Download presentation
Presentation is loading. Please wait.

1
Screening for Breast and Prostate Cancer: Who Should be Tested? Why the Controversy? Brandon P. Combs, MD GIM Grand Rounds 12 February 2013

2
OBJECTIVES Make sure we ask (and answer) the right questions Understand cancer screening basics Review epidemiology of breast and prostate cancer Understand risks and benefits of screening for breast and prostate cancer Examine origins of controversy and common perceptions vs reality Review current screening guidelines What should we tell our patients?
 the right questions Understand cancer screening basics Review epidemiology of breast and prostate cancer Understand risks and benefits of screening for breast and prostate cancer Examine origins of controversy and common perceptions vs reality Review current screening guidelines What should we tell our patients")
3
A THOUGHT EXPERIMENT… If there was a pill that, taken daily after age 50, would double your lifetime risk of getting cancer from 10% to 20% but could decrease your lifetime risk of dying from cancer by 20% (from 3% to 2.4%), would you take it?
, would you take it")
4
WHAT’S A SCREENING TEST? No symptoms allowed! Symptoms DIAGNOSTIC TESTING If you have symptoms you should get tested

5
OUTCOMES AND RISK Outcome – a health related event that people care about e.g. avoid death or suffering from disease Risk – chance of experiencing an outcome Risk reduction – difference in risk of some outcome as a result of a test or intervention (chance of benefit)
.")
6
LET’S APPLY THESE TERMS! A drug has been shown to reduce the risk of dying from heart disease from 2% to 1% over a 10 year period. Which of the following is true? A. Drug reduces risk by 50% B. Drug reduces risk by 1 percentage point C. 1 out of 100 people taking drug will avoid death from heart disease D. 99% of people taking drug get no benefit E. All of these are true

8
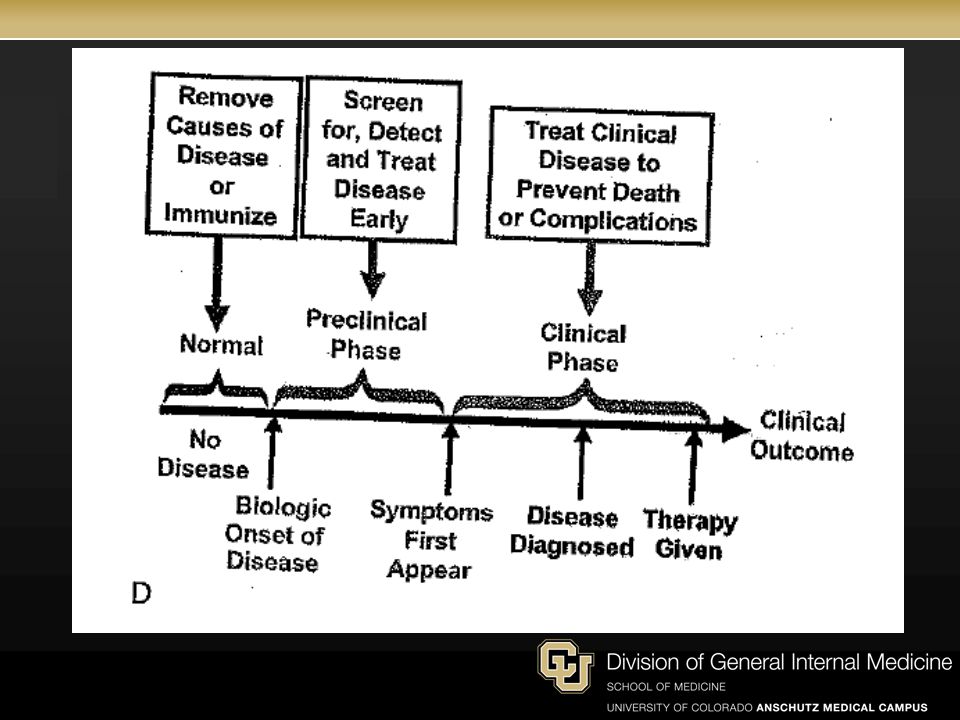
REQUIREMENTS OF A SUCCESSFUL SCREENING PROGRAM: 1. Screening advances time of diagnosis of cancers destined to cause death 2. Early treatment superior to treatment started after patient has symptoms

