Download presentation
Presentation is loading. Please wait.

1
Stephanie M Chu, DO Assistant Professor University of Colorado SOM Team Physician Colorado Buffaloes

2
Review ankle anatomy Clinical examination Ankle sprains Treatment options

3
Articular Ligamentous Functional

4
Articular congruity Between talus and tibia, talus and calcaneus Ligamentous stability Tib-fib ligament (Syndesmotic ligament) Lateral ligament complex Deltoid ligament Subtalar ligaments Articular congruity Between talus and tibia, talus and calcaneus Ligamentous stability Tib-fib ligament (Syndesmotic ligament) Lateral ligament complex Deltoid ligament Subtalar ligaments
 Lateral ligament complex Deltoid ligament Subtalar ligaments Articular congruity Between talus and tibia, talus and calcaneus Ligamentous stability Tib-fib ligament (Syndesmotic ligament) Lateral ligament complex Deltoid ligament Subtalar ligaments")
5
Tibia Fibula Talus Navicular Calcaneus Base of 5 th Metatarsal

7
ATFL Arises from anterior border of tip of fibula and inserts on the neck of talus Parallel to axis of foot in neutral position Parallel to axis of tibia in plantarflexion ATFL Arises from anterior border of tip of fibula and inserts on the neck of talus Parallel to axis of foot in neutral position Parallel to axis of tibia in plantarflexion DeLee & Drez

10
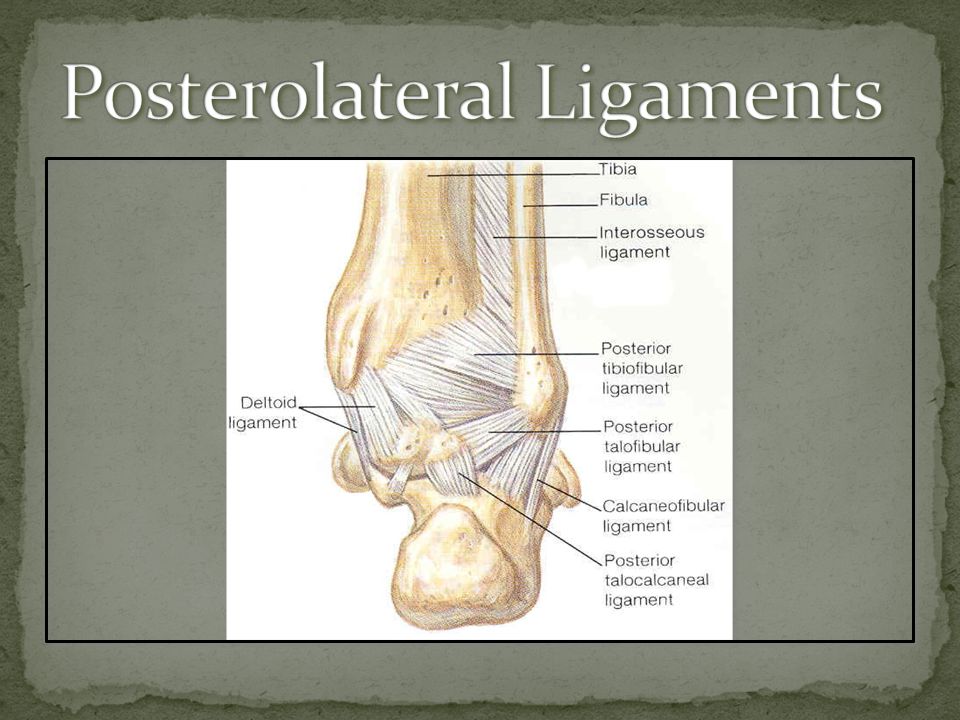
PTFL Arises from posterior tip of fibula and inserts on posterior process of talus ATFL & PTFL Resist AP motion of the talus relative to the fibula PTFL Arises from posterior tip of fibula and inserts on posterior process of talus ATFL & PTFL Resist AP motion of the talus relative to the fibula DeLee & Drez

