-poor Diabetes-controversial; increased glucose levels in post-op period ↑ risk Smoking-nicotine delays wound healing ↑ risk Obesity>20% ideal body weight Remote infections ↑ risk Endogenous mucosal microorganisms Preoperative nares S. aureus- CT patients Immunosuppressive drugs may ↑ risk Preoperative stay-surrogate for severity of illness

27
Prevention of SSIs Preoperative preparation of the patient
Minimize preoperative stay (II) Identify and treat remote site infections (IA) Adequately control glucose in diabetics (IB) Encourage discontinuation of tobacco for 30d (IB). Consider delaying elective procedures in severely malnourished patients (II) No recommendations to taper or discontinue steroids (Unresolved issue)
 Identify and treat remote site infections (IA) Adequately control glucose in diabetics (IB) Encourage discontinuation of tobacco for 30d (IB). Consider delaying elective procedures in severely malnourished patients (II) No recommendations to taper or discontinue steroids (Unresolved issue)")
29
SSI: CDC Guidelines Patient characteristics Preoperative issues
Intra-operative issues Postoperative issues [[animated slide—mouse click for each text box]] The Guidelines for Prevention of Surgical Site Infection developed by the Hospital Infection Control Practices Advisory Committee of the CDC underscores the risk to patients of morbidity and mortality associated with surgical site infections (SSI). Risks associated with SSIs fall into the following categories: Patient characteristics Operative characteristics, including preoperative, intraoperative, and postoperative factors Primary modifiable risks are described in the next slides. Reference Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 29
. Risks associated with SSIs fall into the following categories: Patient characteristics. Operative characteristics, including preoperative, intraoperative, and postoperative factors. Primary modifiable risks are described in the next slides. Reference. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4):")
30
SSI: Preoperative Issues Modifiable Risks
Glucose control-in diabetic patients Preoperative CHG shower Appropriate hair removal Hand hygiene Skin antisepsis [[animated slide—mouse click for each text box]] The Guidelines for Prevention of Surgical Site Infection developed by the Hospital Infection Control Practices Advisory Committee of the CDC underscores the risk to patients of morbidity and mortality associated with surgical site infections (SSI). Specific guidelines for prevention of SSIs include:1,2 Ensuring glucose control in diabetic patients Having the patient shower with an antiseptic prior to surgery. Chlorhexidine is associated with a nine-fold decrease in bacterial colony counts, compared to less than two-fold decrease using povidone-iodine. Leaving hair intact. Shaving causes microabrasions that may provide access for microorganisms. The risk of SSI is lower with clipping hair or the use of depilatories, but each produces greater risk of infection than keeping hair intact. Proper hand and forearm antisepsis by the surgical team and exclusion of members who may be ill or infected to prevent exogenous contamination Preoperative skin antisepsis Prophylactic treatment with an antimicrobial initiated immediately prior to surgery to reduce microbial burden Ensuring normal body temperature; intraoperative hypothermia has been associated with higher SSI risk References Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): 5 Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, 2007. Antimicrobial prophylaxis Normothermia-hypo higher risks Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 5 Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, 2007. 30
. Specific guidelines for prevention of SSIs include:1,2. Ensuring glucose control in diabetic patients. Having the patient shower with an antiseptic prior to surgery. Chlorhexidine is associated with a nine-fold decrease in bacterial colony counts, compared to less than two-fold decrease using povidone-iodine. Leaving hair intact. Shaving causes microabrasions that may provide access for microorganisms. The risk of SSI is lower with clipping hair or the use of depilatories, but each produces greater risk of infection than keeping hair intact. Proper hand and forearm antisepsis by the surgical team and exclusion of members who may be ill or infected to prevent exogenous contamination. Preoperative skin antisepsis. Prophylactic treatment with an antimicrobial initiated immediately prior to surgery to reduce microbial burden. Ensuring normal body temperature; intraoperative hypothermia has been associated with higher SSI risk. References. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, Antimicrobial prophylaxis. Normothermia-hypo higher risks. Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8,")
31
Prevention of SSIs Preoperative preparation of the patient
Preoperative showers with antiseptic agent at least the night before (IB) Do not remove hair preoperatively unless it will interfere with the operation (IA) If hair removed, remove just prior to surgery with electric clippers (IA) Wash and clean at and around incision site prior to performing antiseptic skin preparation (IB)
 Do not remove hair preoperatively unless it will interfere with the operation (IA) If hair removed, remove just prior to surgery with electric clippers (IA) Wash and clean at and around incision site prior to performing antiseptic skin preparation (IB)")
32
Preoperative Showers Cruse and Foord (Arch Surg 1973;107:206)
Garibaldi R (J Hosp Infect 1988;11(suppl B):5 Reduction in bacterial counts: Chlorhexidine 9-fold, povidone-iodine 1.3-fold Cruse and Foord (Arch Surg 1973;107:206) Clean surgery SSI rate, no shower = 2.3% SSI rate, shower with soap = 2.1% SSI rate, shower with hexachlorophene = 1.3%
:5. Reduction in bacterial counts: Chlorhexidine 9-fold, povidone-iodine 1.3-fold. Cruse and Foord (Arch Surg 1973;107:206) Clean surgery. SSI rate, no shower = 2.3% SSI rate, shower with soap = 2.1% SSI rate, shower with hexachlorophene = 1.3%")
33
Chlorhexidine: Preoperative Showers
CDC recommends preoperative showering with antiseptic1 CHG more effective than PI and triclocarban Lower rates of intraoperative wound contamination The surgical site infection guidelines published by the Centers for Disease Control and Prevention recommend preoperative showering with chlorhexidine to reduce microbial colony counts on skin.1 Studies demonstrate that chlorhexidine gluconate is more effective than povidone-iodine or triclocarban medicated soap and was associated with lower rates of intraoperative wound contamination.2 References Mangram AJ, et al. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Garibaldi RA. Prevention of intraoperative wound contamination with chlorhexidine shower and scrub. J Hosp Infect. 1988;11(suppl B):5-9. 1. Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20(4): 2. Garibaldi RA. J Hosp Infect. 1988;11(suppl B):5-9. 33
: Garibaldi RA. Prevention of intraoperative wound contamination with chlorhexidine shower and scrub. J Hosp Infect. 1988;11(suppl B): Mangram AJ et al. Infect Control Hosp Epidemiol. 1999;20(4): Garibaldi RA. J Hosp Infect. 1988;11(suppl B):")
34
Chlorhexidine: Preoperative Showers
