Download presentation
Presentation is loading. Please wait.

1
Management of non naïve patients with hepatitis C Relapsers Alessandra Mangia Liver Unit & Division of Gastroenterology “CSS” San Giovanni Rotondo, Italy 3 rd Hepatitis Conference Paris 19-20 January 2009

2
Topics to be covered * Relapse rates following combination tx of standard or short duration * Predictors of relapse Duration of treatment RBV/IFN dosages * Re-treatment of relapsers

3
Background Non responders diverse groups of pts including Null responders 20% Partial responders 15% Breakthrough 10% Relapsers 15%

4
Definition:Relapse vs nonresponders Limit of detection PegInterferon/Ribavirin >4 log decline Weeks

5
How to recognize the pattern? HCV RNA should be assessed at 3 and 6 months after end of treatment To rule out late relapse HCV RNA assessment should be repeated 18 months after treatment Sensitivity of the assay should be at least 50 IU/ml

6
LATE RELAPSE AFTER COMBINATION TX Author/yrs Patients FU RNA+ve LDL of the HCV RNA No (yrs) (%) assay Marcellin ‘97 80 pts 4 7 50 IU/ml Lau ‘98 5 pts 6-13 0 100 cp/ml Swain ‘04 300 pts 2-3 1 50 IU/ml McHutchison ‘02 395 pts 3 2 1 cp/µg Veldt ’04 286 pts 4 5 <10 3 cp/ml Ferenci ‘05 175 pts >12 0 50 IU/ml
 (%) assay Marcellin ‘97 80 pts IU/ml Lau ‘98 5 pts cp/ml Swain ‘ pts IU/ml McHutchison ‘ pts cp/µg Veldt ’ pts 4 5 <10 3 cp/ml Ferenci ‘ pts > IU/ml")
7
Why a relapse occur ? Insufficient length of therapy Reduction of IFN or RBV

8
Duration of Treatment and Relapse: GT2/3 All Patients Hadziyannis S, et al. Ann Intern Med. 2004;140:346-355. 24 Weeks- LD 0 20 40 60 Patients (%) 24 Weeks- SD 80 100 48 Weeks- LD 48 Weeks- SD 94 84 90 81 11 10 4 79 82 85 80 6 SVR EOT REL
 24 Weeks- SD Weeks- LD 48 Weeks- SD SVR EOT REL.")
9
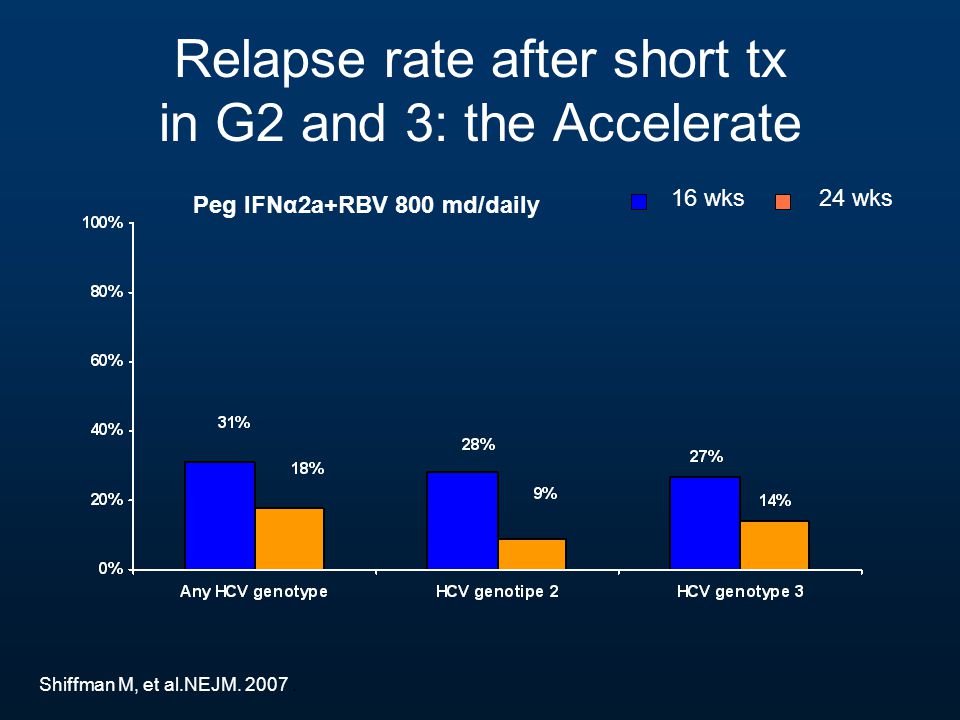
Relapse rate after short tx in G2 and 3: the Accelerate 16 wks 24 wks Peg IFNα2a+RBV 800 md/daily Shiffman M, et al.NEJM. 2007.
10
Duration of Treatment and Relapse: GT1 All Patients Hadziyannis S, et al. Ann Intern Med. 2004;140:346-355. 24 Weeks- LD 0 20 40 60 Patients (%) 24 Weeks- SD 80 100 48 Weeks- LD 48 Weeks- SD 68 29 78 42 39 36 19 41 60 69 52 6 SVR EOT REL
 24 Weeks- SD Weeks- LD 48 Weeks- SD SVR EOT REL.")
11
Relapse rates in G1 pts treated with PEGIFN 2 plus RBV based on time of first negative HCVRNA Time to first neg HCVRNA 24 wks virological relapse 48 wks virological relapse wk 49/106 (8%)1/12 (8%) wk 1244/59 (75%)0/14 (0%) wk 24 (EOT)16/20 (80%)0/2 (0%) ALL69/185 (37%)1/28 (4%) Zeuzem S. J Hepatol 2005

