Download presentation
Presentation is loading. Please wait.

1
DYSPHAGIA Lisa Granville, M.D. Associate Chair & Professor of Medicine Department of Geriatrics Florida State University Copyright 2008, Florida State University College of Medicine. This work was supported by a grant from the Donald W. Reynolds Foundation. All rights reserved.

2
Today’s Learning Objectives: Develop an understanding of the five stages of swallowing functionDevelop an understanding of the five stages of swallowing function Relate at least five of the common signs and symptoms of swallowing abnormalities to etiologic conditionsRelate at least five of the common signs and symptoms of swallowing abnormalities to etiologic conditions Describe the swallow evaluation process including use of radiological assessmentDescribe the swallow evaluation process including use of radiological assessment Compare and contrast the benefits and limitations of artificial feeding for dysphagic patientsCompare and contrast the benefits and limitations of artificial feeding for dysphagic patients

3
Importance of Eating PleasurePleasure SocializationSocialization Maintenance of healthMaintenance of health

4
Mr. D, a 72 year old man living in a nursing home, has had a right sided stroke. He has impulsive behavior with poor judgment consistent with right sided brain damage. What feeding and/or swallowing concerns might exist for this patient?What feeding and/or swallowing concerns might exist for this patient?

5
DYSPHAGIA - from the Greek dys = difficulty phagia = swallowing

6
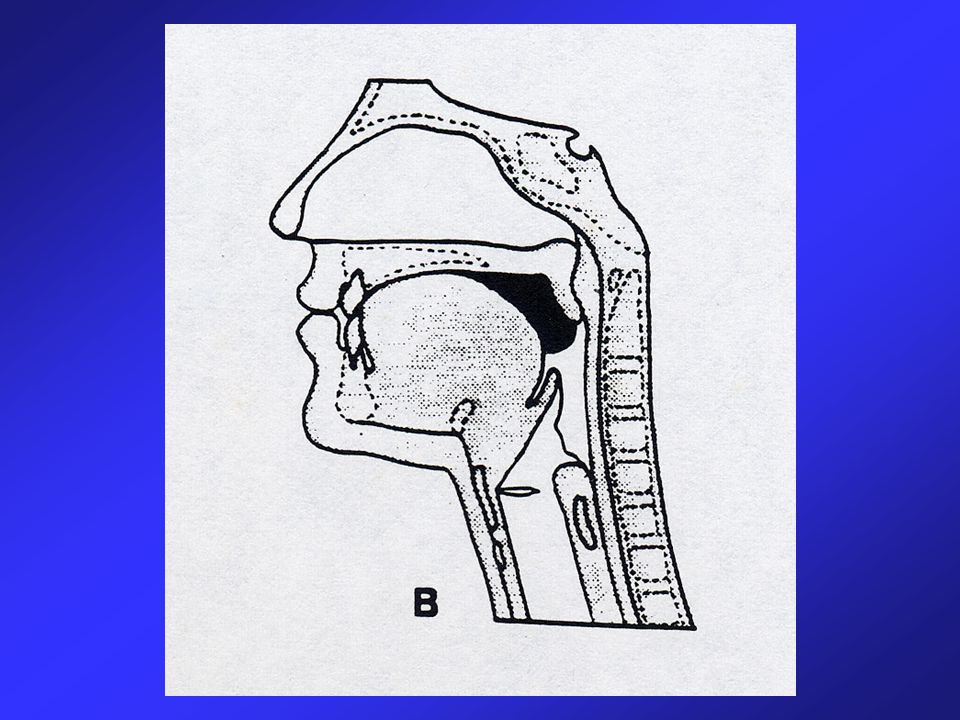
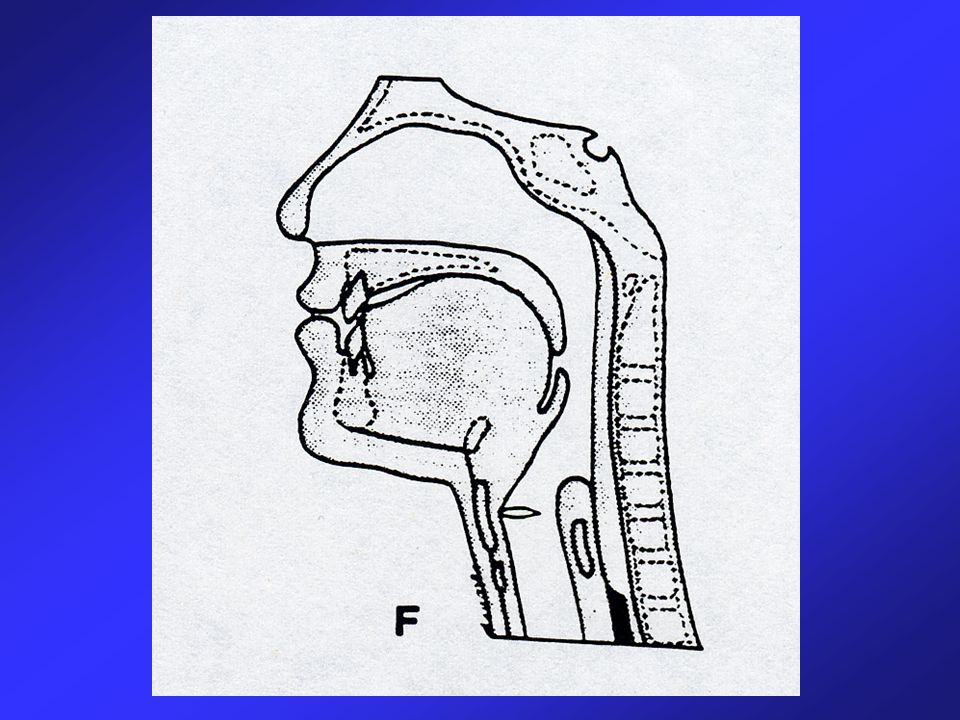
Five Stages of Eating FeedingFeeding Oral PreparatoryOral Preparatory Oral TransportOral Transport PharyngealPharyngeal EsophagealEsophageal