Patients who had 2 preoperative showers with CHG 24 hours before surgery had reduced rates of wound infection compared to patients who showered with soap. The effect of preoperative whole-body washing with chlorhexidine detergent on the incidence of postoperative wound infection was assessed in a placebo-controlled trial of 1989 patients. Patients bathed or showered with chlorhexidine, placebo, or conventional bar soap twice during the 24-hour period before surgery. The overall infection rate for patients treated with chlorhexidine was 9%, compared to 12.8% among patient who used bar soap and 11.7% among placebo patients. Reference Hayek LJ, Emerson JM, Gardner AM. A placebo-controlled trial of the effect of two preoperative baths or showers with chlorhexidine detergent on postoperative wound infection rates. J Hosp Infect. 1987;10(2): Hayek LJ, et al. J Hosp Infect. 1987;10(2): 34
: Hayek LJ, et al. J Hosp Infect. 1987;10(2):")
35
4% Chlorhexidine Gluconate (CHG) Shower -
Mean Skin Surface Concentration (N=60) CHG Shower Group 1A “Evening (PM)” Group 2A “Morning (AM)” CHG Concentration (PPM) Group 3A “Both (AM and PM)” p <0.05 NS P<0.001 MIC90 = 4.8 ppm Left Elbow Right Elbow Abdominal Left Knee Right Knee Skin Sites Edmiston et al, J Am Coll Surg 2008;207:
 CHG Shower. Group 1A Evening (PM) Group 2A Morning (AM) CHG Concentration (PPM) Group 3A. Both (AM and PM) p <0.05. NS. P< MIC90 = 4.8 ppm. Left Elbow. Right Elbow. Abdominal. Left Knee. Right Knee. Skin Sites. Edmiston et al, J Am Coll Surg 2008;207:")
36
Preoperative Hair Removal
Seropian and Reynolds (Am J Surg 1971;121:251) SSI rate, razor-shave (microabrasions) = 5.6% SSI rate, razor-shave >24 hours = 20% SSI rate, razor-shave within 24 hours = 7.1% SSI, razor-shave immediately preop = 3.1% SSI rate, no removal or depilatory = 0.6%
 SSI rate, razor-shave (microabrasions) = 5.6% SSI rate, razor-shave >24 hours = 20% SSI rate, razor-shave within 24 hours = 7.1% SSI, razor-shave immediately preop = 3.1% SSI rate, no removal or depilatory = 0.6%")
37
Preoperative Hair Removal
Cruse and Foord (Arch Surg 1973;107:206) SSI rate, razor-shave = 2.5% Manual hair clipped = 1.7% Electric hair clipper = 1.4% No shave or clip = 0.9%
 SSI rate, razor-shave = 2.5% Manual hair clipped = 1.7% Electric hair clipper = 1.4% No shave or clip = 0.9%")
38
SSI: Preoperative Issues Modifiable Risks
Glucose control-in diabetic patients Preoperative CHG shower Appropriate hair removal Hand hygiene Skin antisepsis [[animated slide—mouse click for each text box]] The Guidelines for Prevention of Surgical Site Infection developed by the Hospital Infection Control Practices Advisory Committee of the CDC underscores the risk to patients of morbidity and mortality associated with surgical site infections (SSI). Specific guidelines for prevention of SSIs include:1,2 Ensuring glucose control in diabetic patients Having the patient shower with an antiseptic prior to surgery. Chlorhexidine is associated with a nine-fold decrease in bacterial colony counts, compared to less than two-fold decrease using povidone-iodine. Leaving hair intact. Shaving causes microabrasions that may provide access for microorganisms. The risk of SSI is lower with clipping hair or the use of depilatories, but each produces greater risk of infection than keeping hair intact. Proper hand and forearm antisepsis by the surgical team and exclusion of members who may be ill or infected to prevent exogenous contamination Preoperative skin antisepsis Prophylactic treatment with an antimicrobial initiated immediately prior to surgery to reduce microbial burden Ensuring normal body temperature; intraoperative hypothermia has been associated with higher SSI risk References Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): 5 Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, 2007. Antimicrobial prophylaxis Normothermia-hypo higher risks Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 5 Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, 2007. 38
. Specific guidelines for prevention of SSIs include:1,2. Ensuring glucose control in diabetic patients. Having the patient shower with an antiseptic prior to surgery. Chlorhexidine is associated with a nine-fold decrease in bacterial colony counts, compared to less than two-fold decrease using povidone-iodine. Leaving hair intact. Shaving causes microabrasions that may provide access for microorganisms. The risk of SSI is lower with clipping hair or the use of depilatories, but each produces greater risk of infection than keeping hair intact. Proper hand and forearm antisepsis by the surgical team and exclusion of members who may be ill or infected to prevent exogenous contamination. Preoperative skin antisepsis. Prophylactic treatment with an antimicrobial initiated immediately prior to surgery to reduce microbial burden. Ensuring normal body temperature; intraoperative hypothermia has been associated with higher SSI risk. References. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8, Antimicrobial prophylaxis. Normothermia-hypo higher risks. Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): Million lives. Institute for Healthcare Improvement. Available at: Accessed on February 8,")
39
Prevention of SSIs Preoperative preparation of the surgical team
Keep nails short and no artificial nails (IB) Perform preoperative surgical scrub for 2-5 minutes with antiseptic-alcohol, chlorhexidine, iodophors (IB); new waterless, surgical hand antisepsis with alcohol Perform preoperative scrub including forearms (IB) Do not wear hand/arm jewelry (II) Prohibiting nail polish (No recommendation)
 Perform preoperative surgical scrub for 2-5 minutes with antiseptic-alcohol, chlorhexidine, iodophors (IB); new waterless, surgical hand antisepsis with alcohol. Perform preoperative scrub including forearms (IB) Do not wear hand/arm jewelry (II) Prohibiting nail polish (No recommendation)")
40
Importance of Our Skin Largest organ of the body Epidermis Dermis
Subcutaneous tissue (hypodermis) The skin is the largest organ of the body, measuring about 2 square meters in adults, consisting of the epidermis and dermis. The epidermis is divided into the following sublayers or strata: Stratum corneum Stratum lucidum, a layer of irregular transparent epidermal cells with traces of nuclei interposed between the stratum corneum and stratum germinativum in the thick skin of the palms and soles (not shown) Stratum granulosum Stratum spinosum Stratum germinativum, also called "stratum basale" The dermis is a connective tissue layer located beneath the epidermis that contains nerve endings, sweat and sebaceous glands, and blood and lymph vessels. Reference Todar K. The Bacterial Flora of Humans. Todar's Online Textbook of Bacteriology Available at: Accessed on February 5, 2007. 40
 The skin is the largest organ of the body, measuring about 2 square meters in adults, consisting of the epidermis and dermis. The epidermis is divided into the following sublayers or strata: Stratum corneum. Stratum lucidum, a layer of irregular transparent epidermal cells with traces of nuclei interposed between the stratum corneum and stratum germinativum in the thick skin of the palms and soles (not shown) Stratum granulosum. Stratum spinosum. Stratum germinativum, also called stratum basale The dermis is a connective tissue layer located beneath the epidermis that contains nerve endings, sweat and sebaceous glands, and blood and lymph vessels. Reference. Todar K. The Bacterial Flora of Humans. Todar s Online Textbook of Bacteriology Available at: Accessed on February 5,")
41
Importance of Our Skin #1 Function: Protective Barrier Microorganisms
80% in first 5 cell layers of epidermis When skin is perforated Integrity is compromised infection risk Skin provides many types of protection, but it’s primary function is to serve as a barrier. The skin’s protective barrier function keep moisture in and microorganisms out. When skin is perforated or incised, its barrier function is compromised. Microorganisms that migrate through a skin perforation substantially increase the risk of infection. 41