12
Re-treatment of relapser pts after an initial short (24 or 12 wks) treatment course StudyScheduleSVR (%) HCV G1Berg C, 2006Pegα2a+ RBV >1000 mg/daily 18/35 (51%) HCV G2/3Mangia A,2009Pegα2a+ RBV 1000- 1200 mg/daily 30/43 (70%)
 treatment course StudyScheduleSVR (%) HCV G1Berg C, 2006Pegα2a+ RBV >1000 mg/daily 18/35 (51%) HCV G2/3Mangia A,2009Pegα2a+ RBV mg/daily 30/43 (70%)")
13
Impact of Peg-IFN dose reduction PegIFN 135 µg is sufficient for treatment of chronic HCV 2 and 3 infection when combined with RBV doses daily according to body weight Weiland O, et al. J Viral Hepat. 2008;15:641-645. 0 20 40 60 Patients (%) EOT 80 100 Relapse SVR 9897 8,9 12,5 85 86 G 3 G 2
 EOT Relapse SVR ,9 12, G 3 G 2.")
14
> 9797-8180-61 n = 218 65 31 11 Relapse (%) 0 20 40 60 80 Cumulative Ribavirin Dose (%) 17 40 56 60-0 Impact of RBV dose reduction Reddy KR, et al. Clin Gastroenterol Hepatol 2007. Significant decrease in SVR for total relapse p=.0006

15
Treatment of Chronic HCV Impact of stopping Ribavirin 0 24 48 HCV RNA negative Peg-IFNα2a 180 µg/wk and RBV 800 mg/day (N=516) Continuing Peg-IFN Stop RBV N=176 Continuing Peg-IFN and RBV N=173 Wk Bronowicki J-P, et al. Gastroenterology 2006; 131: 1040

16
Effect of discontinuing RBV on HCV G1 pts responding to Tx Outcome Treatment during last 24 wksP value PegIFNα2a + RBV (n=173) PegIFNα2a (n=176) SVR (ITT)68.252.6.004 SVR (PP)71.556.7.006 Bronowicki J-P, et al. Gastroenterology 2006; 131: 1040

