Download presentation
Presentation is loading. Please wait.

1
Leads, Leads and More Leads….
The question is.. where does this all “lead” us? Silver Cross EMS Continuing Education 1st Trimester January 2013 By Laurie Carroll, RN, Adventist Bolingbrook Hospital Silver Cross EMS Education Staff.

2
Our Agenda Today System announcements Cardiac anatomy and physiology
EKG review (ALS) 12-lead review (ALS) Mini-CME: Autism
 12-lead review (ALS) Mini-CME: Autism.")
3
Silver Cross EMSS announcements
New 1st Quarter Region 7 QA – 12 lead use. Consider 12-leads for: Chest/arm/jaw/back pain (non-trauma) Unexplained diaphoresis Vomiting w/o fever or diarrhea SOB/dizzy/syncope/weakness/fatigue Epigastric pain (non-trauma) Unexplained fall in elderly Unexplained brady/tachy And document your decision to use/not use
 Unexplained diaphoresis. Vomiting w/o fever or diarrhea. SOB/dizzy/syncope/weakness/fatigue. Epigastric pain (non-trauma) Unexplained fall in elderly. Unexplained brady/tachy. And document your decision to use/not use.")
4
Cardiac Anatomy Review

5
The Heart Four chambers Hollow Muscular Dual Circulation
feeds the heart muscle itself circulates blood outside the heart lungs for oxygenation and CO2 offload peripheral supply to tissues, organs and organ systems

6
Right Heart Receives unoxygenated blood from Blood passes from
systemic circulation vena cavae coronary circulation coronary sinus Blood passes from right atrium through tricuspid valve right ventricle pulmonic valve pulmonary artery to lungs

7
Left Heart Receives oxygenated blood from pulmonary vein
Blood passes from left atrium mitral valve left ventricle aortic valve aorta

8
Aorta Oxygenated blood in the aortic root enters the coronary arteries
Most myocardial blood supply occurs during diastole the aortic valve leaflets are closed and do not obstruct the coronary artery roots the subendocardial blood vessels are not compressed (as they are during systole) allowing blood to flow into the myocardium itself in the normal cardiac cycle, diastole is longer than systole
 allowing blood to flow into the myocardium itself. in the normal cardiac cycle, diastole is longer than systole.")
10
Coronary Artery Disease
Any narrowing of the coronary arteries causes diminished blood supply restriction of delivery of electrolytes and nutrients

11
to help us understand which areas of the heart are affected
Who Supplies What? It is often helpful to understand where the supply of blood is coming from, to help us understand which areas of the heart are affected by various strictures/occlusions.

12
LCA Left Left main divides into two branches
Left Anterior Descending (LAD) Anterior wall of LV RBB and portions of LBB Associated with Anterior Wall MI Circumflex (Cx) Lateral and Posterior walls of LV Left atrium SA node in ~ 30% Associated with Lateral Wall MI
 Anterior wall of LV. RBB and portions of LBB. Associated with Anterior Wall MI. Circumflex (Cx) Lateral and Posterior walls of LV. Left atrium. SA node in ~ 30% Associated with Lateral Wall MI.")
13
RCA Right Right Atrium (RA) Right Ventricle (RV)
Inferior and Posterior LV SA node in ~60% AV node Associated with right ventricular MI or dysrhythmias affecting SA and AV nodes

14
Area of Injury Infarct = dead or necrosis Blockage = causes ischemia

15
Collateral Circulation
If coronary artery disease and stenosis develop slowly, collateral circulation can develop When the stenosis is acute, collateral circulation does not have time to develop

17
Cardiac Rhythm Disturbances
CO (cardiac output) = HR (heart rate) x SV (stroke volume) Rhythm disturbances can hamper delivery of blood to the myocardium
 = HR (heart rate) x SV (stroke volume) Rhythm disturbances can hamper delivery of blood to the myocardium.")
18
Normal ECG Review P wave P-R Interval QRS S-T Segment T wave
Smooth, rounded, upright P-R Interval seconds QRS Symmetrical < .10 seconds S-T Segment Isoelectric T wave Upright, rounded

19
Where do the stickies go, and why?
Hook ‘em up: Where do the stickies go, and why? A lead is a record of electrical activity between two electrodes. Each lead records the average current flow at a specific time in a portion of the heart. Skin preparation: dry, hair-free Placing the electrode. Be sure that the electrode has adequate gel and is not dry.

20
Trouble shooting EKG Clarity
Equipment Grounded? Cables attached? Patient in reclining or semi fowler position? Patient sitting still? Skin clean and dry? Limb leads in place or reversed?