9
HOW IS BREAST AND PROSTATE CANCER INFLUENCED BY SCREENING? Esserman L, S.Y.T.I., REthinking screening for breast cancer and prostate cancer. JAMA: The Journal of the American Medical Association, 2009. 302(15): p. 1685- 1692. Microscopic Local Regional Advanced C ANCER P ROGRESSION Death
: p Microscopic Local Regional Advanced C ANCER P ROGRESSION Death.")
10
HOW IS BREAST AND PROSTATE CANCER INFLUENCED BY SCREENING? Esserman L, S.Y.T.I., REthinking screening for breast cancer and prostate cancer. JAMA: The Journal of the American Medical Association, 2009. 302(15): p. 1685- 1692. Microscopic Local Regional Advanced C ANCER P ROGRESSION Death Tumor D Tumor C Tumor B Tumor A
: p Microscopic Local Regional Advanced C ANCER P ROGRESSION Death Tumor D Tumor C Tumor B Tumor A.")
11
POTENTIAL IMPACT OF A SCREENING PROGRAM Esserman L, S.Y.T.I., REthinking screening for breast cancer and prostate cancer. JAMA: The Journal of the American Medical Association, 2009. 302(15): p. 1685- 1692. total cancer early advanced BEST CASEWORST CASEINTERMEDIATE Cancer Diagnosis
: p total cancer early advanced BEST CASEWORST CASEINTERMEDIATE Cancer Diagnosis.")
12
OVERDIAGNOSIS BIAS Wegwarth, O., et al., Do Physicians Understand Cancer Screening Statistics? A National Survey of Primary Care Physicians in the United States. Annals of Internal Medicine, 2012. 156(5): p. 340-349. Overdiagnosed
: p Overdiagnosed.")
13
LEAD-TIME BIAS Wegwarth, O., et al., Do Physicians Understand Cancer Screening Statistics? A National Survey of Primary Care Physicians in the United States. Annals of Internal Medicine, 2012. 156(5): p. 340-349.
: p")
14
TRUTHS ABOUT SCREENING Lead time – time by which diagnosis advanced by screening compared without screening Overdiagnosis – detection of a cancer by screening that was never going to cause symptoms in your lifetime DISREGARD SURVIVAL STATS IN SCREENING!

15
HOW COMMON IS PROSTATE CANCER? Chance that an average risk 50 year old man will be diagnosed with prostate cancer in his lifetime? A. 1% B. 10% C. 20% D. 50% E. 75% http://seer.cancer.gov/faststats/ Seidman H, Mushinski MH, Gelb SK, Silverberg E. Probabilities of eventually developing or dying of cancer—United States, 1985. CA Cancer J Clin. 1985;35(1):36-56
:")
16
WHAT’S THE RISK OF DYING FROM PROSTATE CANCER? Chance that an average risk 50 year old man will die of prostate cancer in his lifetime? A. 1% B. 3% C. 10% D. 25% E. 50% http://seer.cancer.gov/faststats/

17
TRENDS IN DIAGNOSIS AND DEATH FROM PROSTATE CANCER IN USA Notice large increase in diagnosis When did it start? How does this compare to decrease in mortality? Hoffman, R.M., Screening for Prostate Cancer. New England Journal of Medicine, 2011. 365(21): p. 2013-2019. Incidence per 100, 000
: p Incidence per 100, 000.")
18
HOW’S IT COMPARE TO THE UK? USA diagnosis UK diagnosis USA death UK death PSA Shibata A, Whittemore AS. Re: prostate cancer incidence and mortality in the United States and the United Kingdom. J Natl Cancer Inst 2001;93(14):1109-1110.
: .")
19
BREAST CANCER

20
HOW COMMON IS BREAST CANCER? Chance that an average risk 50 year old woman will be diagnosed with invasive breast cancer in her lifetime? A. 1% B. 10% C. 25% D. 50% E. 75% http://seer.cancer.gov/faststats/ Seidman H, Mushinski MH, Gelb SK, Silverberg E. Probabilities of eventually developing or dying of cancer—United States, 1985. CA Cancer J Clin. 1985;35(1):36-56
:")
21
WHAT’S THE RISK OF DYING FROM BREAST CANCER? Chance that an average risk 50 year old woman will die of breast cancer in her lifetime? A. 1% B. 3% C. 10% D. 25% E. 50% http://seer.cancer.gov/faststats/

