Download presentation
Presentation is loading. Please wait.

2
Gestational Trophoblastic Neoplasia (GTN) Zohreh Yousefi Professor of Obstetrics and Gynecology, Fellowship of Gynecology Oncology, Ghaem Hospital, website: www.zohrehyousefi.comwww.zohrehyousefi.com
 Zohreh Yousefi Professor of Obstetrics and Gynecology, Fellowship of Gynecology Oncology, Ghaem Hospital, website:")
3
Danforth's Williams Obstetrics, 23e B erek and Hacker's Gynecologic Oncology Up To Dat GESTATIONAL TROPHOBLASTIC DISEASE PATHOGENESIS DIAGNOSIS MANAGEMENT GESTATIONAL TROPHOBLASTIC NEOPLASIA TREATMENT SUBSEQUENT PREGNANCY

4
Gestational trophoblastic disease (GTD) is term group of tumors with abnormal trophoblast proliferation produce human chorionic gonadotropin (hCG)
 is term group of tumors with abnormal trophoblast proliferation produce human chorionic gonadotropin (hCG)")
5
GTD histologically is divided into benign hydatidiform moles ( complete and partial) Malignant Invasive mole
 Malignant Invasive mole")
6
Non -molar trophoblastic neoplasms Choriocarcinoma Placental site trophoblastic tumor Epithelioid trophoblastic tumor

7
Gestational trophoblastic neoplasia (GTN ) Malignant forms of gestational trophoblastic disease GT N is all GTD except hydatidiform mole Weeks or years following any type of pregnancy But frequently occur after a hydatidiform mole
 Malignant forms of gestational trophoblastic disease GT N is all GTD except hydatidiform mole Weeks or years following any type of pregnancy But frequently occur after a hydatidiform mole")
8
Hydatidiform mole Microscopic (classic findings) Absence embryonic elements Trophoblastic proliferation (cytotrophoblast and syncytiotrophoblast) Stromal edema and hydropic degeneration Absence of blood vessels
 Absence embryonic elements Trophoblastic proliferation (cytotrophoblast and syncytiotrophoblast) Stromal edema and hydropic degeneration Absence of blood vessels")
9
Macroscopic of Hydatidiform mole Hydropic villi Grapelike vesicles filled clear material usually 1 to 3cm diameter proliferation of the trophoblast

10
Hydatidiform mole Complete mole Partial mole Partial mole Partial mol ( fetal tissue) Grossly placenta a mixture of normal and hydropic villi Fetus Severe growth restriction Multiple congenital anomalies
 Grossly placenta a mixture of normal and hydropic villi Fetus Severe growth restriction Multiple congenital anomalies")
11
Risk Factors hydatidiform mole Strongest risk factors are Age and a history of prior hydatidiform mole Both extremes of reproductive age adolescents twofold risk Older than 40 tenfold risk

12
history of Prior mole the risk of another mole Complete mole is 1.5 percent Partial mole is 2.7 percent Two prior molar pregnancies the risk is 23 percent

13
An ethnic predisposition Diet (Deficiencies of protein or) (Vitamin A deficiency) animal fat Smoking Increased paternal age
 (Vitamin A deficiency) animal fat Smoking Increased paternal age")
14
Pathogenesis Abnormal fertilization process Normal ovum with a duplicated haploid sperm Inactive ovum chromosomes Karyotype 46, XX diploid and result from androgenesis Partial moles triploid karyotype 69, XXX, 69,XXY

16
Clinical Findings Because universal sonography in prenatal care Typically diagnosed at a mean of 10 weeks Vaginal bleeding spotting to profuse hemorrhage Moderate iron-deficiency anemia