11
CFL Arises from tip of fibula and inserts on lateral calcaneus Forms the floor of the peroneal tendon sheath Resists inversion CFL Arises from tip of fibula and inserts on lateral calcaneus Forms the floor of the peroneal tendon sheath Resists inversion DeLee & Drez

12
Normal ROM highly variable DF ranges from 10-50 degrees PF ranges from 15-60 degrees Functional ROM from 10 deg DF to 50 deg PF Normal ROM highly variable DF ranges from 10-50 degrees PF ranges from 15-60 degrees Functional ROM from 10 deg DF to 50 deg PF

13
Subtalar motion Supination – combination of inversion, adduction, internal rotation Pronation – combination of eversion, abduction, external rotation Subtalar motion Supination – combination of inversion, adduction, internal rotation Pronation – combination of eversion, abduction, external rotation

14
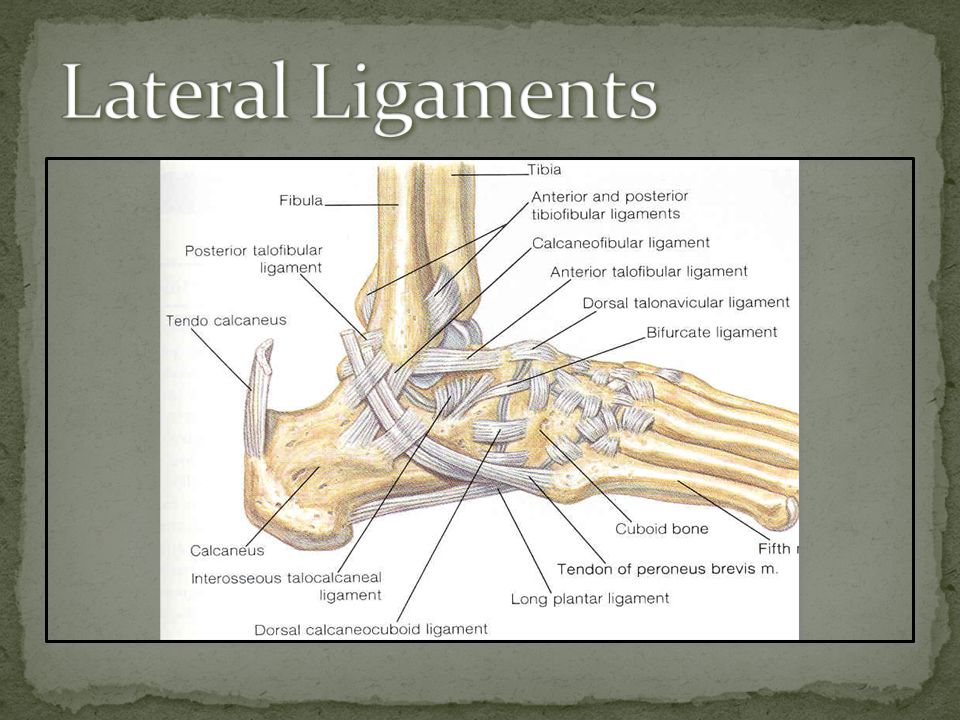
Lateral ligamentous complex Anterior talofibular ligament (ATFL) Calcaneofibular ligament (CFL) Posterior talofibular ligament (PTFL) Ligaments continuous with capsular connective tissue Lateral ligamentous complex Anterior talofibular ligament (ATFL) Calcaneofibular ligament (CFL) Posterior talofibular ligament (PTFL) Ligaments continuous with capsular connective tissue
 Calcaneofibular ligament (CFL) Posterior talofibular ligament (PTFL) Ligaments continuous with capsular connective tissue Lateral ligamentous complex Anterior talofibular ligament (ATFL) Calcaneofibular ligament (CFL) Posterior talofibular ligament (PTFL) Ligaments continuous with capsular connective tissue")
16
Description of injury Position of foot Direction of force Previous h/o ankle sprain Resolution of symptoms Chronic laxity or instability Use of tape/braces Description of injury Position of foot Direction of force Previous h/o ankle sprain Resolution of symptoms Chronic laxity or instability Use of tape/braces Previous treatment Ability to bear weight Symptoms Onset of pain Location Duration of pain Feeling of “giving way” Previous treatment Ability to bear weight Symptoms Onset of pain Location Duration of pain Feeling of “giving way”

