Download presentation
Presentation is loading. Please wait.

1
Musculoskeletal Imaging – The Basics Laurie Lomasney, MD Department of Radiology Loyola University Medical Center

2
Musculoskeletal Imaging Technology Advances in Imaging

3
MSK Imaging – Imaging Modalities Plain Radiographs Nuclear Scintigraphy Ultrasound Computed Tomography Magnetic Resonance Imaging

4
Plain Radiographs Widely available Reproducible Patient friendly ‘Inexpensive’ Usually the indicated primary imaging modality

5
Plain Radiographs Standard protocols available Consider the pathology in question –Image area of question, not the vicinity “One view is No view” Supplemental views possible in most locations

7
Plain Radiographs - Obvious

8
Plain Radiographs – 2 views

9
Posterior Dislocation

10
Plain Radiographs – Extra views Radial Head Fx

11
Plain Radiographs – Extra views Scaphoid Fx

12
Nuclear Scintigraphy Most common = Bone Scan Very sensitive for skeletal pathology Mildly sensitive for soft tissue pathology Usually nonspecific as an isolated test Mostly patient friendly; no significant environmental exposure Small-moderate expense

13
Nuclear Scintigraphy Excellent for specific pathologies –Osteomyelitis –Metastases – Not Multiple myeloma –Occult fracture Reasonably reassuring –Normal is usually normal

14
Nuclear scintigraphy – Bone Scan IV injection radioisotope (Tc-99m) bound to phosphate +/- dynamic imaging Approx 3 hour delay Delayed static imaging with a superficial detector
 bound to phosphate +/- dynamic imaging Approx 3 hour delay Delayed static imaging with a superficial detector")
16
Nuclear Scintigraphy – Bone Scan Osteomyelitis

17
Nuclear Scintigraphy 2 nd MT stress fracture

18
Ultrasound Not available at all institutions Reproducible in trained hands Excellent for superficial soft tissue elements including tendons and muscle Patient friendly Small to moderate expense

19
Ultrasound Routine exam room equipped with adequate imaging devices Superficial gel (standard or aseptic) application with touch with transducer Usually static exam of architecture +/- vascularity assessment Potential for dynamic imaging
 application with touch with transducer Usually static exam of architecture +/- vascularity assessment Potential for dynamic imaging")
21
Ultrasound CephCaud Cephalad Caudad Calcaneus

22
Ultrasound – Achilles Tendon Intrasubstance tear

23
Ultrasound – Patellar tendon Proximal patellar tendonitis – Jumper’s Knee

24
Computed Tomography (CT) Widely available Reproducible, although variety of techniques Excellent bone assessment Occasionally useful for soft tissue assessment Patient friendly Moderate expense Interventional options
 Widely available Reproducible, although variety of techniques Excellent bone assessment Occasionally useful for soft tissue assessment Patient friendly Moderate expense Interventional options")
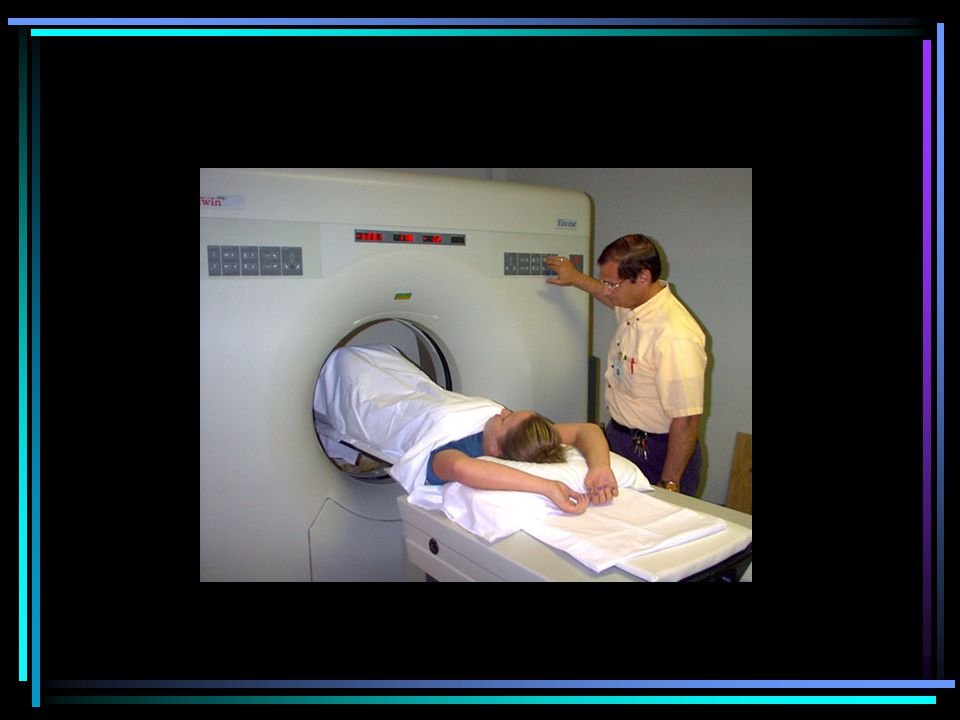
25
Computed Tomography Usually supine axial exam, with some alternative positioning options Can develop reformatted images after exam for alternative views Imaging time in seconds, rarely minutes Usually without IV or oral contrast

27
CT - Fractures Scaphoid fracture

28
CT - Dislocation Lis Franc Fx/Dislocation

29
CT – Bony anomalies Midsubtalar coalition

30
Magnetic Resonance Imaging Widely available, but non-standardized imaging techniques Reproducible Excellent for soft tissue pathology Good-excellent for bone pathology NOT patient friendly Large expense

31
MRI – Absolute Contraindications Cardiac Pacemakers Electronic stimulators Metallic foreign bodies in the orbit Body habitus beyond limits of physical unit Huge listing maintained in MRI facility

32
MRI - Relative Contraindications Penile prostheses IUD’s Cardiac valves Berry aneurysm clips Retained bullet fragments Claustrophobia Huge listing in MRI facility

33
MRI Usually performed with patient supine Multiplanar imaging obtained without changing position One exam = one body part Average exam time 45 minutes; most patients can’t last >2 hours Strict guidelines for sedation Optional contrast – Rad usually decides for body imaging

35
MRI – Trauma Osteochondritis dissecans

36
MRI – Trauma Femoral Neck Fracture

37
MRI - Trauma Tear vastus medialis

38
MRI – Internal Derangement

39
Supraspinatus tear= Full thickness, Full width Coronal PDCoronal T2

40
MRI – Internal Derangement Sagittal NLSagittal FT, FW Supra

41
MRI – Internal Derangement Sagittal, Meniscus NLPosterior Horn Tear

42
MRI – Internal Derangement Bucket handle meniscal tear

43
MRI – Internal Derangement Sagittal – Intact ACL Torn ACL

44
Imaging Plain radiographs are usually the starting point Most x-ray protocols work for most situations; Consider suppl. Views Secondary imaging techniques have specific advantages and disadvantages A specific question is more likely to get you a direct answer When in doubt, ask a Radiologist

45
THANK YOU Laurie Lomasney, MD

Similar presentations









 Ultrasound Magnetic Resonance Imaging (MRI) Radioisotopes Studies.>")