17
Exaggerated early pregnancy symptoms Nausea and vomiting ( hyperemesis) Abdominal cramp
 Abdominal cramp")
18
Abnormally enlarged and soft uterus uterine growth Theca-lutein cysts (hCG) 25 to 60% (Torsion, infarction, rupture and hemorrhage) Releases antiangiogenic factors that activate endothelial damage Severe preeclampsia hypoxic trophoblastic mass
 25 to 60% (Torsion, infarction, rupture and hemorrhage) Releases antiangiogenic factors that activate endothelial damage Severe preeclampsia hypoxic trophoblastic mass")
19
All hydatidiform moles secrete hCG Thyrotrophic -like effects of hCG hCG acts a thyrotrophic substance Elevated serum free thyroxine (T 4 ) (TSH) levels to be decreased thyroid hyper –function “thyroid storm”
 (TSH) levels to be decreased thyroid hyper –function thyroid storm")
20
Diagnosis Amenorrhea followed by irregular bleeding Spontaneous passage of molar tissue High values Serum β-HCG measurement confirming the diagnosis IHC stain positively for p57

21
Sonography Echogenic uterine mass with anechoic cystic spaces without a fetus or amnionic sac The appearance as “snowstorm

22
Transvaginal sonogram demonstrating the “ snow storm” appearance.

23
Mis-diagnosis Incomplete abortion missed abortion Cystic degeneration uterine leiomyoma

24
which of the following symptoms will a highly intelligent physician assistant immediately consider hydatidiform mole? – pelvic pain at night during the first trimester – significantly elevated BP in the first trimester – significant bloody vaginal discharge in the first trimester – nausea and vomiting in the first trimester

25
Answer is B

26
Management Termination of Molar Pregnancy Evacuation and Curettage Hysterectomy (rarely and select cases no desired future pregnancy ) Chest radiograph Initiate effective contraception OCP or MPA } poor compliance}
 Chest radiograph Initiate effective contraception OCP or MPA } poor compliance}")
27
Serum hCG levels: 48 hours of evacuation (baseline) Weekly until undetectable Weekly until normal for 3 consecutive weeks monthly until normal for at least 6 consecutive months Median time for resolution is 9 weeks for complete 7 weeks for partial Hysterectomy reduces the incidence of malignant sequelae does not eliminate follow-up
 Weekly until undetectable Weekly until normal for 3 consecutive weeks monthly until normal for at least 6 consecutive months Median time for resolution is 9 weeks for complete 7 weeks for partial Hysterectomy reduces the incidence of malignant sequelae does not eliminate follow-up")
28
hCG change HM: 84-100 days Spontaneous abortion: 19 days Normal delivery: 12 days Ectopic pregnancy 8-9 days

29
After molar evacuation risk factors for malignant squeal 15 - 20 % complete moles 1 - 5 % partial moles 1 5% of HM become invasion moles 2.5% progress into choriocarcinoma

30
Twin Pregnancy (Normal Fetus and Coexistent Complete Mole) Diagnosis is difficult (early pregnancy ultrasound) A single partial molar pregnancy with abnormal fetus Distinguished
 Diagnosis is difficult (early pregnancy ultrasound) A single partial molar pregnancy with abnormal fetus Distinguished")
31
A few cases the diagnosis is not suspected until examination of the placenta following delivery

32
Amniocentesis ( fetal karyotype ) diploid or triploid If fetal karyotype is normal Major fetal malformations are excluded by ultrasound Chest X-ray performed Serum hCG values If there is no evidence of metastatic disease to allow the pregnancy
 diploid or triploid If fetal karyotype is normal Major fetal malformations are excluded by ultrasound Chest X-ray performed Serum hCG values If there is no evidence of metastatic disease to allow the pregnancy")
33
Possible risk for developing Subsequent GTN Preterm delivery Preeclampsia Sever hemorrhage

34
Persistent GTD : Persistently elevated serum hCG level Irregular vaginal bleeding Persistent theca lute in cysts (2 to 4 months regress spontaneously) Uterine sub involution Risk factors for GTN
 Uterine sub involution Risk factors for GTN")
35
Risk factors of GTN Older age β-hCG levels > 100,000 mIU/mL Large uterine size for-gestational age Theca-lutein cysts > 6 cm Earlier recognition and evacuation of molar pregnancies not lower risk neoplasia