18
Most common injury in sports – 25% Estimated 1 inversion injury/10,000 persons/day Most frequent in basketball, volleyball, soccer, football Majority < 35yrs Most often between ages 15-19 Certain populations (US military service personnel) as high as 35% Most common injury in sports – 25% Estimated 1 inversion injury/10,000 persons/day Most frequent in basketball, volleyball, soccer, football Majority < 35yrs Most often between ages 15-19 Certain populations (US military service personnel) as high as 35% Definition “Ankle injury that occurs when a person stumbles and the supporting foot twists, resulting in damage to the ligaments.” Definition “Ankle injury that occurs when a person stumbles and the supporting foot twists, resulting in damage to the ligaments.”
 as high as 35% Most common injury in sports – 25% Estimated 1 inversion injury/10,000 persons/day Most frequent in basketball, volleyball, soccer, football Majority < 35yrs Most often between ages Certain populations (US military service personnel) as high as 35% Definition Ankle injury that occurs when a person stumbles and the supporting foot twists, resulting in damage to the ligaments. Definition Ankle injury that occurs when a person stumbles and the supporting foot twists, resulting in damage to the ligaments.")
20
Most common – “inversion sprain” Combination of inversion and adduction of foot in plantar flexion Damage to lateral ligament complex of ankle Eversion sprains Damage to deltoid ligament ‘High’ ankle sprain Damage to ankle syndesmosis and tibiofibular ligaments

21
Grade I (mild) Mild ligament stretching No macroscopic tearing Stable Min tenderness or swelling Min functional loss Grade I (mild) Mild ligament stretching No macroscopic tearing Stable Min tenderness or swelling Min functional loss
 Mild ligament stretching No macroscopic tearing Stable Min tenderness or swelling Min functional loss Grade I (mild) Mild ligament stretching No macroscopic tearing Stable Min tenderness or swelling Min functional loss")
22
Grade II (moderate) Partial macroscopic tearing Moderate tenderness or swelling Mild to moderate instability Grade II (moderate) Partial macroscopic tearing Moderate tenderness or swelling Mild to moderate instability
 Partial macroscopic tearing Moderate tenderness or swelling Mild to moderate instability Grade II (moderate) Partial macroscopic tearing Moderate tenderness or swelling Mild to moderate instability")
23
Grade III (severe) Complete rupture of ligaments Marked pain, swelling, ecchymosis Abnormal joint motion (instability) Decreased function Soft or no “ end point ” Grade III (severe) Complete rupture of ligaments Marked pain, swelling, ecchymosis Abnormal joint motion (instability) Decreased function Soft or no “ end point ” Clinically, grading can be subjective, especially in acute setting without radiologic modalities (diagnostic ultrasound or MRI) to confirm.
 Complete rupture of ligaments Marked pain, swelling, ecchymosis Abnormal joint motion (instability) Decreased function Soft or no end point Grade III (severe) Complete rupture of ligaments Marked pain, swelling, ecchymosis Abnormal joint motion (instability) Decreased function Soft or no end point Clinically, grading can be subjective, especially in acute setting without radiologic modalities (diagnostic ultrasound or MRI) to confirm.")
24
Physical Examination Observation Location of ecchymosis, swelling Palpation Point of maximal tenderness Medial pain – may be indicative of concussive injury to deltoid ligament Tenderness over fibula or talus may indicate fracture Associated injuries to midfoot, 5 th metatarsal, prox fibula Physical Examination Observation Location of ecchymosis, swelling Palpation Point of maximal tenderness Medial pain – may be indicative of concussive injury to deltoid ligament Tenderness over fibula or talus may indicate fracture Associated injuries to midfoot, 5 th metatarsal, prox fibula