42
Normal Skin Micro-Flora
Numbers of bacteria that colonize different parts of the body Numbers per square centimeter of skin surface (cfu/cm2). Counts on hands range from 3.9x104 to 4.6x106. 42
. Counts on hands range from 3.9x104 to 4.6x")
43
Surgical Hand Antisepsis

44
Alcohols Advantages Disadvantages Broad spectrum Effective against:
Most gram-positive Most gram-negative Fungi Viruses Rapid acting Short persistence Potentially drying to skin Potentially flammable Spores may be resistant Not applicable for mucosal membranes Isopropyl and ethyl alcohols are most commonly used for skin antisepsis. Alcohol’s advantages for skin antisepsis include broad-spectrum activity against most gram-positive and gram-negative microorganisms and good activity against many fungi and viruses, rapid activity, and safety.1-3 References Larson EL. APIC guideline for handwashing and hand antisepsis in health care settings. Am J Infect Control. 1995;23(4): Boyce JM, Pittet D; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Crosby CT, Mares AK. Skin antisepsis: past, present, and future. JVAD. 2001;1-6. Larson EL.. Am J Infect Control. 1995;23(4): Boyce JM, et al. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Crosby CT, Mares AK. JVAD. 2001:1-6. 44
: Boyce JM, Pittet D; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Crosby CT, Mares AK. Skin antisepsis: past, present, and future. JVAD. 2001;1-6. Larson EL.. Am J Infect Control. 1995;23(4): Boyce JM, et al. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Crosby CT, Mares AK. JVAD. 2001:")
45
Iodine/Iodophors Advantages Disadvantages Broad spectrum
Effective against Most gram-positive Most gram-negative Fungi Viruses Some activity against spores Diminished efficacy by organic material (e.g., blood) Variable persistence Irritates skin Iodine and iodophors have a broad spectrum of activity. They are effective against most gram-positive and gram-negative microorganisms, fungi, and viruses and have some activity against spores.1-3 The disadvantages of iodophors are that they are rapidly neutralized in the presence of organic material such as blood, their persistence varies, and they irritate skin.1,3 References Larson EL. APIC guideline for handwashing and hand antisepsis in health care settings. Am J Infect Control. 1995;23(4): Boyce JM, Pittet D; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Crosby CT, Mares AK. Skin antisepsis: past, present, and future. JVAD. 2001:1-6. Larson EL.. Am J Infect Control. 1995;23(4): Boyce JM, et al. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Crosby CT, Mares AK.. JVAD. 2001:1-6. 45
 Variable persistence. Irritates skin. Iodine and iodophors have a broad spectrum of activity. They are effective against most gram-positive and gram-negative microorganisms, fungi, and viruses and have some activity against spores.1-3. The disadvantages of iodophors are that they are rapidly neutralized in the presence of organic material such as blood, their persistence varies, and they irritate skin.1,3. References. Larson EL. APIC guideline for handwashing and hand antisepsis in health care settings. Am J Infect Control. 1995;23(4): Boyce JM, Pittet D; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Crosby CT, Mares AK. Skin antisepsis: past, present, and future. JVAD. 2001:1-6. Larson EL.. Am J Infect Control. 1995;23(4): Boyce JM, et al. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Crosby CT, Mares AK.. JVAD. 2001:")
46
Chlorhexidine Advantages Disadvantages Broad spectrum
Effective against Most gram-positive Most gram-negative Fungi Viruses Yeast Highly persistent Effective in the presence of organic material (e.g., blood) Minimally absorbed Direct instillation can damage ears or eyes Direct contact with nerve tissue can be damaging Minimal activity against spores Chlorhexidine provides several advantages. It has broad-spectrum activity against most gram-positive and gram-negative microorganisms, fungi, yeast, and viruses; it is highly persistent; it is effective in the presence of organic material; and it’s minimally absorbed.1-4 Disadvantages of chlorhexidine are that concentrations of 1% or higher can damage ear or eye tissue when directly instilled. Additionally, there is minimal activity against spores.5,6 References Larson EL. APIC guideline for handwashing and hand antisepsis in health care settings. Am J Infect Control. 1995;23(4): Hidalgo E, Dominguez C. Mechanisms underlying chlorhexidine-induced cytotoxicity. Toxicol In Vitro. 2001;15(4-5): Maki DG, Ringer M, Alvarado CJ. Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet. 1991;338(8763): Larson E, Bobo L, Bennett R et al. Lack of care giver hand contamination with endemic bacterial pathogens in a nursing home. Am J Infect Control Feb;20(1):11-5. Boyce JM, Pittet D; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Anders N, Wollensak J. Inadvertent use of chlorhexidine instead of balanced salt solution for intraocular irrigation. J Cataract Refract Surg. 1997;23(6): Perez R, Freeman S, Sohmer H, Sichel JY. Vestibular and cochlear ototoxicity of topical antiseptics assessed by evoked potentials. Laryngoscope. 2000;110(9): Larson EL. Am J Infect Control. 1995;23(4): Hidalgo E, Dominguez C. Toxicol In Vitro. 2001;15(4-5): Maki DG, et al. Lancet. 1991;338: Larson E, Bobo L.. J Emerg Med. 1992;10(1):7-11. Boyce JM, et al. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Anders N, Wollensak J. J Cataract Refract Surg. 1997;23(6): Perez R, et al. Laryngoscope. 2000;110(9): 46
 Minimally absorbed. Direct instillation can damage ears or eyes. Direct contact with nerve tissue can be damaging. Minimal activity against spores. Chlorhexidine provides several advantages. It has broad-spectrum activity against most gram-positive and gram-negative microorganisms, fungi, yeast, and viruses; it is highly persistent; it is effective in the presence of organic material; and it’s minimally absorbed.1-4. Disadvantages of chlorhexidine are that concentrations of 1% or higher can damage ear or eye tissue when directly instilled. Additionally, there is minimal activity against spores.5,6. References. Larson EL. APIC guideline for handwashing and hand antisepsis in health care settings. Am J Infect Control. 1995;23(4): Hidalgo E, Dominguez C. Mechanisms underlying chlorhexidine-induced cytotoxicity. Toxicol In Vitro. 2001;15(4-5): Maki DG, Ringer M, Alvarado CJ. Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet. 1991;338(8763): Larson E, Bobo L, Bennett R et al. Lack of care giver hand contamination with endemic bacterial pathogens in a nursing home. Am J Infect Control Feb;20(1):11-5. Boyce JM, Pittet D; Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Anders N, Wollensak J. Inadvertent use of chlorhexidine instead of balanced salt solution for intraocular irrigation. J Cataract Refract Surg. 1997;23(6): Perez R, Freeman S, Sohmer H, Sichel JY. Vestibular and cochlear ototoxicity of topical antiseptics assessed by evoked potentials. Laryngoscope. 2000;110(9): Larson EL. Am J Infect Control. 1995;23(4): Hidalgo E, Dominguez C. Toxicol In Vitro. 2001;15(4-5): Maki DG, et al. Lancet. 1991;338: Larson E, Bobo L.. J Emerg Med. 1992;10(1):7-11. Boyce JM, et al. MMWR Recomm Rep Oct 25;51(RR-16):1-45. Anders N, Wollensak J. J Cataract Refract Surg. 1997;23(6): Perez R, et al. Laryngoscope. 2000;110(9):")
47
Surgical Hand Antisepsis
Surgical hand scrubs should: Significantly reduce microorganisms on intact skin Contain a non-irritating antimicrobial preparation Have broad-spectrum activity Be fast-acting and persistent