21
There are three kinds of leads:
Standard Limb Leads Augmented Leads Precordial Leads

22
(Remember: “lead” may refer to a direction, or placement.)
Standard Limb Leads (Remember: “lead” may refer to a direction, or placement.) Lead I: The positive lead is above the left breast or on the left arm and the negative lead is on the right arm. Records the difference of potential between the Left arm and Right arm. Lead II: The postive lead is on the left abdomen or left thigh and the negative lead is also on the right arm. Records the difference of potential between the left leg and the right arm. Lead III: The postive lead is also on the left abdomen or left lower lateral leg but the negative lead is on the left arm. Records the difference of potential between the left leg and the right arm.
 Lead I: The positive lead is above the left breast or on the left arm and the negative lead is on the right arm. Records the difference of potential between the Left arm and Right arm. Lead II: The postive lead is on the left abdomen or left thigh and the negative lead is also on the right arm. Records the difference of potential between the left leg and the right arm. Lead III: The postive lead is also on the left abdomen or left lower lateral leg but the negative lead is on the left arm. Records the difference of potential between the left leg and the right arm.")
23
Augmented Leads The four limb leads go on the four extremities as follows: The upper extremities need placement of the electrodes on the area of the lateral humoral aspect of the arms. The lower extremities need placement of the electrodes on the lateral lower legs near the lateral mallelous. Lead aVR faces the heart from the right shoulder and is oriented to the cavity of the heart. Lead aVL faces the heart from the left shoulder and is oriented to the Left Ventricle. Lead aVF face the heart from the left hip and is oriented to the inferior surface of the Left Ventricle.

24
Precordial Lead Placement
v1 - 4th ICS, R sternal border v2 - 4th ICS, L sternal border v3 - midway between v2 & v4 v4 - 5th ICS, L MCL v5 - 5th ICS, between v4 & v6 v6 - 5th ICS, L mid-axillary line Tip Some find it easier to put the leads on in this order v1, v2, v4, v6 Then v3 and v5

25
You Lookin’ at Me? It is important to look at contiguous leads to determine which area of the heart is affected. Each lead is like a camera lens that “looks” at an area of the heart.

26
And how do I know if I have the leads in the right place?
If everything in Lead I (P, QRS & T wave) is inverted, RA and RL are reversed. Watch for the progression of the R wave in the precordial leads. “R” WAVE PROGRESSION The right ventricle depolarizes faster than the left ventricle because it is smaller. The left ventricle sits to the left and posterior to the right ventricle. As current spreads leftward through the left ventricle, the height of the R wave in the precordial leads progressively increases. Normally, in V1 the R wave is more negative and as it progress to V6 the R wave becomes more positively deflected. “R” wave progression indicates that current is flowing normally through the anterior plane of the heart. (Conover)
 is inverted, RA and RL are reversed. Watch for the progression of the R wave in the precordial leads. R WAVE PROGRESSION. The right ventricle depolarizes faster than the left ventricle because it is smaller. The left ventricle sits to the left and posterior to the right ventricle. As current spreads leftward through the left ventricle, the height of the R wave in the precordial leads progressively increases. Normally, in V1 the R wave is more negative and as it progress to V6 the R wave becomes more positively deflected. R wave progression indicates that current is flowing normally through the anterior plane of the heart. (Conover)")
27
ECG Patterns As contiguous leads look at different parts of the heart, you may see an ischemic pattern that covers a large area or border area between two regions. For example, if there is ST-segment elevation in leads II/III/aVF/V5/V6, the ischemia appears to be on both the inferior and lateral areas, referred to as inferolateral. Likewise, there are anterolateral and anteroseptal (like the illustration here) ischemic patterns. What is an ischemic pattern? The AHA cites “typical ST-segment elevation” as “> 1 mm in 2 or more contiguous leads”
 ischemic patterns. What is an ischemic pattern The AHA cites typical ST-segment elevation as > 1 mm in 2 or more contiguous leads")
28
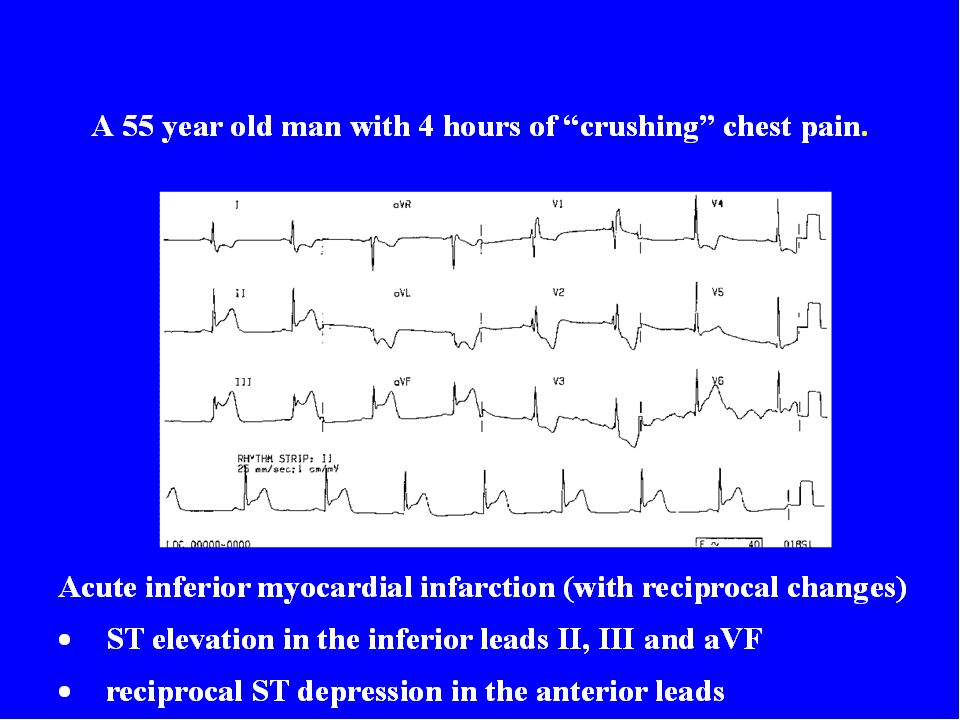
Injury=Elevated ST segment
Signifies an acute process; ST returns to baseline with time Location of injury can be determined in same manner as infarct location Usually associated with reciprocal ST depression in other leads If ST elevation is diffuse and unassociated with Q waves or reciprocal ST depression, consider pericarditis