22
TRENDS IN DIAGNOSIS OF BREAST CANCER IN USA Esserman L, S.Y.T.I., REthinking screening for breast cancer and prostate cancer. JAMA: The Journal of the American Medical Association, 2009. 302(15): p. 1685- 1692. ALL LOCAL METASTATIC REGIONAL Incidence per 100, 000
: p ALL LOCAL METASTATIC REGIONAL Incidence per 100, 000.")
23
WOMEN UNDER 40 (USA) Bleyer, A. and H.G. Welch, Effect of Three Decades of Screening Mammography on Breast-Cancer Incidence. New England Journal of Medicine, 2012. 367(21): p. 1998- 2005.
: p")
24
Sequential mammographic screening program introduction Similar declines in breast cancer mortality USA and Europe, independent of mammography Bleyer A BMJ 2011;343:bmj.d5630

25
QUICK REVIEW – TRUE OR FALSE? 1. Detecting more early cancer proves that cancer screening saves lives 2. Early detection of cancer can improve 5-year survival even if death isn’t postponed by screening 3. Getting a mammogram decreases your risk of getting breast cancer

26
A 50 YEAR OLD MAN’S RISK OF DYING OF PROSTATE CANCER IN NEXT 10 YRS WITHOUT SCREENING? (ASSUME AVERAGE RISK, NON-SMOKER) A. 0.2% B. 1% C. 5% D. 10% E. 25%
 A. 0.2% B. 1% C. 5% D. 10% E. 25%.")
27
A 50 YEAR OLD MAN’S RISK OF DYING OF PROSTATE CANCER IN NEXT 10 YRS WITH ANNUAL SCREENING? Answer: 0.1% Starting risk: 0.2% modified risk: 0.1% Percent of 50 y/o men who benefit from screening: 0.1% or 1/1000 Percent of 50 y/o men who do not benefit: 99.9% or 999/1000 Woloshin S, Schwartz LM, Welch G. The risk of death by age, sex, and smoking status in the United States: putting health risks in context. J Natl Cancer Inst. 2008;100:845–853. Medline. doi:10.1093/jnci/djn124 Schröder, F.H., et al., Prostate-Cancer Mortality at 11 Years of Follow-up. New England Journal of Medicine, 2012. 366(11): p. 981-990.
: p")
28
A 50 YEAR OLD WOMAN’S RISK OF DYING OF BREAST CANCER IN NEXT 10 YRS WITHOUT SCREENING? (ASSUME AVERAGE RISK, NON-SMOKER) A. 0.5% B. 1% C. 5% D. 10% E. 25%
 A. 0.5% B. 1% C. 5% D. 10% E. 25%.")
29
A 50 YEAR OLD WOMAN’S RISK OF DYING OF BREAST CANCER IN NEXT 10 YRS WITH ANNUAL SCREENING? (ASSUME AVERAGE RISK, NON-SMOKER) Answer: 0.4% Starting risk: 0.5% modified risk: 0.4% Percent of 50 yr old women who benefit from screening: 0.1% or 1/1000 Percent of 50 yr old women who do not benefit: 99.9% or 999/1000
 Answer: 0.4% Starting risk: 0.5% modified risk: 0.4% Percent of 50 yr old women who benefit from screening: 0.1% or 1/1000 Percent of 50 yr old women who do not benefit: 99.9% or 999/1000.")
30
ARE THESE RESULTS WHAT YOU EXPECTED?