48
Traditional Iodophors
Combined Agents Active Agents Tincture of Iodine Traditional Iodophors CHG/ Alcohol Broad Spectrum X Rapid Activity Residual Activity Activity in Blood/Organic Non-Irritating Minimal Absorption The combination of chlorhexidine gluconate and alcohol meets all of the criteria for an ideal antiseptic solution. 48

49
Surgical Hand Antisepsis
Formulations containing 60-90% alcohol alone, or 50-95% when combined with small amounts of a QUAT, or CHG lower bacterial counts on skin post-scrub more effectively than other agents Next most active agents (in order of decreasing activity) are CHG, iodophors, triclosan, and plain soap Alcohol-based preparations containing 0.5-1% CHG have persistent activity but alcohol alone may not
 are CHG, iodophors, triclosan, and plain soap. Alcohol-based preparations containing 0.5-1% CHG have persistent activity but alcohol alone may not.")
51
Surgical Hand Antisepsis
Studies suggest that neither a brush nor a sponge is necessary to reduce bacterial counts on the hands of surgical personnel to acceptable levels, especially when alcohol-based products are used One study (AORN J 2001;73:412) found a brushless application of a preparation of 1% CHG plus 61% ethanol yielded lower bacterial counts on the hands of participants than using a sponge/brush to apply 4% CHG
 found a brushless application of a preparation of 1% CHG plus 61% ethanol yielded lower bacterial counts on the hands of participants than using a sponge/brush to apply 4% CHG.")
56
Prevention of SSI Preoperative preparation of the patient
Use appropriate antiseptic for skin preparation (IB) Alcohol (70-92%) Chlorhexidine 4%, 2% or 0.5% in alcohol base Iodine/iodophors Apply in concentric circles moving to periphery Prep area to include incision and any drain sites
 Alcohol (70-92%) Chlorhexidine 4%, 2% or 0.5% in alcohol base. Iodine/iodophors. Apply in concentric circles moving to periphery. Prep area to include incision and any drain sites.")
57
Chlorhexidine Highly effective in studies of
hand washing preoperative showering IV catheter care CHG has a broad spectrum of activity Rapid Persistent Active w/ organic material Non-irritating Recommended in 15 evidence-based guidelines (hand hygiene, catheter-related bloodstream infection) ChloraPrep is a combination of 2% chlorhexidine gluconate and 70% isopropyl alcohol. It has rapid activity against both gram-positive and gram-negative bacteria and is persistent. ChloraPrep remains active in the presence of organic material, including blood, serum, and other protein-rich biomaterials.1,2 Currently, chlorhexidine is recommended in 15 evidence-based guidelines, as shown on the next slide. References Larson EL. APIC guideline for handwashing and hand antisepsis in health care settings. Am J Infect Control. 1995;23(4): Maki DG, Ringer M, Alvarado CJ. Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet. 1991;338(8763): Larson E.. Am J Infect Control. 1995;23(4): Maki DG, et al. Lancet. 1991;338: 57
 ChloraPrep is a combination of 2% chlorhexidine gluconate and 70% isopropyl alcohol. It has rapid activity against both gram-positive and gram-negative bacteria and is persistent. ChloraPrep remains active in the presence of organic material, including blood, serum, and other protein-rich biomaterials.1,2 Currently, chlorhexidine is recommended in 15 evidence-based guidelines, as shown on the next slide. References. Larson EL. APIC guideline for handwashing and hand antisepsis in health care settings. Am J Infect Control. 1995;23(4): Maki DG, Ringer M, Alvarado CJ. Prospective randomised trial of povidone-iodine, alcohol, and chlorhexidine for prevention of infection associated with central venous and arterial catheters. Lancet. 1991;338(8763): Larson E.. Am J Infect Control. 1995;23(4): Maki DG, et al. Lancet. 1991;338:")
58
2% CHG/70% IPA vs. 10% PVP-I Randomized, parallel group, open label, healthy human volunteers 55 subjects Microbial samples: right and left abdominal and inguinal sites Efficacy defined as ≥2.0 log10 reduction from baseline CFUs/cm2 on abdominal sites ≥3.0 log10 mean reduction from baseline CFUs/cm2 on inguinal sites The efficacy of 2% CHG/70% IPA (ChloraPrep) for preoperative skin preparation has been evaluated in several studies. A randomized, parallel-group, open label, Phase III clinical trial was conducted to compare the efficacy of ChloraPrep to 10% povidone-iodine (Betadine) for skin antisepsis. A total of 55 healthy subjects between the ages of 18 and 70 years were included in the study. Microbial samples were taken from right and left abdominal and inguinal sites to establish baseline measurements. Eligible subjects were randomized to treatment with either ChloraPrep or Betadine. Microbial counts were taken using cylinder sampling techniques at 10 minutes, 24 hours, and 48 hours after application of antiseptic. Efficacy was defined as 2.0 log10 mean reduction from baseline CFUs/cm2 on abdominal sites and 3.0 log10 mean reduction from baseline CFUs/cm2 on inguinal sites. Reference Hibbard JS. Analyses comparing the antimicrobial activity and safety of current antiseptic agents: a review. J Infus Nurs. 2005;28(3): Hibbard JS. J Infus Nursing. 2005;28(3): 58
 for preoperative skin preparation has been evaluated in several studies. A randomized, parallel-group, open label, Phase III clinical trial was conducted to compare the efficacy of ChloraPrep to 10% povidone-iodine (Betadine) for skin antisepsis. A total of 55 healthy subjects between the ages of 18 and 70 years were included in the study. Microbial samples were taken from right and left abdominal and inguinal sites to establish baseline measurements. Eligible subjects were randomized to treatment with either ChloraPrep or Betadine. Microbial counts were taken using cylinder sampling techniques at 10 minutes, 24 hours, and 48 hours after application of antiseptic. Efficacy was defined as 2.0 log10 mean reduction from baseline CFUs/cm2 on abdominal sites and 3.0 log10 mean reduction from baseline CFUs/cm2 on inguinal sites. Reference. Hibbard JS. Analyses comparing the antimicrobial activity and safety of current antiseptic agents: a review. J Infus Nurs. 2005;28(3): Hibbard JS. J Infus Nursing. 2005;28(3):")
59
2% CHG/70% IPA vs. 10% PVP-I Abdominal Inguinal
