Download presentation
Presentation is loading. Please wait.

1
Care Management of a Population: Focus on Asthma CHOP Care Network Chestnut Hill 7700 Germantown Ave Philadelphia, PA 19118 Sue Kammerle RN,CPN

2
We are coordinating care by having systems in place to accomplish our Practice Goals Decrease asthma hospitalizations of our patients Decrease acute episodes (hospital, office based, urgent care) of our patients Improve functional measures of well being (school attendance, sleep, participation in desired activities) of our patients Improved our patients and families perception of control and knowledge of disease To incorporate evidence based practices within all clinical decisions To develop an infrastructure that imbeds clinical goals into workflow and is sustainable To develop workflows that are efficient and fiscally sound
 of our patients Improve functional measures of well being (school attendance, sleep, participation in desired activities) of our patients Improved our patients and families perception of control and knowledge of disease To incorporate evidence based practices within all clinical decisions To develop an infrastructure that imbeds clinical goals into workflow and is sustainable To develop workflows that are efficient and fiscally sound")
3
Risk Stratification The National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma August 2007

4
Clinical Care System – Evidenced Based Care 4 http://www.nhlbi.nih.gov/guidelines/asthma/ Snapshot -- defining diagnosis “language”

5
High Risk Patients Care Manager receives referral from primary clinician regarding patient who has asthma which is NOT in control, not based on severity. Patient may have had multiple exacerbations, ER visits or hospitalizations. Care Manager may identify patients from ER or Hospitalization Review and recommend need for Care Coordination to provider Focus of telephone contacts are to identify reasons for non adherence to recommended treatments and asthma care plan. Care Manager then will provide appropriate education and/or resources needed to improve adherence focusing on the goal of keeping asthma symptoms IN CONTROL. Communicates with primary clinician regarding contacts with family through copying telephone encounters and focused discussion on planning future interventions. May refer to community resources, such as LaSalle Neighborhood Nurses as needed to make home visits.

6
All asthma patients should have a diagnosis on the active problem list intermittent, mild, moderate, severe asthma NOS, asthma intrinsic, asthma exacerbation, EIA, etc. are not to be used on Problem list All asthma patients should have an active prescription (developed order templates aligned with agreed standards). a short acting bronchodilator an inhaled steroid for all with a Persistent Diagnosis (mild, moderate, severe) 6 Clinical Care System - Asthma Standard Care / Planned Care / Evidence Based Care Our sites attempted to standardize care throughout the practice -- goal to keep it simple
. a short acting bronchodilator an inhaled steroid for all with a Persistent Diagnosis (mild, moderate, severe) 6 Clinical Care System - Asthma Standard Care / Planned Care / Evidence Based Care Our sites attempted to standardize care throughout the practice -- goal to keep it simple.")
7
7 Clinical Care System - Asthma Standard Care / Planned Care / Evidence Based Care Snapshot designed with critical information