31
PROSTATE CANCER – PERCEPTIONS AND REALITY Hoffman RM, Lewis CL, Pignone MP, Couper MP, Barry MJ, Elmore JG. et al. Decision-making processes for breast, colorectal, and prostate cancer screening: the DECISIONS survey.. Med Decis Making. 2010;3053S- 64S Lifetime risk of dying from prostate cancer: Perception Reality Lifetime risk of being diagnosed with prostate cancer: Perception Reality

32
BREAST CANCER – PERCEPTIONS AND REALITY Hoffman RM, Lewis CL, Pignone MP, Couper MP, Barry MJ, Elmore JG. et al. Decision-making processes for breast, colorectal, and prostate cancer screening: the DECISIONS survey.. Med Decis Making. 2010;3053S- 64S

33
PATIENTS OVERESTIMATE BENEFITS OF SCREENING Gigerenzer, G., J. Mata, and R. Frank, Public Knowledge of Benefits of Breast and Prostate Cancer Screening in Europe. Journal of the National Cancer Institute, 2009. 101(17): p. 1216-1220 “If screen 1000 women 40 yrs and older every other year for 10 yrs, how many fewer deaths from breast cancer?” “If screen 1000 men 50 yrs and older every other year for 10 yrs, how many fewer deaths from prostate cancer?”
: p If screen 1000 women 40 yrs and older every other year for 10 yrs, how many fewer deaths from breast cancer If screen 1000 men 50 yrs and older every other year for 10 yrs, how many fewer deaths from prostate cancer .")
34
UNWARRANTED CERTAINTY Patients overestimate risk & benefit 74% believed “finding cancer early saves lives most or all of the time” 40% felt that 80 y/o declining PSA or mammogram was “irresponsible” Hoffman RM, Lewis CL, Pignone MP, Couper MP, Barry MJ, Elmore JG. et al. Decision-making processes for breast, colorectal, and prostate cancer screening: the DECISIONS survey.. Med Decis Making. 2010;3053S-64S Schwartz LM, Woloshin S, Fowler FJ Jr, Welch HG. Enthusiasm for cancer screening in the United States.. JAMA. 2004;29171-8 Hudson, B., et al., Patients' Expectations of Screening and Preventive Treatments. The Annals of Family Medicine, 2012. 10(6): p. 495-502.
: p")
35
Placed much greater emphasis on survival statistics compared to mortality reduction One half incorrectly said that finding more cases of cancer in screened as opposed to unscreened populations “proves that screening saves lives.”

36
PERCEPTION AND REALITY 1. Exaggerated perception of the risk of getting and dying of cancer 2. Exaggerated perception of the benefits of screening What about the harms?

37
WHAT ARE THE HARMS FROM PSA SCREENING OVER 10 YRS ? false positive test: 10-12% unnecessary diagnosis and treatment (overdiagnosis): 1-3% erectile dysfunction or incontinence: 3% death: 0.03% Schroder F, Hugosson J, Roobol M, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med 2009;360(13):1320-1328. Andriole G, Grubb R III, Buys S, et al. Mortality results from a randomized prostate-cancer trial. N Engl J Med 2009;360(13):1310-1319. Moyer, V.A., Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine, 2012. 157(2): p. 120-134.
: 1-3% erectile dysfunction or incontinence: 3% death: 0.03% Schroder F, Hugosson J, Roobol M, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med 2009;360(13): Andriole G, Grubb R III, Buys S, et al. Mortality results from a randomized prostate-cancer trial. N Engl J Med 2009;360(13): Moyer, V.A., Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine, (2): p")
38
WHAT ARE THE HARMS FROM MAMMOGRAPHY SCREENING OVER 10 YRS ? false positive test requiring another mammogram or biopsy: 20-50% biopsy to rule out cancer: 5-20% unnecessary surgery, radiation, or chemo (overdiagnosis): 0.2 – 1.0% Woloshin, S. and L.M. Schwartz, How a charity oversells mammography. BMJ, 2012. 345 Woloshin, S. and L.M. Schwartz, Numbers Needed to Decide. Journal of the National Cancer Institute, 2009. 101(17): p. 1163-1165.
: 0.2 – 1.0% Woloshin, S. and L.M. Schwartz, How a charity oversells mammography. BMJ, Woloshin, S. and L.M. Schwartz, Numbers Needed to Decide. Journal of the National Cancer Institute, (17): p")
39
PERCEPTION AND REALITY 1. Exaggerated perception of the risk of getting and dying of cancer 2. Exaggerated perception of the benefits of screening 3. Harms often ignored Does public health messaging help?