Baseline microbial counts were similar for the two treatment groups. Mean reductions from baseline in CFUs/cm2 for abdominal sites are presented on the left and for inguinal sites on the right. ChloraPrep reduced microbial counts better than Betadine for abdominal and inguinal sites across all measurement periods and demonstrated superior results for persistent activity (48 hours) at abdominal sites and for immediate and persistent activity (10 minutes and 24 hours) for inguinal sites. These results were statistically significantly better than Betadine. No adverse events were reported. Reference Hibbard JS. Analyses comparing the antimicrobial activity and safety of current antiseptic agents: a review. J Infus Nurs. 2005;28(3): Abdominal Inguinal P= compared to baseline for all results Hibbard JS. J Infus Nursing. 2005;28(3): 59
 at abdominal sites and for immediate and persistent activity (10 minutes and 24 hours) for inguinal sites. These results were statistically significantly better than Betadine. No adverse events were reported. Reference. Hibbard JS. Analyses comparing the antimicrobial activity and safety of current antiseptic agents: a review. J Infus Nurs. 2005;28(3): Abdominal. Inguinal. P= compared to baseline for all results. Hibbard JS. J Infus Nursing. 2005;28(3):")
60
2% CHG/70% IPA for Foot and Ankle Surgery
Prospective, randomized trial 125 evaluable patients 40 subjects/group 5 pre-prep baseline Products ChloraPrep® (2% CHG/70% IPA) DuraPrep® (0.7% Iodine/74% IPA) Techni-Care® (3% Chloroxylenol-PCMX) Cultures: hallux, web spaces between toes, and control site Another study evaluated the efficacy of ChloraPrep, 0.7% iodine and 74% IPA (DuraPrep), and 3.0% chloroxylenol (Techni-Care) for eliminating bacteria from the foot. Infection rates in foot and ankle surgery are often higher than in other kinds of surgery because it is difficult to remove bacteria from the forefoot. This prospective, randomized study included 125 evaluable patients undergoing foot and ankle surgery. Cultures were obtained from 5 additional subjects before surgical preparation to quantify the amount of bacteria present before antiseptic skin preparation. Cultures were obtained from the nail fold (hallux), the web space between the second and third toes and between the fourth and fifth toes, and the anterior tibia (the control site). Reference Ostrander RV, Botte MJ, Brage ME. Efficacy of surgical preparation solutions in foot and ankle surgery. J Bone Joint Surg Am. 2005;87(5): Ostrander RV, et al. Bone Joint Surg Am. 2005;87(5): 60
 DuraPrep® (0.7% Iodine/74% IPA) Techni-Care® (3% Chloroxylenol-PCMX) Cultures: hallux, web spaces between toes, and control site. Another study evaluated the efficacy of ChloraPrep, 0.7% iodine and 74% IPA (DuraPrep), and 3.0% chloroxylenol (Techni-Care) for eliminating bacteria from the foot. Infection rates in foot and ankle surgery are often higher than in other kinds of surgery because it is difficult to remove bacteria from the forefoot. This prospective, randomized study included 125 evaluable patients undergoing foot and ankle surgery. Cultures were obtained from 5 additional subjects before surgical preparation to quantify the amount of bacteria present before antiseptic skin preparation. Cultures were obtained from the nail fold (hallux), the web space between the second and third toes and between the fourth and fifth toes, and the anterior tibia (the control site). Reference. Ostrander RV, Botte MJ, Brage ME. Efficacy of surgical preparation solutions in foot and ankle surgery. J Bone Joint Surg Am. 2005;87(5): Ostrander RV, et al. Bone Joint Surg Am. 2005;87(5):")
61
2% CHG/70% IPA for Foot and Ankle Surgery
The highest percentage of positive cultures were obtained in the 3% Chloroxylenol (Techni-Care) group, while the lowest percentages were obtained from the 2% CHG/70% IPA (ChloraPrep) group. The positive culture rates in the ChloraPrep group were statistically significantly lower than in the 0.7% Iodine 74% IPA (DuraPrep) group at the hallux and toe sites (P<0.01, P<0.05, respectively). The control site was the anterior tibia, 12 centimeters proximal to the ankle joint. Reference Ostrander RV, Botte MJ, Brage ME. Efficacy of surgical preparation solutions in foot and ankle surgery. J Bone Joint Surg Am. 2005;87-A: Control = anterior tibia, 12 cm proximal to the ankle joint. Ostrander RV, et al. J Bone Joint Surg Am. 2005;87-A: 61
 group, while the lowest percentages were obtained from the 2% CHG/70% IPA (ChloraPrep) group. The positive culture rates in the ChloraPrep group were statistically significantly lower than in the 0.7% Iodine 74% IPA (DuraPrep) group at the hallux and toe sites (P<0.01, P<0.05, respectively). The control site was the anterior tibia, 12 centimeters proximal to the ankle joint. Reference. Ostrander RV, Botte MJ, Brage ME. Efficacy of surgical preparation solutions in foot and ankle surgery. J Bone Joint Surg Am. 2005;87-A: Control = anterior tibia, 12 cm proximal to the ankle joint. Ostrander RV, et al. J Bone Joint Surg Am. 2005;87-A:")
62
2% CHG/70% IPA for Foot and Ankle Surgery
This shows bacterial colony counts for each site. Overall, ChloraPrep was the most effective solution for eliminating bacteria from the hallux and toe sites (P<0.0001). Reference Ostrander RV, Botte MJ, Brage ME. Efficacy of surgical preparation solutions in foot and ankle surgery. J Bone Joint Surg Am. 2005;87-A: Ostrander RV, et al. J Bone Joint Surg Am. 2005;87-A: 62
. Reference. Ostrander RV, Botte MJ, Brage ME. Efficacy of surgical preparation solutions in foot and ankle surgery. J Bone Joint Surg Am. 2005;87-A: Ostrander RV, et al. J Bone Joint Surg Am. 2005;87-A:")
63
Prevention of SSIs Preoperative preparation of the surgical team
Clean underneath each fingernail prior to first surgical scrub (IB) After performing surgical scrub keep hands up and away from body; allow water to run from hands to elbows; dry with sterile towel (1B)
 After performing surgical scrub keep hands up and away from body; allow water to run from hands to elbows; dry with sterile towel (1B)")
65
Prevention of SSIs Management of infected or colonized surgical personnel Exclude from duty, surgical personnel who have draining skin lesions until infection eliminated or personnel have received adequate therapy (IB) Do not routinely exclude personnel colonized with S. aureus or group A strep unless personnel linked epidemiologically to outbreak (IB) Educate personnel regarding symptoms and signs of infection-have them report to OHS (IB)
 Do not routinely exclude personnel colonized with S. aureus or group A strep unless personnel linked epidemiologically to outbreak (IB) Educate personnel regarding symptoms and signs of infection-have them report to OHS (IB)")
66
Prophylactic Antibiotics
Antibiotics given for the purpose of preventing infection when infection is not present but the risk of postoperative infection is present. Cefazolin is widely used for clean operations.