17
Intensive regimen in “difficult to cure” G1, high HCVRNA, >85 Kg PegIFNα-2a 180 µg/wk + RBV 1200 mg/day (n=46) PegIFNα-2a 180 µg/wk + RBV 1600 mg/day (n=47) PegIFNα-2a 270 µg/wk + RBV 1200 mg/day (n=47) PegIFNα-2a 270 µg/wk + RBV 1600 mg/day (n=47) Treatment-naïve Pts with G1, HCVRNA > 800,000 IU/ml and Body Weight > 85 kg N=188 Fried M et al, Hepatology 2008 wk 48 Follow-up
 PegIFNα-2a 180 µg/wk + RBV 1600 mg/day (n=47) PegIFNα-2a 270 µg/wk + RBV 1200 mg/day (n=47) PegIFNα-2a 270 µg/wk + RBV 1600 mg/day (n=47) Treatment-naïve Pts with G1, HCVRNA > 800,000 IU/ml and Body Weight > 85 kg N=188 Fried M et al, Hepatology 2008 wk 48 Follow-up")
18
Intensive regimen Tx resistant Relapse diminished Relapse rate - PegIFN 180 µg/wk +RBV 1200 mg/day: 40% - PegIFN 270 µg/wk +RBV 1200 mg/day: 42% - PegIFN 180 µg/wk +RBV 1600 mg/day: 46% - PegIFN 270 µg/wk +RBV 1600 mg/day: 19% Fried M et al, Hepatology 2008

19
Re-treatment of relapsers after std IFN + RBV

20
PegIFN alfa + RBV in Previous Relapsers Sherman M, et a. Gut 2006;55:1631-1638 Maucari R. et al J Hepatol 2007; 46:596-604 Jacobson IM, et al. Am J Gastroenterol. 2005;100:2453-2462. 0 10 20 30 40 50 60 70 80 100 90 38 53 50 32 PegIFN 2b 1.5 µg/kg/wk + RBV 800 mg/day (n = 30 ) PegIFN 2b 1.0 µg/kg/wk + RBV 1000-1200 mg/day (n = 25) SVR (%) IFN + RBV (n = 53) IFN + RBV (n = 55) IFN + RBV (n = 77) 48 Wks PegIFN 2a + RBV 800 mg/day (n = 85 ) PegIFN 2b 1.5 µg/kg/wk + RBV 1000-1200 mg/day (n = 53)
 PegIFN 2b 1.0 µg/kg/wk + RBV mg/day (n = 25) SVR (%) IFN + RBV (n = 53) IFN + RBV (n = 55) IFN + RBV (n = 77) 48 Wks PegIFN 2a + RBV 800 mg/day (n = 85 ) PegIFN 2b 1.5 µg/kg/wk + RBV mg/day (n = 53).")
21
SVR 3% No 68 (44%) SVR 49% Yes 86 (56%) Maucari R, et al.J Hepatol. 2007 At Week 12 (N = 154) Predictive value of EVR SVR 97% SVR 51% Yes No Yes No
 Predictive value of EVR SVR 97% SVR 51% Yes No Yes No.")
22
Treatment of Relapsers after PegIFN + RBV given for 48 weeks