40
ORIGINS OF CONTROVERSY “5 yr survival when caught early is 98%” “Get screened now”

41
FROM THE AMERICAN CANCER SOCIETY… 1970’S “Give yourself the chance of a lifetime”

42
FROM THE UNIVERSITY OF COLORADO… “The Pink Life Saver…aims to change that by bringing the often life-saving benefits of mammography to time-saving, convenient locations around the Denver area.” http://www.uch.edu/conditions/imaging-services/mammograms/pink-life-saver/

43
REGARDING PSA TESTS, FROM GENERAL COLIN POWELL… “Get checked. It could save your life…There are MORE CASES of prostate cancer than any other major cancer. Every THREE minutes an American man finds out he has prostate cancer. Nearly 30,000 men will die from prostate cancer this year.” http://www.prostateconditions.org/pcaw-media-kit

44
FROM ZEROCANCER.ORG “More than 115,000 men have been tested for free during the last 12 years, saving countless lives.”

45
CREDIBLE SOURCES OF INFORMATION Organizations that understand the distinction between potential benefit and actual benefit

46
Moyer, V.A., Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine, 2012. 157(2): p. 120-134. “The USPSTF recommends against PSA-based screening for prostate cancer” “It bases its recommendations on the evidence of both the benefits and harms of the service, and an assessment of the balance. The USPSTF does not consider the costs of providing a service in this assessment.”
: p The USPSTF recommends against PSA-based screening for prostate cancer It bases its recommendations on the evidence of both the benefits and harms of the service, and an assessment of the balance. The USPSTF does not consider the costs of providing a service in this assessment. .")
47
Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement. Annals of Internal Medicine, 2009. 151(10): p. 716-726. “The USPSTF recommends against routine screening mammography in women aged 40 to 49 years. The decision to start regular, biennial screening mammography before the age of 50 years should be an individual one and take patient context into account, including the patient's values regarding specific benefits and harms.” “The USPSTF recommends biennial screening mammography for women aged 50 to 74 years.”
: p The USPSTF recommends against routine screening mammography in women aged 40 to 49 years. The decision to start regular, biennial screening mammography before the age of 50 years should be an individual one and take patient context into account, including the patient s values regarding specific benefits and harms. The USPSTF recommends biennial screening mammography for women aged 50 to 74 years. .")
48
NATIONAL CANCER INSTITUTE “Screening for breast cancer does not affect overall mortality, and the absolute benefit for breast cancer mortality appears to be small.” http://www.cancer.gov/

49
NATIONAL CANCER INSTITUTE “Finding prostate cancer may not improve health or help a man live longer.” http://www.cancer.gov/

50
Probability Extreme Benefit The world of breast and prostate cancer screening in one graph Extreme Harm Minor HarmMinor Benefit

51
WHAT TO TELL YOUR PATIENTS If you are hearing a lot of certainty (e.g. ‘you need to get screened’) it’s time to start asking questions Healthy skepticism is a good thing There is no substitute for seeing harms and benefits side by side in absolute terms
 it’s time to start asking questions Healthy skepticism is a good thing There is no substitute for seeing harms and benefits side by side in absolute terms.")
52
WHAT’S THE “RIGHT” THING TO DO? There is no right or wrong answer – it’s a close call We should be experts on the medicine - Patients are expert on priorities Understand the risks and benefits Discussion should be evidence based, not fear based Promote informed, shared decisions

53
A THOUGHT EXPERIMENT… If you knew that routine PSA testing after age 50 would double your lifetime risk of getting prostate cancer from 10% to 20% but could decrease your lifetime risk of dying from prostate cancer by 20% (from 3% to 2.4%), would you be tested?
, would you be tested")
54
A THOUGHT EXPERIMENT… If you knew that getting routine mammograms after age 50 would double your lifetime risk of getting breast cancer from 8% to 15% but could decrease your lifetime risk of dying from breast cancer by 25% (from 3.6% to 2.7%), would you be tested?
, would you be tested")
55
THANK YOU! Special thanks to: Tanner Caverly, MD Dan Matlock, MD, MPH

Similar presentations



: Department.>")