36
Criteria for Diagnosis of Gestational Trophoblastic Neoplasia Criteria for the diagnosis of postmolar GTN 1. Plateau or rise of serum β-hCG level 2. Detectable serum β-hCG level for 6 months or more 3. Histological criteria for choriocarcinoma 4-Irregular bleeding,uterine sub involution

37
Plateau of serum β-hCG level (± 10 percent) for four easurements during a period of 3 weeks or longer days 1, 7, 14, 21 Rise of serum β-hCG level > 10 percent during three weekly consecutive, during a period of 2 weeks or more—days 1, 7, 14
 for four easurements during a period of 3 weeks or longer days 1, 7, 14, 21 Rise of serum β-hCG level > 10 percent during three weekly consecutive, during a period of 2 weeks or more—days 1, 7, 14")
38
Diagnosis Sonography Abdomino pelvic or trans vaginal sonography Radiograph of chest Chest CT scan Brain CT scan or MRI

39
SPESIAL 1-Selective angiography of abdominal and pelvic or hepatic (if indicated ) 2-Whole body PET Less commonly (occult disease ) 3-Stool guaiac tests If positive test is or if gastrointestinal symptoms be routinely performed in persistent GTN 4- complete radiographic evaluation of the gastrointestinal tract
 2-Whole body PET Less commonly (occult disease ) 3-Stool guaiac tests If positive test is or if gastrointestinal symptoms be routinely performed in persistent GTN 4- complete radiographic evaluation of the gastrointestinal tract")
40
GTN CLASSIFICATION Invasive Mole Almost all invasive moles arise from partial or complete moles Deep penetration into the myometrium or peritoneum Involvement of vaginal vault

41
Invasive hydatidiform mole infiltrating the myometrium

42
Choriocarcinoma Most common follow a term pregnancy or miscarriage Rapidly growing both myometrium and blood vessels Blood-borne metastases

43
differentiation between invasive mole and choriocarcinoma if we see villi, it must be invasion mole if we can’t see villi, it is choriocarcinoma

44
Common Sites for Metastatic Gestational Trophoblastic Tumors Site Per cent Lung60-95 Vagina40-50 Vulva/cervix10-15 Brain5-15 Liver5-15 Kidney0-5 Spleen0-5 Gastrointestinal0-5

45
Symptoms Metastatic symptoms Profuse vaginal bleeding Vaginal or cervical metastasis (bluish nodule in vaginal) Abdominal pain (intra-abdominal hemorrhage) Cough, hemoptysis Headache, nausea, vomit, paralysis or coma Urologic hemorrhage
 Abdominal pain (intra-abdominal hemorrhage) Cough, hemoptysis Headache, nausea, vomit, paralysis or coma Urologic hemorrhage")
46
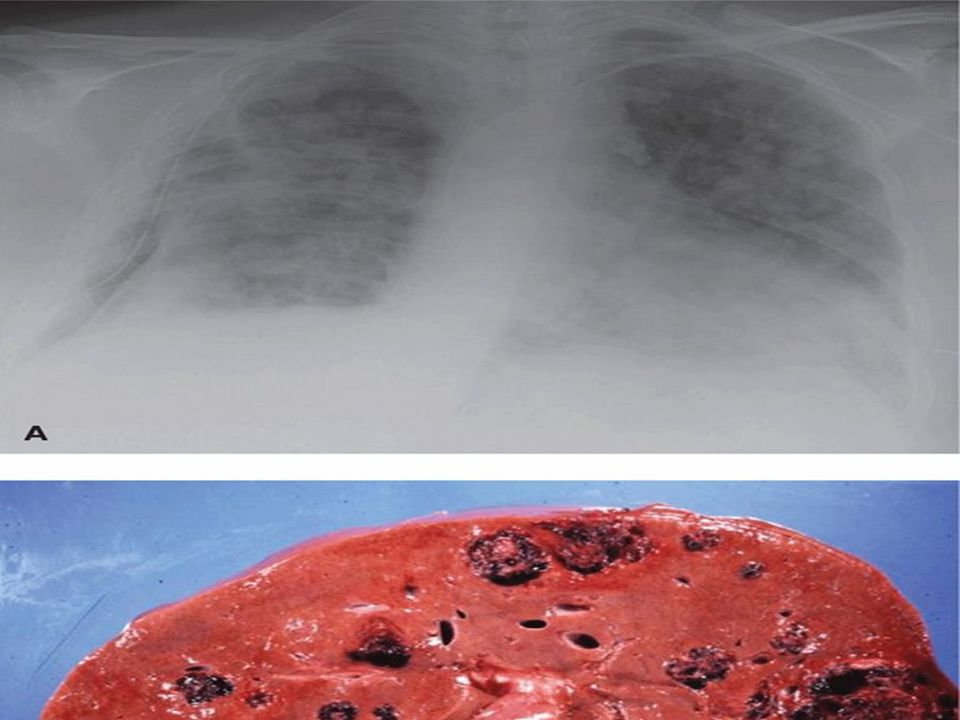
Lung metastasis Four principal pulmunary radiologic patterns: Snowstorm pattern (Alveolar pattern ) Discrete rounded densities Plural effusion Embolic pattern
 Discrete rounded densities Plural effusion Embolic pattern")
48
Brain metastasis Plasma CSF /hCG level ratio is normally >60: 1 In patients with CNS metastases <60: 1 Falsely lowered plasma CSF /hCG level First -trimester abortions In the absence of lung or vaginal metastasis Risk of cerebral and hepatic spread is exceedingly low

