Download presentation
Presentation is loading. Please wait.

1
Tracheotomy/Tracheostomy Appendectomy
SUR 111 Tracheotomy/Tracheostomy Appendectomy

2
Tracheotomy Tracheostomy

3
Tracheotomy/Tracheostomy
Tracheotomy temporary opening into the trachea to facilitate breathing Tracheostomy permanent opening of the trachea and creation of a tracheal stoma Must place tracheal tube with either Patient will be hooked up to a ventilator Long term tracheostomy may eventually be able to wean off ventilator, but maintain stoma that will function as their nose did prior to surgery

4
Tracheostomy is indicated for a patient who requires emergent or elective airway management for:
prolonged ventilator dependence acute upper airway obstruction chronic upper airway obstruction

5
Pathology for Tracheotomy or Tracheostomy
Vocal cord paralysis Neck surgery Trauma Prolonged intubation Secretion management Cannot intubate Stridor due to tracheal blockage Sleep apnea Stridor - a high-pitched sound heard best on inspiration. Sleep apnea - A condition characterized by temporary breathing interruptions during sleep

6
Anatomy of the Neck The neck is traditionally organized into triangles; each side is divided into two large triangles separated by the sternocleidomastoid muscle. The neck has many significant structures, including The carotid artery The jugular vein The vagus nerve The recurrent laryngeal nerve The esophagus The trachea The spinal accessory nerve (cranial nerve XI) The digastric muscle The hypoglossal nerve (cranial nerve XII) The larynx The pharynx The thyroid The parathyroid The ansa cervicalis Lymph nodes (From Potter PA and Perry AG: Fundamentals of nursing, ed 5, St Louis, 2001, Mosby.)
 The digastric muscle. The hypoglossal nerve (cranial nerve XII) The larynx. The pharynx. The thyroid. The parathyroid. The ansa cervicalis. Lymph nodes. (From Potter PA and Perry AG: Fundamentals of nursing, ed 5, St Louis, 2001, Mosby.)")
7
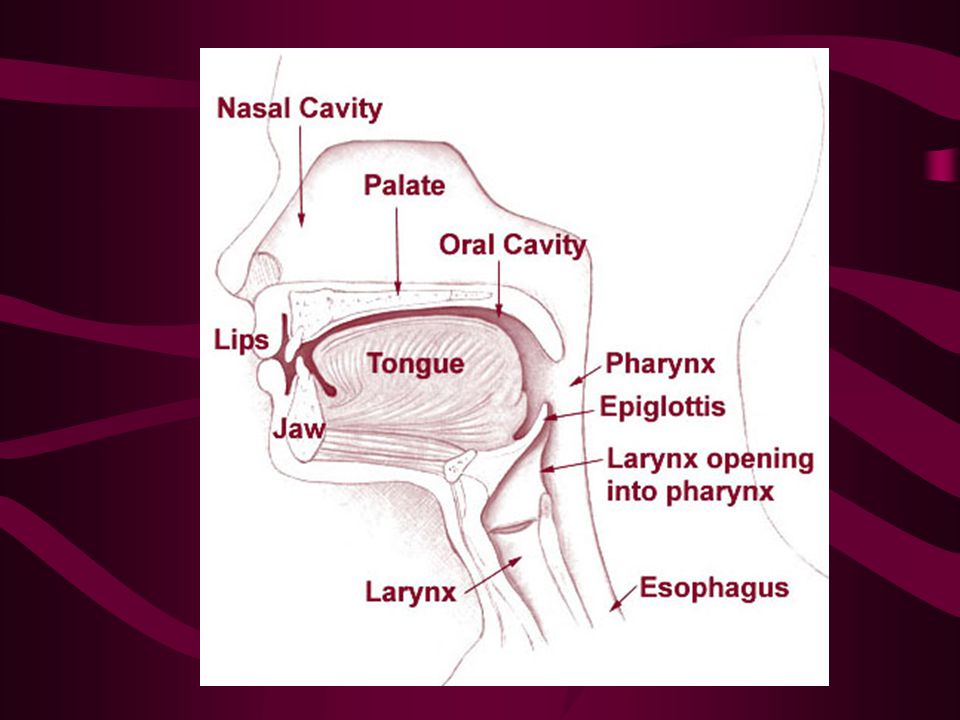
Anatomy of the Larynx Posterior view of the pharynx
The larynx is composed of nine segments of cartilage, three paired sets and three unpaired segments as illustrated in Figure 25–18. The hyoid bone - (Lingual Bone) is a bone in the human neck, and is the only bone in the skeleton not articulated to any other bone. It is supported by the muscles of the neck and in turn supports the root of the tongue. Posterior view of the pharynx Anterior view of the pharynx (From Thibodeau GA and Patton KT: Anthony's textbook of anatomy and physiology, ed 17, St Louis, 2003, Mosby.)
 is a bone in the human neck, and is the only bone in the skeleton not articulated to any other bone. It is supported by the muscles of the neck and in turn supports the root of the tongue. Posterior view of the pharynx. Anterior view of the pharynx. (From Thibodeau GA and Patton KT: Anthony s textbook of anatomy and physiology, ed 17, St Louis, 2003, Mosby.)")
9
Anesthesia General Local