23
StudyTreatmentGTN (Previous Treatment) SVR Rate (Previous Treatment) Kaiser [1] CIFN 9 µg/day + RBV x 72 weeks 112069% PegIFN alfa-2a + RBV x 72 weeks 42% EPIC3 [2] PegIFN alfa-2b + RBV x 48 weeks 1 (81%) 2/3 (15%) 164 (PegIFN alfa-2a) 180 (PegIFN alfa-2b) 34% (PegIFN alfa-2a) 32% (PegIFN alfa-2b) Outcomes in Relapsers to PegIFN-Based Therapy 1. Kaiser S, et al. AASLD 2007. Abstract 1310. 2. Gross J, et al. AASLD 2005. Abstract 60.
![StudyTreatmentGTN (Previous Treatment) SVR Rate (Previous Treatment) Kaiser [1] CIFN 9 µg/day + RBV x 72 weeks % PegIFN alfa-2a + RBV x 72 weeks 42% EPIC3 [2] PegIFN alfa-2b + RBV x 48 weeks 1 (81%) 2/3 (15%) 164 (PegIFN alfa-2a) 180 (PegIFN alfa-2b) 34% (PegIFN alfa-2a) 32% (PegIFN alfa-2b) Outcomes in Relapsers to PegIFN-Based Therapy 1.](http://images.slideplayer.com/14/4332463/slides/slide_23.jpg "Kaiser S, et al. AASLD Abstract Gross J, et al. AASLD Abstract 60..")
24
EPIC 3 NR Study HCV pts (18-65 yrs) with Metvir score F2-4 n=2293 Previous Tx = 62% IFN/RBV, 21% PegIFN alfa-2b, 16% alfa 2a Poynard EASL 2008 Patients (%) PegIFN alfa-2b 1.5 µg/Kg/wk +Weight-based RBV 800-1400 mg/day/48 wks
 with Metvir score F2-4 n=2293 Previous Tx = 62% IFN/RBV, 21% PegIFN alfa-2b, 16% alfa 2a Poynard EASL 2008 Patients (%) PegIFN alfa-2b 1.5 µg/Kg/wk +Weight-based RBV mg/day/48 wks")
25
Does the presence of an advanced liver disease influence the relapse rate?

26
Predictors of relapse in 485 patients with RVR following a short (12 weeks) therapy Peg INF α2b (1.5 μg/kg) + RBV (800-1200 mg) EOT: 96%; SVR: 82%, Relapse: 14% Predictors o Predictors of relapsepOR; 95% CI Age >45 years0.004- BMI >30 kg / m 2 0.00012.5; 1.49 – 4.20* Platelet counts <140.000 m 3 0.00011.7; 1.03 – 2.70* *independently associated with SVR Mangia et al, Hepatology 2009
 therapy Peg INF α2b (1.5 μg/kg) + RBV ( mg) EOT: 96%; SVR: 82%, Relapse: 14% Predictors o Predictors of relapsepOR; 95% CI Age >45 years BMI >30 kg / m ; 1.49 – 4.20* Platelet counts < m ; 1.03 – 2.70* *independently associated with SVR Mangia et al, Hepatology 2009")
27
TotalSVRRelapse Pts without risk factors* 316290 (91,8%)26 (8,2%) Pts with 1 or 2 risk factors* 169128 (74,4%)41 (25,6%) SVR and relapse rates in 485 RVR genotypes 2 and 3 patients after short therapy (12 wks), according to the presence or absence of risk factors* Mangia et al, Hepatology 2009 * BMI >30 and/or PLT <140,000
26 (8,2%) Pts with 1 or 2 risk factors* (74,4%)41 (25,6%) SVR and relapse rates in 485 RVR genotypes 2 and 3 patients after short therapy (12 wks), according to the presence or absence of risk factors* Mangia et al, Hepatology 2009 * BMI >30 and/or PLT <140,000")
28
Final Results from the EPIC 3 Program Poynard T et al EASL 2008 Study Outline: PegIFN-α2b 1.5 mcg/Kg week + Rbv 800-1400 mg/day NR and RR to combo therapy with any IFN Genotype Peg-α2b (n=180) Peg-α2a (n=164) IFN alfa (n=300) G1 F237%27%42% F418%20%26% G2/3 F275%50%76% F436%58%59% SVR in Prior Relapsers
 Peg-α2a (n=164) IFN alfa (n=300) G1 F237%27%42% F418%20%26% G2/3 F275%50%76% F436%58%59% SVR in Prior Relapsers")
29
New agents

30
Telaprevir + Pegasys + Copegus in G1 NR or Relapsers to Peg-IFN + RBV PROVE 3 Study Weeks 48 0 Placebo plus PEGASYS ®† plus COPEGUS ®†† TVR ‡ 750 mg q8h plus PEGASYS ®† plus COPEGUS ®†† TVR ‡ 750 mg q8h plus PEGASYS ®† CHC, G1, NR and REL to peg-IFN + RBV, n=453 24 $ 12 § f/u 24 wks PEGASYS ®† plus COPEGUS ®†† TVR ‡ 750 mg q8h plus PEGASYS ®† plus COPEGUS ®†† f/u 24 wks f/u 48 wks A B C D Placebo plus PEGASYS ®† plus COPEGUS ®†† f/u 48 wks PEGASYS ®† plus COPEGUS ®††

