Download presentation
Presentation is loading. Please wait.

1
Opening Pandora’s Box Professional attitudinal barriers to implementing practice nurse-led SBIRT in general practice Jock Mackenzie Project Officer Reducing Risky Drinking Project Southcity Clinic Bayside Medicare Local

2
Reducing Risky Drinking Project Southcity Clinic - Bayside Medicare Local - July 2012 Substance dependent and DD clients w complex needs Training, consultancy and support services Reducing Risky Drinking Project RRDP Practice nurse-led SBIRT in general practice Barriers and Facilitators Report & Recommendations Professional attitudinal barriers Research questions

3
Opening Pandora’s Box

4
Design and Methods Exploration of reasons for low rates of SBIRT Literature review on barriers to SBIRT Focus group with practice nurses and nurse mentor Key informant survey of steering group members Delphi technique Quantitative screening outcomes data

5
NICS Barriers Tool the innovation itself (and its implementation) the health professional level the patient level the organizational context the economic and political context NICS (2006) Identifying Barriers to Evidence Uptake. National Institute of Clinical Studies http://www.nhmrc.gov.au/nicshttp://www.nhmrc.gov.au/nics

6
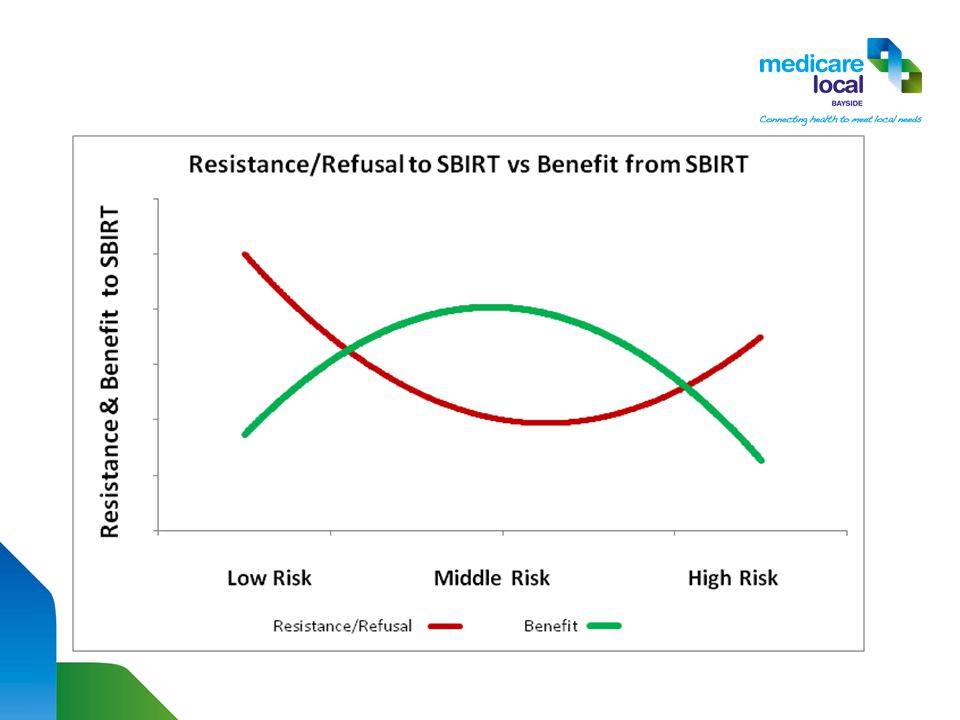
Some Interesting Findings Poor acceptance of NHMRC Alcohol Guidelines Influence of clinician’s personal drinking habits Lack of confidence in managing patient resistance Over-estimation and over-generalization of patient resistance Differential patient resistance by level of risk

7
Addressing Risky Drinking in General Practice

8
Addressing harms in General Practice Harms well known & occur to drinkers and others Most harms avoidable and SBIRT effective response GP and PN well placed to detect and treat Most risky drinkers won’t seek help or consider an issue Risky drinking goes unrecognized & unaddressed Unless obvious or client raises as an issue Many reasons but PRIMARY reason is clinicians avoid

9
What is SBIRT? Screening, BI and Referral to Treatment (& follow ups) Non-treatment seeking risky drinkers in primary care Aim to encourage and initiate behaviour change Different evidentiary support, resources barriers and enablers Very important stage precedes - Engagement Failure to engage is the KEY barrier to SBIRT
 Non-treatment seeking risky drinkers in primary care Aim to encourage and initiate behaviour change Different evidentiary support, resources barriers and enablers Very important stage precedes - Engagement Failure to engage is the KEY barrier to SBIRT.")
10
Evidence for SBIRT Short term evidence strong (Babor et al., 2007) Long-term population health simulation models promising Collins & Lapsley (2008) reduce risky drinking by 50%, avoid 2,000 early deaths and directly save $6 billion SIPS Study UK - just attempting screening beneficial Brief feedback has same impact as more extended BIs Simply raising question initiates dialogue - active ingredient Follow the latest research! tinyurl.com/findingsSBIRTtinyurl.com/findingsSBIRT Ashton, M. (2012) Alcohol screening and brief interventions in primary health care. Drug Findings http://findings.org.uk/
 Alcohol screening and brief interventions in primary health care. Drug Findings")
11
Barriers to SBIRT in General Practice Lack of time, awareness, training, funding & access to AOD Competing priorities, scepticism, confusion re guidelines, lack of role security Fear of offending and losing rapport Most patients not seeking help for drinking Challenging risky drinking taboo in many cultures More a clinician drinks, the less they engage patients Professional anxiety is THE main barrier to SBIRT

12
Perceptions of Resistance Clinicians overstate and overgeneralise patient resistance Patients consider appropriate, important, not embarrassed While some do object and a few may not come back Worried patients appreciate a chance to discuss and those not worried are usually open to information and advice Resistance does happen and confidence to manage is KEY Johnson, et al (2010). Barriers and enablers to implementing SBIRT: Systematic review of qualitative evidence J Public Health (2011) 33(3): 412-421
 33(3):")
13
Perception of Resistance

15
Tips and Tricks for Engaging Engaging not easy when no obvious link w presentation Non-routine clinical context health checks or registration Many different strategies for creating opportunity Includes screening in ‘Patient Information Update Form’ Take the focus off patient, refocus on the process itself Framing screening as health promotion campaign Link presentation e.g. diabetes/ anxiety/insomnia to drinking Appeal to pride in managing good health Acknowledge questions may seem odd which may defuse refusal Be creative! All of these are contained in the Clinical Protocol

16
Products from the Project Web resource at bml.org.au search for SBIRT This will contain: The Barriers and Enablers Report “Opening Pandora’s Box” Newletter articles about the project The Clinical Protocol Training materials Online E3 Learning Module with APNA March 2013

17
Further research ideas Compare self-reported resistance of patients vs perceived resistance Attitudes of patients to engagement By demographics, by CALD, by risk level, by Stage of Change Perceived resistance as outcome measure Is there a compliant middle ground Differential effectiveness of components of SBIRT in initiating and maintaining therapeutic conversations

18
References Please visit http://www.bml.org.au and search for SBIRT or emailhttp://www.bml.org.au jmackenize@southcityclinic.org.au

Similar presentations












>")