7
Definition: Feeding Voluntary movement of food from the environment into the oral cavity for the purpose of ingestion

8
Patient/Caregiver Reported Symptoms of Eating Abnormalities Self-Feeding: Easy distractibility, disinterest, drowsiness Easy distractibility, disinterest, drowsiness Rearranging, playing with food Rearranging, playing with food Attempts to ingest nonfood items Attempts to ingest nonfood items Incorrect utensil selection or use Incorrect utensil selection or use Inability to open containers or grasp utensils Inability to open containers or grasp utensils Dropping food enroute to oral cavity Dropping food enroute to oral cavity

9
Definition: Oral Preparatory Stage Voluntary mastication and preparation of food into a bolus

10
Definition: Oral Transport Stage Voluntary posterior movement of a bolus from the tip of the tongue to the anterior tonsillar pillars

11
Patient/Caregiver Reported Symptoms of Eating Abnormalities Oral Preparatory and Oral Transport Stages: Drooling or oral spillage Drooling or oral spillage Impaired chewing, munching Impaired chewing, munching Pocketing, holding of food in oral cavity Pocketing, holding of food in oral cavity Delayed or difficult initiation of swallow Delayed or difficult initiation of swallow Coughing and choking Coughing and choking

12
Definition: Pharyngeal Stage Reflexive passage of a bolus from the oral cavity into the upper esophagus

13
Patient/Caregiver Reported Symptoms of Eating Abnormalities Pharyngeal Stage: Nasal regurgitation Nasal regurgitation Aspiration Aspiration Wet or gurgly voice quality Wet or gurgly voice quality Coughing and choking Coughing and choking

14
Definition: Esophageal Stage Reflexive passage of a bolus from the cricopharyngeal sphincter past the lower esophageal sphincter into the stomach

15
Patient/Caregiver Reported Symptoms of Eating Abnormalities Esophageal Stage: Neck or chest pain Neck or chest pain Heart burn Heart burn Food sticking Food sticking Difficulty swallowing solids > liquids Difficulty swallowing solids > liquids Regurgitation Regurgitation

23
Etiology of Feeding & Swallowing Problems NeurologicalMechanicalPsychologicalCombination

24
Medication Related Swallowing Impairments

25
Identification/Evaluation of Feeding & Swallowing Problems Patient / caregiver observationsPatient / caregiver observations Clinical examinationClinical examination Instrumental evaluationInstrumental evaluation

26
Clinical Examination of Swallow Background informationBackground information –Active medical problems, therapies, nutrition/hydration status, overall health status, life expectancy Description of the problemDescription of the problem –Onset, duration, frequency, progression, speech Clinical observation/mental status examClinical observation/mental status exam –Speech, language, voice status, cognitive status Oral mucosa and dentitionOral mucosa and dentition Sensory motor exam of oro-facial structuresSensory motor exam of oro-facial structures Test swallow observationsTest swallow observations –Duration of oral stages, oral residue, cough, self feeding ability