67
Surgical Infection Prevention Arch Surg 2005;140:174
40.7 92.9 47.6 All Surgeries (34,133) 79.1 90.8 52.4 Hysterectomy (2,756) 41.0 75.9 40.6 Colon (5,279) 36.3 97.4 52.0 Hip/knee (15,030) 44.8 91.9 40.0 Vascular (3,207) 34.3 95.8 45.3 Cardiac (7,861) Antibiotic stopped within 24 hours % Correct Antibiotic Antibiotic within 1 hour Surgery (N)
 Hysterectomy (2,756) Colon (5,279) Hip/knee (15,030) Vascular (3,207) Cardiac (7,861) Antibiotic stopped within 24 hours. % Correct Antibiotic. Antibiotic within 1 hour. Surgery (N)")
68
Prevent Surgical Site Infections: Institute for Healthcare Improvement
Components if implemented reliably can eliminate SSIs Appropriate use of antibiotics: one hour before incision; appropriate antibiotics; discontinue with 24 h after surgery (Surgical Care Improvement Project-CMS Quality Indicator) Appropriate hair removal Maintenance of postoperative glucose control (<200mg/dl) for major cardiac surgery patients Establishment of postoperative normothermia for colorectal surgery patients
 Appropriate hair removal. Maintenance of postoperative glucose control (<200mg/dl) for major cardiac surgery patients. Establishment of postoperative normothermia for colorectal surgery patients.")
70
SSI: CDC Guidelines Patient characteristics Preoperative issues
Intra-operative issues Postoperative issues [[animated slide—mouse click for each text box]] The Guidelines for Prevention of Surgical Site Infection developed by the Hospital Infection Control Practices Advisory Committee of the CDC underscores the risk to patients of morbidity and mortality associated with surgical site infections (SSI). Risks associated with SSIs fall into the following categories: Patient characteristics Operative characteristics, including preoperative, intraoperative, and postoperative factors Primary modifiable risks are described in the next slides. Reference Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 70
. Risks associated with SSIs fall into the following categories: Patient characteristics. Operative characteristics, including preoperative, intraoperative, and postoperative factors. Primary modifiable risks are described in the next slides. Reference. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4):")
71
SSI: Primary Risk Factors
Endogenous microorganisms Skin-dwelling microorganisms Most common source S aureus most common isolate Fecal flora (gnr) when incisions are near the perineum or groin Exogenous microorganisms Surgical personnel (members of surgical team) OR environment (including air) All tools, instruments, and materials Most surgical site infections (SSIs) are caused by skin-dwelling microorganisms from the patient. Staphylococcus aureus is the most common isolate associated with the development of surgical site infections. Exogenous sources of pathogens that contribute to surgical site infection include surgical personnel, particularly surgical team members, who carry microorganisms on their person. The operating room environment, including the air itself, may be contaminated with microorganism that are transferred to the patient. All tools, instruments, and materials brought into the sterile field may harbor pathogens if they are not adequately sterilized. Reference Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 71
 when incisions are near the perineum or groin. Exogenous microorganisms. Surgical personnel (members of surgical team) OR environment (including air) All tools, instruments, and materials. Most surgical site infections (SSIs) are caused by skin-dwelling microorganisms from the patient. Staphylococcus aureus is the most common isolate associated with the development of surgical site infections. Exogenous sources of pathogens that contribute to surgical site infection include surgical personnel, particularly surgical team members, who carry microorganisms on their person. The operating room environment, including the air itself, may be contaminated with microorganism that are transferred to the patient. All tools, instruments, and materials brought into the sterile field may harbor pathogens if they are not adequately sterilized. Reference. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. The hospital infection control practices advisory committee. Guidelines for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4):")
72
OR Environment Air Largest source of airborne microbial contamination is the OR staff Organisms become airborne as a result of conversation or shedding from the hair or exposed skin Microbial level directly proportional to the number of people moving about in the room Improved ventilation associated with decreased SSI