8
All patients with an asthma diagnosis should receive an annual flu vaccine (annual EMR mining with follow-up planned calls). All patients with a Asthma Diagnosis should have an active Asthma Care Plan. Frequency of Asthma encounters (planned /follow-up encounters) 1 year from last WCC visit for those with an intermittent asthma diagnosis. 6 months from last WCC or last “asthma assessment encounter” for those with a mild persistent asthma diagnosis 4 months from last WCC or last “asthma assessment encounter” for those with a moderate persistent asthma diagnosis 3 months from last WCC or last “asthma assessment encounter” for those with a severe persistent asthma diagnosis 1 month or less for uncontrolled asthma 8 Clinical Care System - Asthma Standard Care / Planned Care / Evidence Based Care Our sites attempted to standardize care throughout the practice -- goal to keep it simple
 1 year from last WCC visit for those with an intermittent asthma diagnosis. 6 months from last WCC or last asthma assessment encounter for those with a mild persistent asthma diagnosis 4 months from last WCC or last asthma assessment encounter for those with a moderate persistent asthma diagnosis 3 months from last WCC or last asthma assessment encounter for those with a severe persistent asthma diagnosis 1 month or less for uncontrolled asthma 8 Clinical Care System - Asthma Standard Care / Planned Care / Evidence Based Care Our sites attempted to standardize care throughout the practice -- goal to keep it simple.")
9
Recommended medications Ventolin HFA - recommended short acting bronchodilator (counter, on all formularies) Spacers with all mdi’s recomended Flovent HFA - recommended inhaled steroid for all patients with a persistent asthma diagnosis (dosing 2 puffs BID with spacer) Flovent 44 - mild persistent asthma Flovent 110 - moderate persistent asthma Flovent 220 - severe persistent asthma 9 Clinical Care System - Asthma Standard Care / Planned Care / Evidence Based Care Our sites attempted to standardize care throughout the practice -- goal to keep it simple
 Spacers with all mdi’s recomended Flovent HFA - recommended inhaled steroid for all patients with a persistent asthma diagnosis (dosing 2 puffs BID with spacer) Flovent 44 - mild persistent asthma Flovent moderate persistent asthma Flovent severe persistent asthma 9 Clinical Care System - Asthma Standard Care / Planned Care / Evidence Based Care Our sites attempted to standardize care throughout the practice -- goal to keep it simple")
10
Office Based Education OBJECTIVE: To implement the EPR-3 guidelines by providing clinicians and support staff appropriate training in the pathophysiology, diagnosis, treatment guidelines and educational goals for patients and their families

11
Methods for providing staff education Monthly scheduled business meetings for providers included discussion of guidelines Scheduled presentations for clinicians, nurses and support staff by office based nurse practitioners and consultants Two nurse practitioners in our office have become Certified Asthma Educators and can provide on to one in house review of guidelines, curriculum, mentoring for patient education to clinicians, nurses and medical assistants

12
Resources Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma (EPR-3) August 2007 Association of Asthma Educators Curriculum www.asthmaeducators.org www.asthmaeducators.org CHOP Patient Communication Focal Points CHOP In patient Asthma Teaching Script CHOP Patient Family Education Manual Teaching Sheets CHOP DVD: “Controlling Asthma, A Guide for Families” CAPP, Community Asthma Prevention Program of Philadelphia: Four Visit Education Plan for the Asthma Prevention Office Visit “Culturally –Competent Asthma Education: A Continuing Education Monograph”, from the Association of Asthma Educators, Maureen George, MSN, RN, CS
 August 2007 Association of Asthma Educators Curriculum CHOP Patient Communication Focal Points CHOP In patient Asthma Teaching Script CHOP Patient Family Education Manual Teaching Sheets CHOP DVD: Controlling Asthma, A Guide for Families CAPP, Community Asthma Prevention Program of Philadelphia: Four Visit Education Plan for the Asthma Prevention Office Visit Culturally –Competent Asthma Education: A Continuing Education Monograph , from the Association of Asthma Educators, Maureen George, MSN, RN, CS")
13
13 Asthma Care Assistant Populates in Telephone and Office Encounters

14
Triage Nurse Responsibilities Refill Encounters of Asthma Medications to include Assessment of Current Status, Plan is to use Asthma Control Tool Nurses to be looking also at entire patient: Is medication being refilled too soon? Has patient been in office for yearly well visit? Has patient been in office for appropriate follow up based on asthma diagnosis?

15
Triage Nurse Responsibilities Using Barton Schmitt Protocols and EPIC templates to document telephone encounter for Acute Symptoms. Phone follow up for office visits for exacerbations, ER visits or Hospitalizations: Clarification of family’s understanding of Asthma Care Plan including medication and adherence to it or barriers to adherence. Make appropriate in office follow up appointment with primary clinician. HAS BEEN TARGETED TO ALL PATIENTS WITH ASTHMA, REGARDLESS OF SEVERITY OR PRIMARY CLINICIAN. Protocols exist for ER and Hospital follow-up

16
16 Asthma Control Tool

17
Clinical Nurses Asthma Care Assistant in encounter ACT on all well visits for patients with asthma Asthma Education Modules Consignment of spacers and nebulizer Patient education handouts Asthma Care Plans