27
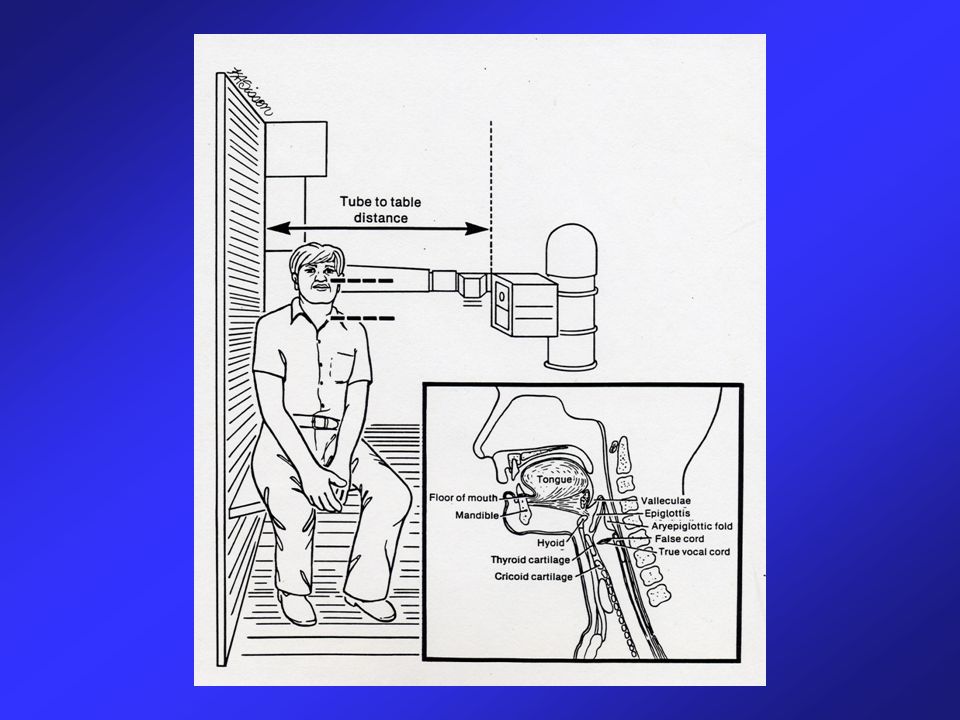
Instrumental Examination of Swallow Function Videoflurographic swallowing study (VSS)Videoflurographic swallowing study (VSS) –AKA: modified barium swallow, cookie swallow test –Considered to be the “gold standard” –Allows observation of outline of structures from oral cavity to stomach, this is a dynamic assessment Fiberoptic endoscopic evaluation of swallow (FEES)Fiberoptic endoscopic evaluation of swallow (FEES) –Allows direct observation of structures: nasal cavity, nasopharynx, oropharynx, larynx, hypopharynx
Videoflurographic swallowing study (VSS) –AKA: modified barium swallow, cookie swallow test –Considered to be the gold standard –Allows observation of outline of structures from oral cavity to stomach, this is a dynamic assessment Fiberoptic endoscopic evaluation of swallow (FEES)Fiberoptic endoscopic evaluation of swallow (FEES) –Allows direct observation of structures: nasal cavity, nasopharynx, oropharynx, larynx, hypopharynx")
32
Three Major Goals of Dysphagia Intervention 1. To maintain or improve nutrition and hydration. 1. To maintain or improve nutrition and hydration. 2. To prevent or reduce the risk of aspiration. 2. To prevent or reduce the risk of aspiration. 3. To maintain or restore the highest level of functional ability and maximize quality of life. 3. To maintain or restore the highest level of functional ability and maximize quality of life.

33
Nutritional Support Enteral vs. parenteral routes of administration Long-term vs. short-term use Complete nutritional replacement vs. partial support

34
Possible Benefits of Artificial Feeding Promotion of healing Improved resistance to infection Decreased skin breakdown Decreased aspiration Prolonged life Artificial feeding does not reverse or cure dysphagia

35
Possible Burdens of Artificial Feeding Tube placement Infection Need for restraints or immobility Increased aspiration Prolonged life

36
At lunchtime Mr. D is served a hotdog, bites off too large a piece, begins choking and subsequently dies of asphyxiation. Could this outcome have been avoided?Could this outcome have been avoided? How would you inform the family of his death?How would you inform the family of his death? What reaction from his family is anticipated?What reaction from his family is anticipated?

Similar presentations









 (MND) are a group of neurological disorders that selectively affect motor neurons.>")






 833-2090 www. med-speech.com.>")