73
Prevention of SSIs Intraoperative (Ventilation)
Maintain 15 AC/hr (>3 fresh), positive pressure (IB) Filter all air through appropriate filters (IB) Introduce air at ceiling and exhaust near floor (IB) Keep OR doors closed as needed for passage of equipment, personnel, and patients (IB) Limit the number of OR personnel (IB) Consider ultraclean air for orthopedic implants (II)
, positive pressure (IB) Filter all air through appropriate filters (IB) Introduce air at ceiling and exhaust near floor (IB) Keep OR doors closed as needed for passage of equipment, personnel, and patients (IB) Limit the number of OR personnel (IB) Consider ultraclean air for orthopedic implants (II)")
74
OR Environment Ventilation
Three primary design components act to purify the OR air High-flow ventilation - 15 air changes per hour (3 outside air) High-efficiency filtration % Positive pressure relative to adjacent areas (prevents contamination from less clean areas) Maintain the temperature ( F [20-230C]) and relative humidity (30-60%)
 High-efficiency filtration % Positive pressure relative to adjacent areas (prevents contamination from less clean areas) Maintain the temperature ( F [20-230C]) and relative humidity (30-60%)")
75
OR Environment Environment as an Exogenous Source of Pathogens
Clean environment minimizes the risk of OR environmental surfaces and floors as a source of infection Microorganisms isolated from the OR are usually non-pathogens rarely associated with infection When inanimate sources implicated, the sources have been contaminated solutions, antiseptics, or dressings (not floors, walls or environmental surfaces)
")
76
Prevention of SSIs Intraoperative (Cleaning/disinfection environmental surfaces) Clean when visibly soiled/contaminated with EPA approved disinfectant before the next operation (IB) Do not perform special cleaning after contaminated or dirty surgery (IB) Do not use tacky mats (IB) Cleaning between surgery if no visible contamination (No recommendation)
 Do not perform special cleaning after contaminated or dirty surgery (IB) Do not use tacky mats (IB) Cleaning between surgery if no visible contamination (No recommendation)")
77
OR Environment Disinfection
OR environment (furniture, lights, equipment) should be damp-dusted with a germicide on a scheduled basis Exogenous microorganisms can contaminate surgical practice setting Disinfection is essential to reduce the risk of cross-infection Disinfection of these surfaces will control airborne microorganisms that might travel on dust and lint
 should be damp-dusted with a germicide on a scheduled basis. Exogenous microorganisms can contaminate surgical practice setting. Disinfection is essential to reduce the risk of cross-infection. Disinfection of these surfaces will control airborne microorganisms that might travel on dust and lint.")
78
OR Environment Disinfection
Floors should be cleaned with a low-level disinfectant For end-of-use cleaning, necessary to clean a 3-to-4 ft perimeter around the operative site (extended as necessary by contamination) Important to reestablish a clean environment after each operation For terminal daily cleaning, entire floor is cleaned Same cleaning procedures performed whether clean or contaminated case
 Important to reestablish a clean environment after each operation. For terminal daily cleaning, entire floor is cleaned. Same cleaning procedures performed whether clean or contaminated case.")
79
OR Environment Disinfectants
Low-level disinfectants are used for non-critical (skin contact) surfaces/furniture/lights Phenolics Quaternary ammonia compounds Chlorine (1:10 dilution of 5.25% sodium hypochlorite- blood spills)
 surfaces/furniture/lights. Phenolics. Quaternary ammonia compounds. Chlorine (1:10 dilution of 5.25% sodium hypochlorite- blood spills)")
80
OR Environment Reusable Items
Clean (in accordance to manufacturer’s recommendation) Lower the microbial load (mechanical or manual) Reduces organic and inorganic residual Disinfect or sterilize based on the risk of infection associated with the use of the item Critical items (sterile tissue, vascular system) must be sterile Semicritical (endoscopes) must be high-level disinfected
 Lower the microbial load (mechanical or manual) Reduces organic and inorganic residual. Disinfect or sterilize based on the risk of infection associated with the use of the item. Critical items (sterile tissue, vascular system) must be sterile. Semicritical (endoscopes) must be high-level disinfected.")
81
OR Environment Sterilization
Inadequate sterilization of surgical instruments has resulted in SSI Surgical instruments can be sterilized by steam, ethylene oxide, hydrogen peroxide plasma, dry heat or other approved methods Microbial monitoring of sterilization performance is necessary and can be accomplished by biological indicators

82
Prevention of SSIs Intraoperative (Sterilization of surgical instruments) Perform flash sterilization only for patient care items that will be used immediately. Do not use for reasons of convenience, as an alternative to purchasing additional instrument sets, or to save time (IB) Sterilize all surgical instruments according to published guidelines (IB)
 Sterilize all surgical instruments according to published guidelines (IB)")
83
OR Environment Microbiologic Sampling
No standardized parameters by which to compare microbial levels obtained from cultures of ambient air or environmental surface Routine microbiologic sampling cannot be justified Environmental sampling should only be performed as part of an epidemiologic investigation

84
Prevention of SSIs Intraoperative (Surgical attire and drapes-minimize patient’s exposure to skin, mm, or hair of surgical team and protect team from exposure to blood and OPIM) Wear a mask to fully cover the mouth and nose, and a cap or hood to fully cover hair on head and face (IB) Wear sterile gloves (IB) Do not wear shoe covers to prevent SSIs (IB)
 Wear a mask to fully cover the mouth and nose, and a cap or hood to fully cover hair on head and face (IB) Wear sterile gloves (IB) Do not wear shoe covers to prevent SSIs (IB)")
85
Prevention of SSIs Intraoperative
Use materials for surgical gowns and drapes that are effective barriers when wet (IB) Change surgical scrubs when visibly soiled, contaminated and/or penetrated by blood (IB)
 Change surgical scrubs when visibly soiled, contaminated and/or penetrated by blood (IB)")
86
Prevention of SSIs Asepsis and surgical technique
Adhere to the principles of asepsis when placing intravascular devices, spinal or epidural anesthesia catheters, or when dispensing and administering IV drugs (IB) Handle tissue gently, maintain effective hemostasis, minimize devitalized tissue and foreign bodies, and eradicate dead space at the surgical site (IB)
 Handle tissue gently, maintain effective hemostasis, minimize devitalized tissue and foreign bodies, and eradicate dead space at the surgical site (IB)")
87
Prevention of SSIs Asepsis and surgical technique
Use delayed primary skin closure or leave an incision open to heal by second intention if the surgeon considers the surgical site to be heavily contaminated (IB) If drainage is necessary, use a closed suction drain. Place a drain through a separate incision distant from the operative incision. Remove the drain as soon as possible. (IB)
 If drainage is necessary, use a closed suction drain. Place a drain through a separate incision distant from the operative incision. Remove the drain as soon as possible. (IB)")
89
SSI: CDC Guidelines Patient characteristics Preoperative issues
Intra-operative issues Postoperative issues [[animated slide—mouse click for each text box]] The Guidelines for Prevention of Surgical Site Infection developed by the Hospital Infection Control Practices Advisory Committee of the CDC underscores the risk to patients of morbidity and mortality associated with surgical site infections (SSI). Risks associated with SSIs fall into the following categories: Patient characteristics Operative characteristics, including preoperative, intraoperative, and postoperative factors Primary modifiable risks are described in the next slides. Reference Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4): 89
. Risks associated with SSIs fall into the following categories: Patient characteristics. Operative characteristics, including preoperative, intraoperative, and postoperative factors. Primary modifiable risks are described in the next slides. Reference. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4): Mangram AJ, et al. Infect Control Hosp Epidemiol. 1999;20(4):")
90
Prevention of SSIs Postoperative Incision Care
Protect with a sterile dressing for hours postoperatively an incision that has been closed primarily (IB) Wash hands before and after dressing changes and any contact with the surgical site (IB)
 Wash hands before and after dressing changes and any contact with the surgical site (IB)")
91
Prevention of SSIs Surveillance Use CDC definitions of SSI (IB)
When postdischarge surveillance is performed, use a method that accommodates available resources and data needs (II) Assign surgical wound classification upon completion of an operation (II) Record key variables shown to be associated with SSI (wound classification, ASA class, duration of operation)(IB)
 Assign surgical wound classification upon completion of an operation (II) Record key variables shown to be associated with SSI (wound classification, ASA class, duration of operation)(IB)")
92
Surveillance at UNC Hospitals
Follow certain operations for SSIs and benchmark Vaginal hysterectomy CABG Cholecystectomy Knee replacement Mastectomy Ventricular shunt Laminectomy