30
Anterior MI LAD Most lethal with highest mortality
Can suddenly develop CHB, VF, VT If present with hemiblocks or BBB, Can extend to septum and/or lateral walls Nitrates are desired over fluids

31
Anterior Infarction

34
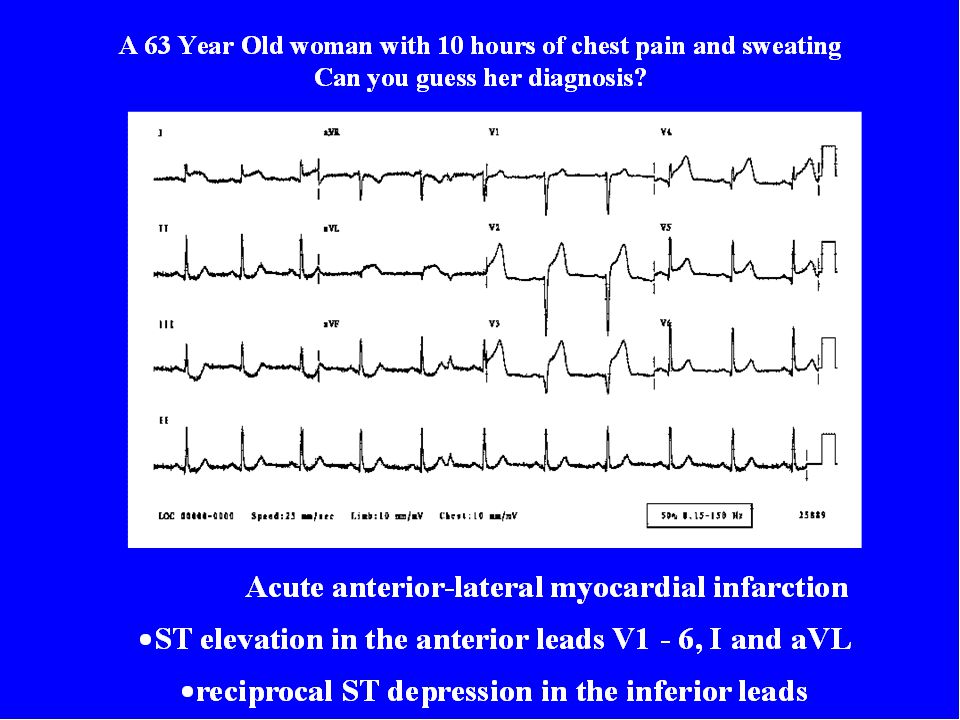
Anterior Infarction ST elevation without abnormal Q wave Usually associated with occlusion of the left anterior descending branch of the left coronary artery (LCA)
")
35
usually an extension of anterior or inferior MI
Lateral or Septal Wall MI Rarely seen alone, usually an extension of anterior or inferior MI Septal – Left Anterior Descending Lateral – Left Circumflex

