Download presentation
Presentation is loading. Please wait.

1
Bunch of Heart Stuff Chemeketa Community College EMT-Paramedic Program

2
Objectives Left Ventricular Failure Right Ventricular Failure Pulmonary Edema Cor Pulmonale Acute Pulmonary Embolism EKG’s

3
Left Ventricular Failure Affects over 2% of US pop. Disproportionate # of EMS calls #1 Dx of inpatients >65 Incidence of CHF doubles per decade of life Mortality Rate with CHF 8 times for men 5 times for women

4
Left Ventricular Failure The failure of the LV to effectively pump forward Synonymous with CHF Acute CHF Rapid Chronic CHF Slow Midnight Shoppers

5
LVF Common Causes Systemic HTN –Afterload Coronary Artery Disease –Arteriosclerosis/Atherosclerosis Ischemia –Local/temporary occlusion

6
LVF Common Causes Infarction –Permanent, necrosis Cardiomyopathy –Diseased heart muscle tissue ETOH Enlargement

7
LVF Causes Volume overload –Bag of Potato Chips Severe anemia –Hypoxemia

8
LVF Fluid will collect in LA Small & Relatively incapable Pulmonary Vasculature Fills Pulmonary Congestion Occurs Pulmonary Edema 2 nd to LVF

9
LVF S/S Generalized Weakness Fatigue Chest Pain May be masked by respiratory complaint Anxiety Dyspnea

10
LVF S/S Tachypnea Orthopnea Paroxysmal Nocturnal Dyspnea Elevation of pulmonary venous & cap pressures Wakening from sleep Decrease in exercise tolerance

11
LVF S/S Rales Wheezes Reflex Airway Spasm Cardiac Asthma Rhonchi (Larger airway) Dull percussion at lung bases
 Dull percussion at lung bases")
14
Edema in Lungs

15
LVF S/S Productive Cough Foamy-Blood-tinged sputum Cyanosis B/P Initial HTN

16
LVF S/S Pulse Rapid Possible Dysrhythmia –Location of infarct Diaphoresis

17
Right Ventricular Failure Causes #1 Cause of RVF is LVF Stenosis: –Pulmonary valve –Mitral Valve Pulmonary Vascular HTN RV AMI

18
RVF – Who Cares Inability of RV to pump forward Overwhelmed by venous return Backflow in systemic circulation

19
RVF – S/S Tachycardia Venous Congestion Engorged Liver, spleen JVD Peripheral Edema Dependent Edema Pitting Edema Sacral (Bedridden)
")
20
RVF-S/S Ascites Accumulation of serous fluid in peritoneal cavity – Taber’s 19 th Pleural Effusion Peripheral Cyanosis Tachy if isolated RVF Right sided hypertrophy X-ray

21
RVF – S/S Clubbing of fingers Dx: Chronic Hypoxia with RHF Most of the other LVF S/S also CP SOB Tachypnea Anxiety Etc…

22
Cor Pulmonale Cause of RVF Pulmonary Parenchymal or vascular disease CP is a disease process Case Scenario Explanation

23
Cor Pulmonale – Case 58 yo male Hx of Chronic bronchitis or emphysema Typical S/S of bronchitis Progression Deterioration of Pulmonary capillaries Alveolar Fibrosis Chronic Hypoxemia

24
Cor Pulmonale – Case Progression caused: Increase in pulmonary artery pressures Result RV afterload increase –RV ill equipped RV Enlarges (Hypertrophy) Chronic RH HTN leads to RVF
 Chronic RH HTN leads to RVF")
25
Cor Pulmonale – Case Patient displays all signs of: RVF Initial causative pulmonary condition Voila’

26
Treatment of RVF & LVF CHF a circumstance not a Dx Treatment objectives Decrease myocardial: –Workload –Oxygen demand Increase force & efficiency of contraction Reduce fluid retention

27
Tx Decrease Workload No Physical activity Sitting upright Oxygen –Pt may tolerate BVM Morphine

28
Tx Vasodilatory Therapy (Nitrates) –AMI reperfusion –Container expansion reduces preload Increase Contractility Shock algorithm directs –Dopamine –Dobutamine –Norepinephrine
 –AMI reperfusion –Container expansion reduces preload Increase Contractility Shock algorithm directs –Dopamine –Dobutamine –Norepinephrine")
29
Tx Reduce Fluid Retention Diuretics –Lasix –Bumex