10
Medications Local anesthetic: Lidocaine or bupivicaine with or without epinephrine Antibiotic irrigation

11
Positioning Supine Shoulder roll Donut headrest Pillow under knees
Safety strap

12
Prep End of chin to midchest and bedsheet to bedsheet
Prep of choice: Duraprep, betadine scrub and/or paint

13
Draping Towels Small fenestrated sheet (Pediatric lap sheet)
")
14
Supplies, Equipment, Instruments
Minor basin Basic pack Pediatric lap sheet Other small fenestrated sheet Blades Suture or ties of surgeon’s choice (prn) Tracheotomy tray Tracheotomy tube (Shiley) Twill tape
 Tracheotomy tray. Tracheotomy tube (Shiley) Twill tape.")
15
Isthmus of thyroid is divided to expose the trachea
Surgical Procedures Tracheotomy/Tracheostomy Tracheostomy is indicated for patient who require emergent or elective airway management of prolonged ventilator dependence or acute or chronic upper airway obstruction. Technique: An incision is made over the anterior tracheal wall. The surgeon visualizes the tracheal wall. The tracheal incision is made, usually between the third and fourth tracheal rings. The endotracheal tube is partially removed to the point superior to the tracheal incision. The tracheostomy tube is inserted. Hemostasis is achieved. Tracheostomy tube is secured. Dressings are applied. The obturator from the endotracheal tube is sent with the patient. Isthmus of thyroid is divided to expose the trachea Two tracheal rings are cut, and the upper ring is partially resected. Tracheal hook pulls the trachea from the depth of the wound toward the surface Tube is inserted (Modified from DeWeese DD: Textbook of otolaryngology, ed 6, St Louis, 1982, Mosby.)
")
16
Operative Sequence Discussion

17
Considerations Will make sure obturator goes with patient to PACU or ICU Complications: hemorrhage, infection, damage to other structures

18
Large Intestine (Colon) Anatomy
Look to page in ST

19
Sigmoid colon most frequent site of colon cancer
Sigmoid colon most frequent site of colon cancer. Are recesses or folds above the anus that can become clogged with feces and lead to fissures or fistulas Colon responsible for absorption of water and electrolytes, compaction of fecal waste, and production of Vitamin K Sigmoid colon 1° site of colon cancer