93
Prevention of SSIs Surveillance
Periodically calculate operation-specific SSI rates (IB) Report stratified, operation-specific SSI rates to surgical team members (IB) Provide infection control committee with coded surgeon specific data (No recommendation)
 Report stratified, operation-specific SSI rates to surgical team members (IB) Provide infection control committee with coded surgeon specific data (No recommendation)")
94
CDC Surgical Site Infection Prevention Guidelines - 1999
Category IA and IB No prior infections 15 air changes/hr in OR Do not shave in advance Keep OR doors closed Control glucose in D.M. pts Use sterile instruments Stop tobacco use Wear a mask Shower with antiseptic soap Cover hair Prep skin with approp. agent Wear sterile gloves Surgical team nails short Gentle tissue handling Surgical team scrub hands DPC for heavily contaminated Exclude I/C surgical team wounds Give prophylactic antibiotics Closed suction drains (when used) Pos pressure ventilation in OR Sterile dressing x hr SSI surveillance with feedback to surgeons
 Pos pressure ventilation in OR Sterile dressing x hr SSI surveillance with feedback to surgeons.")
95
PLUS Antibacterial Sutures
Antibacterial agent (triclosan) kills bacteria and inhibits colonization of the suture Proven in vitro to create a zone of inhibition around the suture against common SS pathogens: S. aureus, MRSA, CONS Triclosan-coated sutures may be valuable in reducing SSIs. Ann Thorac Surg 2007:87:232 Hospitals challenged with the question whether to invest in this technology for routine surgical wound closure-must review data on SSI reduction, cost of surgical wounds, wound care, prolonged hospitalization, suture cost, etc
 kills bacteria and inhibits colonization of the suture. Proven in vitro to create a zone of inhibition around the suture against common SS pathogens: S. aureus, MRSA, CONS. Triclosan-coated sutures may be valuable in reducing SSIs. Ann Thorac Surg 2007:87:232. Hospitals challenged with the question whether to invest in this technology for routine surgical wound closure-must review data on SSI reduction, cost of surgical wounds, wound care, prolonged hospitalization, suture cost, etc.")
96
National Organizations Targeting Infection Prevention as a Measure of Quality
Centers for Medicare and Medicaid Services (CMS) Institute for Healthcare Improvement (IHI) National Quality Forum The Joint Commission Consumers Union-report HAIs
 Institute for Healthcare Improvement (IHI) National Quality Forum. The Joint Commission. Consumers Union-report HAIs.")
97
Center for Medicare and Medicaid Services FY2008
Rule adopts eight conditions for which CMS will not provide higher payments if the event occurs while a patient is under the care of the hospital, effective FY09 Object left in surgery Air embolism Blood incompatibility

98
Center for Medicare and Medicaid Services FY2008
CMS will not provide higher payments Catheter-associated urinary tract infections Pressure ulcers Vascular catheter associated infections Mediastinitis after coronary artery bypass graft Falls Agency intends to consider other HAIs and medical errors for non-payment in future years Hospitals cannot bill patients for the amount CMS refuses to pay

99
Center for Medicare and Medicaid Services FY2008
Intent Mobilize hospitals to improve care and keep patients safe Consensus among public health experts that HAI/errors are preventable Encourage stricter adherence to proven infection prevention practices Unintended Consequences Avoidance of patients perceived to be at risk for infections Hospitals may game the system by falsifying codes to avoid non-payment

100
Public Reporting of HAIs
Advisory Commission on Hospital Infection Control Purpose: prepare hospitals for the public disclosure of HAIs as may be required by law for specific clinical procedures Class I surgical site infections Ventilator-associated pneumonia Central-line related bloodstream infections Must ensure quality and accuracy of information Commission will submit an interim report May 2008 and final report 2009 General Assembly

101
Prevent Surgical Site Infections: Institute for Healthcare Improvement
Components if implemented reliably can eliminate SSIs Appropriate use of antibiotics Appropriate hair removal Maintenance of postoperative glucose control for major cardiac surgery patients Establishment of postoperative normothermia for colorectal surgery patients

102
Conclusions Surgical site infections result in significant patient morbidity and mortality, and increased hospital cost Reduction in surgical site infections can be achieved by strict adherence to standard surgical guidelines Observations have revealed failure to follow standard guidelines Strict adherence to standard guidelines crucial to reduce SSIs

103
TOPICS Epidemiology of healthcare associated infections (HAI)
Review the morbidity, mortality, and economic consequences of HAIs Discuss the risk factors and etiology of SSIs Provide strategies to prevent SSIs National initiatives to prevent SSIs

104
Thank you

Similar presentations




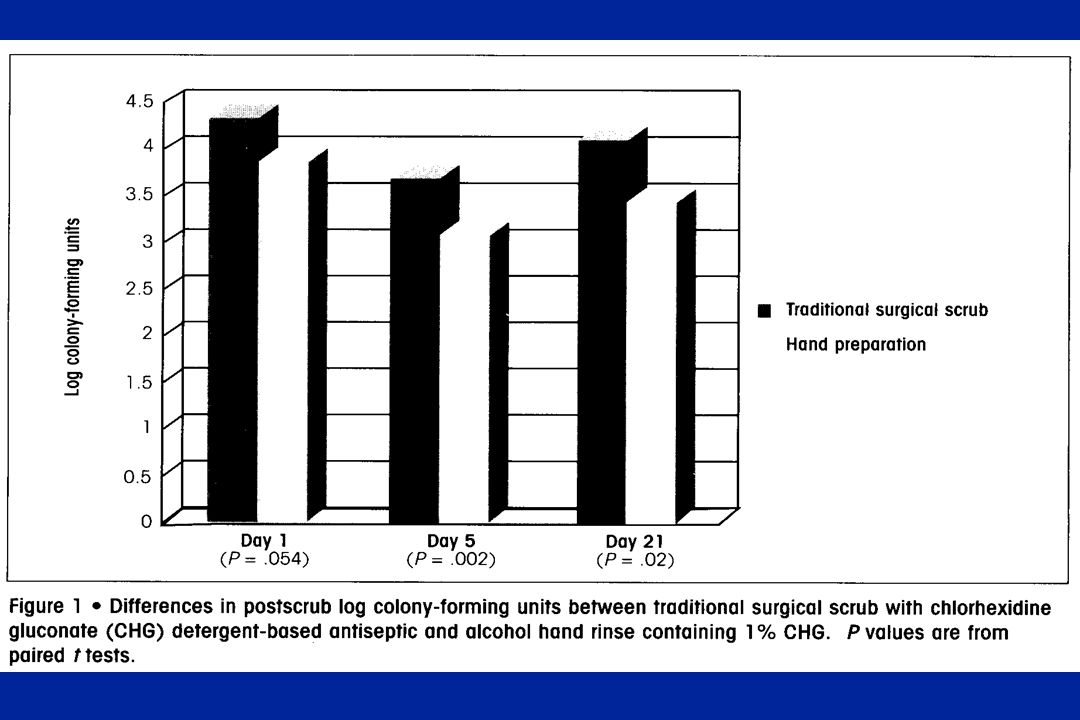







: What the Direct Caregiver Should Know>")

