30
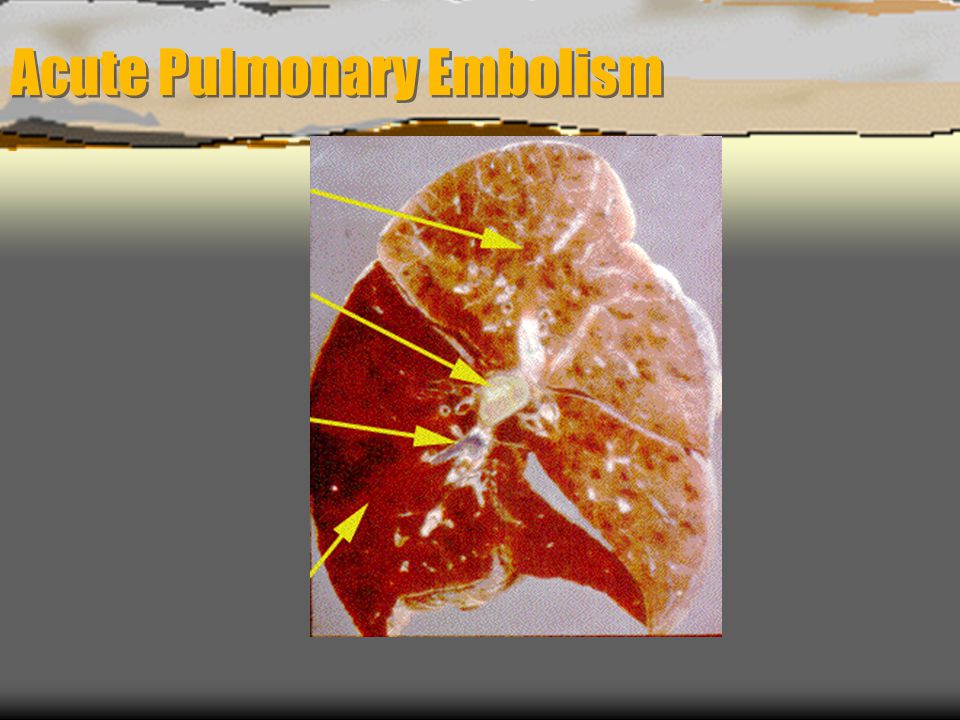
Acute Pulmonary Embolism Chemeketa Community College Paramedic Program

31
Acute Pulmonary Embolism

33
Defined Blood clot lodged in pulmonary artery Blocks pulmonary artery flow Supplied area ceases to function Decreased gas exchange V/Q mismatch

34
Defined Typically forms in deep veins of thighs Can also be fat or air

35
History Anticoagulation therapy Heparin – 1930s Streptokinase – 1930 Urokinase – 1951 1960s – Large study of clot resolution Recently TPA

36
Incidence Unknown, range from 50,000-100,000/yr Higher than diagnosed, most diagnosed postmortem 8% death rate with heparin tx 1/3 will die within 1 hour

37
Risk Factors Deep vein thrombosis Prolonged immobilization Surgery Trauma Pelvic or femur fractures Late pregnancy

38
Risk Factors Thrombophlebitis Certain meds Oral contraceptives Atrial fibrillation Smoking Unknown

39
Increasing Frequency Older population Malignancies More sedentary Heart failure COPD Surgical procedures

40
Presentation Variable and Non-specific Dyspnea Pleuritic chest pain Syncope Hemoptysis RHF Tachycardia

41
Presentation No physical findings significantly accurate Deep venous thrombosis in proximal lower ext. helpful for Dx Only about ½ source known

42
Why doesn’t lung tissue die from emboli like heart muscle? Lung has two blood supplies Pulmonary and Bronchial Share capillary beds

43
Pre-hospital Treatment Good Physical Exam and History Index of suspicion Airway High flow O 2 IV Rapid Transport

44
Treatment ??? Heparin Thrombolytic agents Streptokinase TPA Catheter fragmentation Catheter embolectomy Open-chest embolectomy

45
Definitive Diagnosis ???? Angiographic V/Q scan (venous/perfusion mismatch) Operative Multiple sources of evidence
 Operative Multiple sources of evidence.")
46
Differential Diagnosis Pneumonia Herpes Zoster Pleurisy COPD Rib fracture Asthma Angina MI Pneumothorax Pancreatitis Hepatitis Salicylate OD Bronchitis Hyperventilation Lung carcinoma Sepsis TB Muscle pain Costochondritis CA Pericarditis CHF Percardial tamponade

47
Watch Out Extraordinarily difficult to diagnose Watch out for hyperventilation Young women

49
Group Projects! Work in Pairs and find the answers

50
List As Many Drugs As You Can That Will Dilate Blood Vessels. Name the source Describe why they work

51
List Drugs That Cause Tachycardias. Describe why they cause increase rate change

52
List Drugs that cause Bradycardias. Why do they cause them?

53
List Drugs that cause Hypertension. How do they do it?

54
Your patient has a heart rate of 140 bpm. What could be his problem?

Similar presentations












 Occurs when the right ventricle fails as an effective forward pump, causing back-pressure of blood into the systemic.>")





. “Heart (or cardiac) failure is the pathophysiological state in which the heart is unable to pump blood at a rate commensurate.>")