31
PROVE 3 – Interim Results in Prior G1 Relapsers McHutchison et al, AASLD 2008

32
Telaprevir + PegIFN alfa-2a + RBV in Nonresponders or Relapsers Open-label treatment of patients from control arms of PROVE1-3 trials Poordad F, et al. EASL 2008. Abstract 1000. 0 20 40 60 80 100 Undetectable HCV RNA, < 10 IU/mL (%) Wk 4 (RVR) 33 50 79 Wk 4 Null Responder* Wk 12 Null Responder † Partial Responder ‡ Wk 20 Breakthrough Relapser 67 100 89 100 80 100 Wk 8Wk 12 *< 1 log 10 drop at Wk 4. † <2 log 10 drop at Wk 12. ‡ ≥ 2 log 10 drop at Wk 12; detectable HCV RNA at Wk 24.
 Wk 4 (RVR) Wk 4 Null Responder* Wk 12 Null Responder † Partial Responder ‡ Wk 20 Breakthrough Relapser Wk 8Wk 12 *< 1 log 10 drop at Wk 4. † <2 log 10 drop at Wk 12. ‡ ≥ 2 log 10 drop at Wk 12; detectable HCV RNA at Wk 24..")
33
Conclusions Relapsers are good candidates to re- treatment with PegIFN and RBV combination EVR stopping rule recommended Optimize weight-based RBV dose during re- treatment Consider longer duration of re-treatment (cirrhotic, obese) Higher doses of PegIFN alpha may be superior to standard dose in selected patients (G1, obese) Potential role for cIFN
 Higher doses of PegIFN alpha may be superior to standard dose in selected patients (G1, obese) Potential role for cIFN")
35
Q.1 Which factors, among the following, are associated with a relapse in patients infected with genotype 1? Short duration of initial course Low dose of ribavirin Severe liver damage All the previous

36
Q.2 For how long should a cirrhotic patient with genotype 2 infection who relapsed after 12-14 wks of treatment be re-treated ?

37
Q.3 Which treatment would you advise for a genotype 1 65 yr-old non-cirrhotic pt relapsing after 48 wks of PegIFN and RBV combination? Telaprevir and PegIFN 9 mcg of CIFN + RBV for 72 wks PegIFN and RBV for 48 wks

38
Q.3 Which is the minimum decline on treatment and at what time should it be assessed to decide not to stop re- treatment? If a minimum of a 1 log decline occurs at wk 12 it may be reasonable to continue tx and reassess HCV RNA periodically

39
Relapse rates in Genotype 2 and 3 after RVR 12 – 16 wks 24 wks %

40
Key Questions for HCV Patients Facing Retreatment 1.What were you treated with, at what dosage, and for how long? 2.What type of response did you have? 3.What is your GT? 4.Did you require dose reductions or treatment interruptions during previous therapy? What adverse effects caused these interruptions/dose reductions? 5.Were you overweight during previous courses of therapy? 6.Were there adherence issues? 7.Do you have any significant comorbidities/other conditions that may affect your response to treatment? 8.Did you have a good support system during previous courses of treatment? What do you have now?

41
Summary : re-treatment of Relapsers Response pattern IFN Response Re- Treatment strategy Maintenance Tx RelapseYesTreat for 72 weeks Yes, if it can keep RNA-ve

Similar presentations






 PROMISE Trial Phase 3 Treatment Experienced Forns X, et al. Gastroenterology.>")

 in the Treatment of Chronic Hepatitis C Virus Presentation Prepared by: David.>")
 WINR Study Phase 3 Treatment.>")
 Phase 3 Treatment Experienced Zeuzem S, et al. N Engl.>")

 Phase 3 Treatment Naïve Jacobson IM, et. al. N Engl J Med.>")





 Phase 3 Treatment Naïve Sherman KE, et. al. N Engl J.>")