38
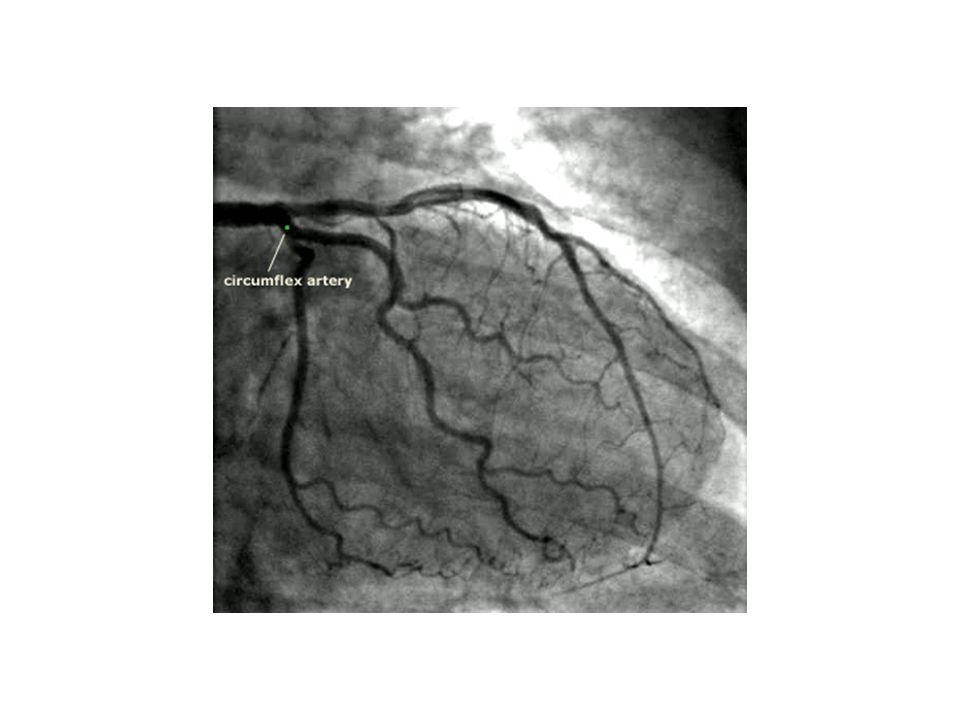
Pre Intervention Post Intervention

39
Lateral Infarction ST elevation with/without abnormal Q wave.
May be a component of a multiple-site infarction Usually associated with obstruction of the left circumflex artery.

40
Inferior Wall RCA The most common type of MI Nausea is common
Frequent re-infarction or extends to lateral wall SA / AV node SB, sinus arrest, HB - 1st or 2nd degree AV blocks, PVC’s Nitrates if BP stable Medical control may ask crew to hold nitro for inferior wall MI until right sided infarct is ruled out.