25
Physical Examination (compare to uninjured ankle) ROM Stability testing Anterior drawer (ATFL) Talar tilt (CFL, ATFL) Syndesmosis External rotation test Squeeze test Physical Examination (compare to uninjured ankle) ROM Stability testing Anterior drawer (ATFL) Talar tilt (CFL, ATFL) Syndesmosis External rotation test Squeeze test
 ROM Stability testing Anterior drawer (ATFL) Talar tilt (CFL, ATFL) Syndesmosis External rotation test Squeeze test Physical Examination (compare to uninjured ankle) ROM Stability testing Anterior drawer (ATFL) Talar tilt (CFL, ATFL) Syndesmosis External rotation test Squeeze test")
26
Plain radiographs Standard AP/lat/mortise views Stress radiographs Ant drawer & talar tilt thought to be inadequate predictors of functional stability Can be useful for syndesmotic injuries Arthrography Rarely used Plain radiographs Standard AP/lat/mortise views Stress radiographs Ant drawer & talar tilt thought to be inadequate predictors of functional stability Can be useful for syndesmotic injuries Arthrography Rarely used

27
Ankle Fractures Sensitivity = 98-100% Specificity = 31%

28
Ankle = Pain around the malleoli and ONE of the following: Inability to bear weight immediately following injury AND in ED (four steps) Bone tenderness 6 centimeters up posterior edge of the tibia and fibula
 Bone tenderness 6 centimeters up posterior edge of the tibia and fibula")
29
Bone scan May have a role in syndesmotic injuries CT scan Useful for evaluation of OCD lesions, loose bodies, syndesmotic widening MRI Useful for determining soft tissue injury, OCD, associated tendon injures Bone scan May have a role in syndesmotic injuries CT scan Useful for evaluation of OCD lesions, loose bodies, syndesmotic widening MRI Useful for determining soft tissue injury, OCD, associated tendon injures

31
Acute ankle sprains Grade I and II Functional rehab Includes brief period of immobilization (taping, functional braces statistically better than immobilization) Lace-up supports more effective than tape Early ROM, followed by strengthening and proprioceptive exercises Acute ankle sprains Grade I and II Functional rehab Includes brief period of immobilization (taping, functional braces statistically better than immobilization) Lace-up supports more effective than tape Early ROM, followed by strengthening and proprioceptive exercises Seah, Richard, and Sivanadian Mani-Babu. "Managing ankle sprains in primary care: what is best practice? A systematic review of the last 10 years of evidence." British medical bulletin 97.1 (2011): 105-135.
:")
32
Grade III Somewhat controversial Evidence suggest semi-rigid orthoses and pneumatic bracing provide beneficial ankle support to prevent recurrent sprains Numerous studies have shown that functional rehab results similar to surgical outcomes Grade III Somewhat controversial Evidence suggest semi-rigid orthoses and pneumatic bracing provide beneficial ankle support to prevent recurrent sprains Numerous studies have shown that functional rehab results similar to surgical outcomes

33
Chronic ankle sprains Functional rehabilitation Role in recovery May attempt for as long as 6 months Studies have shown that delayed functional rehab can still be successful Chronic ankle sprains Functional rehabilitation Role in recovery May attempt for as long as 6 months Studies have shown that delayed functional rehab can still be successful

35
Previous history of ankle sprain Ligament hyperlaxity Poor sensorimotor control Axial/foot alignment Plantar/dorsiflexion strength Inversion/Eversion strength Gender/sport No significant difference Previous history of ankle sprain Ligament hyperlaxity Poor sensorimotor control Axial/foot alignment Plantar/dorsiflexion strength Inversion/Eversion strength Gender/sport No significant difference

36
Taping Shown to be effective for initial stabilization Aids in proprioception Braces Shown to be effective in athletes with h/o previous sprains Prophylactic proprioceptive training More effective in athletes with h/o previous sprains Taping Shown to be effective for initial stabilization Aids in proprioception Braces Shown to be effective in athletes with h/o previous sprains Prophylactic proprioceptive training More effective in athletes with h/o previous sprains

Similar presentations










>")



 Radiographic Evaluation of the Ankle>")