20
Becomes emergent procedure if ruptures
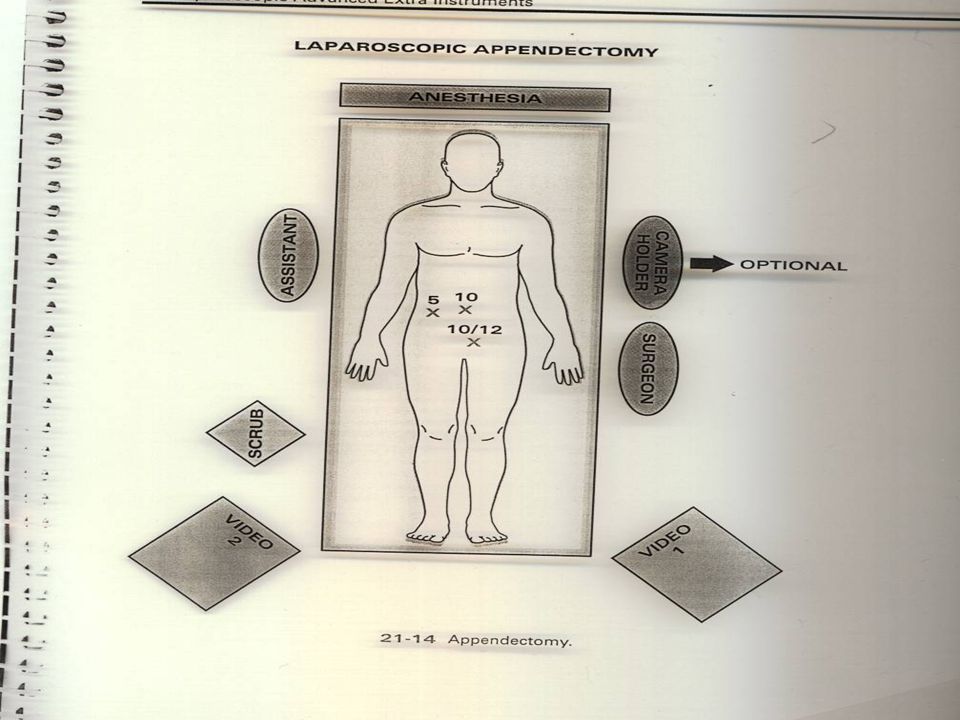
Appendectomy Removal of the appendix Appendicitis Inflammation/infection of the appendix Acute condition Urgent procedure Becomes emergent procedure if ruptures Rupture leads to peritonitis which untreated leads to death Sometimes Removed as Prophylactic Procedure (Incidental Appendectomy) in addition to other lower abdominal surgical procedures The appendix is removed when acutely infected to prevent peritonitis, which will occur if it should rupture. Many surgeons perform an appendectomy as a prophylactic (preventive) procedure when operating in the abdomen for other reasons. The procedure is then called an incidental appendectomy. Technique: The abdomen is entered. The appendix is isolated from the mesoappendix. The appendix is ligated and removed. A purse-string suture is placed around the stump of the appendix. The wound is closed. Isolation or bowel technique is used for this procedure.
 in addition to other lower abdominal surgical procedures. The appendix is removed when acutely infected to prevent peritonitis, which will occur if it should rupture. Many surgeons perform an appendectomy as a prophylactic (preventive) procedure when operating in the abdomen for other reasons. The procedure is then called an incidental appendectomy. Technique: The abdomen is entered. The appendix is isolated from the mesoappendix. The appendix is ligated and removed. A purse-string suture is placed around the stump of the appendix. The wound is closed. Isolation or bowel technique is used for this procedure.")
22
The base of the mesoappendix is coagulated using the endocoagulator
Laparoscopic Appendectomy The appendix is attached to the mesoappendix, which is divided with scissors or ESU and ligated with vessel clips or surgical stapler. Mesoappendix - (mes(o)- a prefix meaning in the middle) the peritoneal fold attaching the appendix to the mesentery of the ileum. The base of the mesoappendix is coagulated using the endocoagulator (From Goldberg JM and Falcone T: Atlas of endoscopic techniques in gynecology, Philadelphia, 2001, Saunders.)
- a prefix meaning in the middle) the peritoneal fold attaching the appendix to the mesentery of the ileum. The base of the mesoappendix is coagulated using the endocoagulator. (From Goldberg JM and Falcone T: Atlas of endoscopic techniques in gynecology, Philadelphia, 2001, Saunders.)")
23
The appendix is attached to the mesoappendix, which is divided with scissors or ESU and ligated with vessel clips or surgical stapler

24
The endo-loop is tightened at the base of the appendix
Laparoscopic Appendectomy, continued Once the appendix is mobilized, it can be amputated from the cecum. Two ties must be placed around the appendix between the lines of amputation. The endo-loop is tightened at the base of the appendix (From Goldberg JM and Falcone T: Atlas of endoscopic techniques in gynecology, Philadelphia, 2001, Saunders.)
")
25
Once the appendix is mobilized, it can be amputated from the cecum
Two ties must be placed around the appendix between the lines of amputation

26
The appendix is excised with scissors
Laparoscopic Appendectomy, continued The appendix is then transected with the ESU, scissors, or surgical stapler. The stapler provides additional security against leakage. The specimen is brought out of the abdomen with a specimen retrieval bag. The appendix is excised with scissors (From Goldberg JM and Falcone T: Atlas of endoscopic techniques in gynecology, Philadelphia, 2001, Saunders.)
")
27
The appendix is then transected with the ESU, scissors, or surgical stapler
The stapler provides additional security against leakage The specimen is brought out of the abdomen with a specimen retrieval bag

28
Loop technique: http://www. dailymotion
Stapler technique:

Similar presentations