43
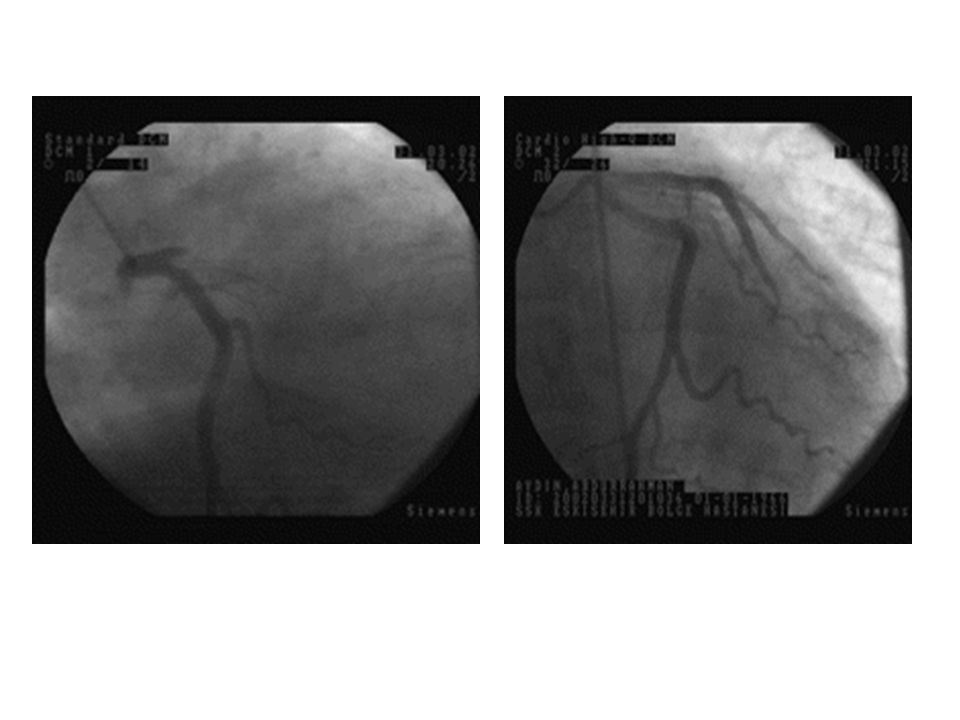
RCA STENOSIS

44
Post PCI Pre PCI

45
Inferior Infarction ST elevation with/without abnormal Q wave
Usually associated with right coronary artery (RCA) occlusion
 occlusion.")
46
Right Ventricular MI Rare RCA LAD or Left circumflex could also cause
Right sided heart failure Fluids – JVD with hypotension Watch for inferior wall MI too!

47
Right Ventricular Infarction
Usually accompanies inferior MI due to proximal occlusion of the RCA Best diagnosed ST elevation in lead V4R An important cause of hypotension in inferior MI recognized by jugular venous distension with clear lung fields Aggressive therapy is indicated including: reperfusion, adequate IV fluids for right heart filling, and pacing to maintain A-V synchrony

48
Posterior Wall RCA Left Circumflex Seen with Inferior or lateral wall

49
Posterior Infarction Tall, broad (>0.04 sec) R wave and
ST depression in V1 and V2 (reciprocal changes) Frequently associated with inferior MI Usually associated with obstruction of RCA and or left circumflex coronary artery
 Frequently associated with inferior MI. Usually associated with obstruction of. RCA and or left circumflex coronary artery.")
51
Reciprocal Changes Region of ST Elevation Region of ST Depression
Anterior (leads V1-V4) Inferior (true posterior) Inferior (leads II, III, aVF) Anterior (leads V1-V3 or lateral lead 1. aVL) Lateral ( leads I, aVF, V5, V6) Inferior ( leads II, III, aVF) True Posterior Anterior (leads V1-V3)
 Inferior (true posterior) Inferior (leads II, III, aVF) Anterior (leads V1-V3 or lateral lead 1. aVL) Lateral ( leads I, aVF, V5, V6) Inferior ( leads II, III, aVF) True Posterior. Anterior (leads V1-V3)")
52
Making the accurate Field Diagnosis: There are elevations (1 mm) in
two contiguous or connecting leads: (Leads adjacent to each other) There is at least one lead with reciprocal changes.. Reminder: ECG would have changes in the area where the heart is being affected. All other areas would look normal, without elevation or depression unless there is an "old MI." In that case, the prior damage would show up as a depressed segment.
 There is at least one lead with reciprocal changes.. Reminder: ECG would have changes in the area where the heart is being affected. All other areas would look normal, without elevation or depression unless there is an old MI. In that case, the prior damage would show up as a depressed segment.")
53
Treat The Patient… Not The Monitor
If the patient’s symptoms do not match the ECG, you need to do more detective work ECG is “nondiagnostic” in ~ 50% of patients with chest discomfort

55
12 Lead Review #1

56
#1

57
Normal 12 Lead / #1

59
Acute Anterior Lateral Infarct/ #2

60
#3

61
Anterolateral Infarct/ #3

62
#4

63
Acute Inferior Wall Infarct / #4

64
#5

66
#6

67
Anterio-lateral / #6

72
Bundle Branch Blocks Conduction Abnormalities
Right Bundle Branch Block

73
Right Bundle Branch Block

74
Pre PCI Post PCI

75
Mini-CME: Autism Many patients we encounter in EMS have some form of autism or fall somewhere on the autism spectrum of disorders. This month, please register for and complete the course Autism 101, found at: Submit the completion certificate to your EMS coordinator (or Silver Cross EMSS Operations if you are an independent provider).
.")
76
Thank you! Any further questions? If you are viewing the live presentation, please feel free to type them in the message box now. Otherwise, feel free to call or the EMS office or visit our website, ww.silvercrossems.com.

Similar presentations



















>")











>")