49
Generally in GTN Serum hCG levels combined Clinical findings Rather than a histological specimen Diagnose and treat this malignancy

50
Follow-up of GTN patients β-subunit until hCG Weekly until normal for 3 consecutive weeks monthly until normal for at least 3 consecutive months at 1-month interval for 1 year: at 1- month interval for 2 years in high stage at yearly interval for many years (increased risk of late recurrence)
")
51
Be careful : hCG Pelvic examination Chest X-ray unusual rise of serum hCG Rule out Normal pregnancy Ectopic pregnancy False-Positive hCG

52
False-Positive hCG: Quiescent GTN Phantom hCG Pituitary hCG Non-gynecologic tumors secreted -hCG

53
Quiescent GTN Constant, low level of hCG <100 IU/L Without evidence of a primary or metastatic malignancy Persisting for periods 3 months to 16 years Slow-growing Oral contraceptive pills and avoid pregnancy until hCG has been undetectable for six months 20 percent will eventually have recurrent active H –hCG assay is critical

54
H CG variants Hyperglycosylated hCG (H -hCG) hCG produced by syncytiotrophoblasts (H -hCG) synthesized by cytotrophoblast (H -hCG) absolute marker of ongoing invasion hCG-H is detectable >1 ng/ml: active GTN To discriminate quiescent disease
 hCG produced by syncytiotrophoblasts (H -hCG) synthesized by cytotrophoblast (H -hCG) absolute marker of ongoing invasion hCG-H is detectable >1 ng/ml: active GTN To discriminate quiescent disease")
55
Phantom hCG False positive serum hCG Send the serum to two laboratories Using different commercial assays If negative in one or both false positive hCG Presence of hCG in serum but not urine

56
Heterothallic antibodies may results false-positive False positive are at risk for recurrent Risk for other false positives, such as CA-125 and thyroid antibodies

57
Pituitary hCG Secreted LH and hCG pulsatile and paralleled Higher levels of h CG in postmenopausal than premenopausal Cross-reactivity with LH Pituitary production hCG ranges from 1 to 32 mIU/mL HRT or BSO or OCP after 2–3 weeks Suppress hCG Pituitary production

58
Staging of GTN WHO Scoring System

59
Staging International staging of WHO may be summarized as follows: Ⅰ : lesion localized in uterus, no metastasis; Ⅱ : lesion extends beyond uterus, but still confined to internal genitalias; Ⅲ : pulmonary lesion Ⅳ : metastasis to other distant sites.