18
Identification of Asthma and Highest Risk Care Coordination Patients 18

21
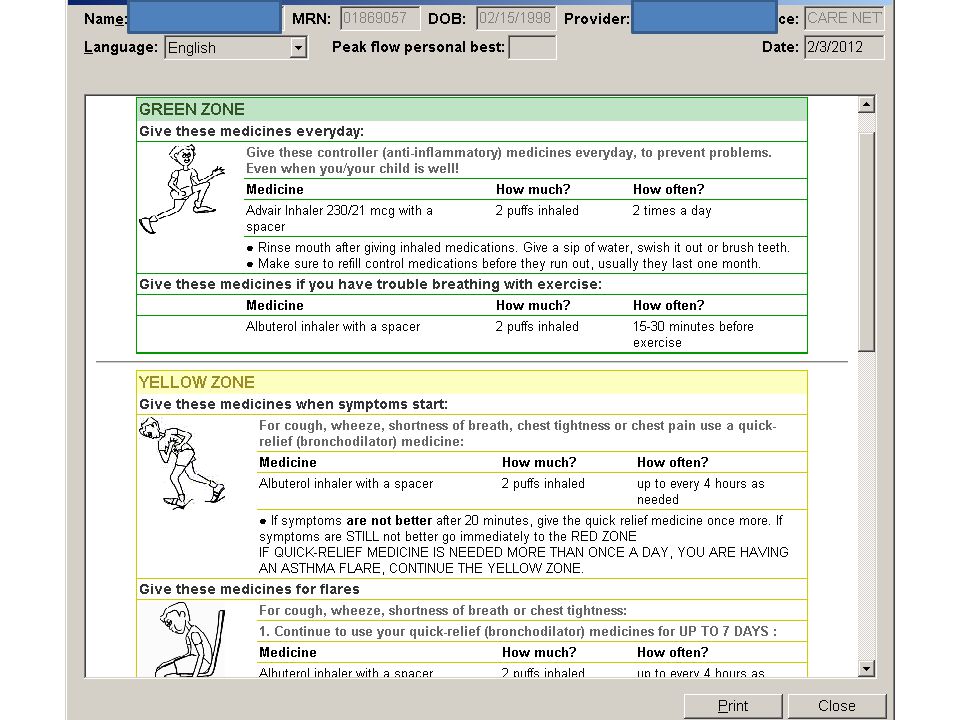
21 Patient Education Linked to patient education material

22
Coordination of Highest Risk Patients Patient identified in Problem List as Advance Care Planning Focus of telephone contacts are to identify reasons for non adherence to recommended treatments and asthma care plan. Care Manager then will provide appropriate education and/or resources needed to improve adherence focusing on the goal of keeping asthma symptoms IN CONTROL. Communicates with primary clinician regarding contacts with family through copying telephone encounters and focused discussion on planning future interventions. May refer to community resources, such as LaSalle Neighborhood Nurses as needed to make home visits. EMR function has Care Coordination pool-encounters are routed by providers and nursing staff Meet with patient and parents in office for further review of needs. Referral staff route encounter to CC when an Advance Care Planning Patient requests a referral.

23
Care Coordination ER visits Primary Responsibility of Care Coordinator Review all ER reports recieved Review all calls to CHOP After Hours for those with disposition of Referred to ER Call parent to follow up, assess current status, medications, and need for office follow up Make note of any needs assessed during phone call such as needs for education or equipment as a heads up to the clinician and staff seeing patient in the office for follow up Keep encounter active in EMR if unable to reach parent as a reminder that additional phone calls may be needed. Make note in Snapshot of asthma ER and Hospital visits- an easy visual reminder if has frequent ER visits A triage nurse may the the first to receive a call from the parent. They will do the follow up and then route the call to Care Coordination for further review.

25
Care Coordination Hospitalizations Place call to parent while still inpatient Notify Primary Clinician and Care Coordination staff of admission Keep encounter active in EMR to follow patient course Place call after discharge to assess current status, medications and need for office follow up

29
In Conclusion Though Care Coordination within our office we are working to keep our patients in control with thorough Assessment, Education, Intervention and Follow Up.

Similar presentations








 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")