61
IIb IIa

62
IIIa<3cm or locate in half lung IIIb disease beyond IIIa

64
Who Orgnaization prognostic scoring system for gestational trophoblastic neoplasia Prognostic factor0124 Age<39>39_- Antecedent pregnancyHydatidiformAbortion, ectipicTerm pregnancy- Interval (months)<44-67-12>12 hCG level (IU/liter)<1010-10 >10 ABO blood groups (female/male) O/ABA/OAB Largest tumor (cm)<33-5>5_ Site of metastasis_Spleen, kidneyGastrointestinal tract, liverBrain Number of metastases_1-34-8>8 Prior chemotherapy__Single drugMultiple drugs The total score is obtained by adding the individual scores for each prognostic factor. Total score : 8, high risk. Interval :between antecedent pregnancy and start of chemotherapy.

65
According to the FIGO staging of gestational trophoblastic tumors a lady with choriocarcinoma having lung metastasis will belong to which stage

66
protocol for treatment of GTD Clinically staging( FIGO) WHO scoring Again, it is stressed that the diagnosis of GTN made by persistently elevated serum β-hCG without confirmation by pathological tissue study
 WHO scoring Again, it is stressed that the diagnosis of GTN made by persistently elevated serum β-hCG without confirmation by pathological tissue study")
67
Choice of treatment Chemotherapy ( highly sensitive ) Surgery ( unresponsive or drug fails ) Irradiation (brain and liver )
 Surgery ( unresponsive or drug fails ) Irradiation (brain and liver )")
68
Chemotherapy are best management Protocols: Single-agent for low-risk Methotrexate Combination for high-risk disease EMA-CO Early-stage GTN is typically cured Later -stage disease usually responds to chemotherapy

69
Surgery in malignant GTN Hysterectomy Laparoscopy Craniotomy (brain hemorrhage) Thoracotomy (solitary nodules in drug-resistant disease ) selective resection of lesion in uterus or liver
 Thoracotomy (solitary nodules in drug-resistant disease ) selective resection of lesion in uterus or liver")
70
Main causes of death: Hemorrhage Infection Metastasis

71
Placental Site Trophoblastic Tumor (PSST) PSTT or non-trophoblastic malignancy Uncommon tumor arises from implantation site- intermediate trophoblast Secrete (hPL) from intermediate cells Relatively small amounts of hCG hCG free β-subunit is more than one third of hCG (30%)
 PSTT or non-trophoblastic malignancy Uncommon tumor arises from implantation site- intermediate trophoblast Secrete (hPL) from intermediate cells Relatively small amounts of hCG hCG free β-subunit is more than one third of hCG (30%)")
72
Typically local myometrial invasion Rare systemic metastases Treatment of ( PSST) is preferred hysterectomy Because resistant to chemotherapy For higher-risk than stage I combination chemotherapy given
 is preferred hysterectomy Because resistant to chemotherapy For higher-risk than stage I combination chemotherapy given")
73
Epithelioid Trophoblastic Tumor This rare tumor Intermediate trophoblast -type Grossly a nodular fashion Primary treatment is hysterectomy Relatively resistant to chemotherapy Approximately a fourth this neoplasm will have metastatic disease, combination chemotherapy

74
SUBSEQUENT PREGNANCY Pregnancy outcomes are usually normal May develop: 1-Repeat molar gestation 2-percent 2-Spontaneous abortions 3-Congenital anomalies 4-Ovarian failure (chemotherapy) 5-Secondary tumors including leukemia colon cancer, melanoma and breast cancer
 5-Secondary tumors including leukemia colon cancer, melanoma and breast cancer")
76
After Termination of Subsequent Pregnancy Sonographic evaluation in early pregnancy pathological evaluation placenta after delivery serum β-hCG level is measured 6 weeks postpartum

77
Conclusion The possibility of metastatic GTN should be considered In any woman of the reproductive age Presenting with metastatic disease Or an unknown primary site of malignancy

78
www.zohrehyousefi.com

Similar presentations





 for FIGO prognostic score and UAPI for prediction of MTX-R (ROC curves have been.>")


>")












 Dr. Yousefi. Z.>")


 dr yousefi Gynecologist oncologist of Medical Sciences of Mashhad University.>")