Download presentation
Presentation is loading. Please wait.

1
Dr Narisha Ramparsad Department of Haematology and Molecular Medicine
VENOUS THROMBOSIS Dr Narisha Ramparsad Department of Haematology and Molecular Medicine

2
Normal haemostasis Ensures fluid state of blood in vasculature
Prevents blood loss – site of injury – by forming haemostatic plug Clot removal – when healing is complete

3
Overview of Haemostasis
THROMBOSIS BLEEDING

4
Definitions A blood clot that forms in a blood vessel or within the heart and remains there is called a thrombus. A thrombus that travels from the blood vessel or heart to another location in the body is called an embolus, and the disorder, an embolism. For example, an embolus that occurs in the lungs is called a pulmonary embolism. Sometimes, a piece of atherosclerotic plaque, small pieces of tumor, fat clumps, air, amniotic fluid, or other materials can act in the same manner as an embolus. (MEDLINE PLUS)
")
5
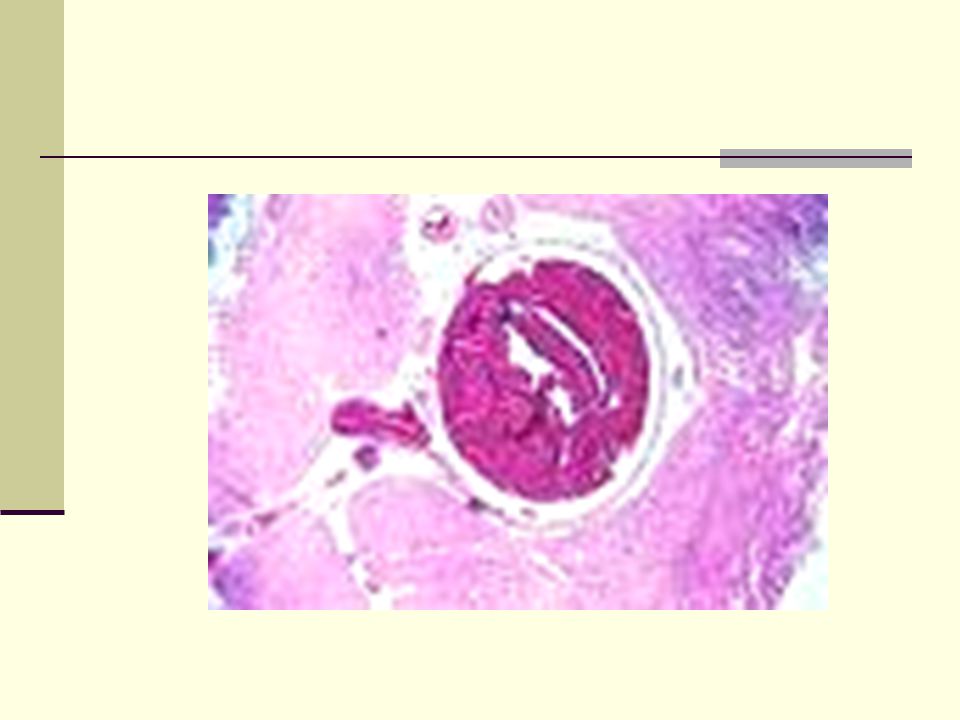
Pathogenesis -Thrombosis
Normally - balance between clotting and bleeding With thrombosis - imbalance with procoagulant state manifesting Risk increases when > 1 risk factor present Venous thrombi – fibrin & RBCs mainly, leucocytes & plts also present Virchow’s triad 1) vessel wall damage 2) blood flow (stasis) 3) hypercoaguability of blood Venous thrombosis can affect any part of venous system but deep veins most commonly affected.
 vessel wall damage. 2) blood flow (stasis) 3) hypercoaguability of. blood. Venous thrombosis can affect any part of venous system but deep veins most commonly affected.")
7
Acquired Risk Factors Malignancy Presence of a central venous catheter
Surgery, especially orthopedic Trauma Pregnancy Oral contraceptivesHormone replacement therapyTamoxifen Immobilization Congestive failure Antiphospholipid antibody syndrome Myeloproliferative disorders Polycythemia vera,Essential thrombocythemia Paroxysmal nocturnal hemoglobinuria Inflammatory bowel disease Nephrotic syndrome Hyperviscosity e.g Waldenstrom's macroglobulinemia, Multiple myeloma Marked leukocytosis in acute leukemia Sickle cell anemia

8
Acquired Risk Factors NB in South Africa – effect of HIV
Decrease Protein S, Protein C Increase Factor VIII

9
Inherited Risk Factors
Factor V Leiden mutation Prothrombin gene mutation Protein S deficiency Protein C deficiency Antithrombin (AT) deficiency Rare disorders: Dysfibrinogenemia
 deficiency. Rare disorders: Dysfibrinogenemia.")
10
Coagulation Cascade – Inherited Risk factors – thrombosis

11
Venous thromboembolism (VTE)
VTE = Deep Vein Thrombosis (DVT) and/or Pulmonary Embolism (PE) Incidence increases with age 117 cases/ Increasing health problem – prevention important, potentially fatal
 and/or Pulmonary Embolism (PE) Incidence increases with age. 117 cases/ Increasing health problem – prevention important, potentially fatal.")
12
VTE

13
VTE Thrombosis commonly occurs in deep veins of limbs. Can also affect superficial veins Venous system leg – 2 important categories deep calf vein involvement only proximal vein thrombosis (involving popliteal, femoral or iliac veins) – give rise to clinically significant PE Pulmonary emboli ( majority arise from deep veins of leg >90%) Other sources of PE include – upper extremity thrombosis, deep pelvic veins, renal veins, IVC
 – give rise to clinically significant PE. Pulmonary emboli ( majority arise from deep veins of leg >90%) Other sources of PE include – upper extremity thrombosis, deep pelvic veins, renal veins, IVC.")
14
DEEP VEINS OF THE LEG

15
DEEP VEIN THROMBOSIS – clinical features
Leg pain, swelling, tenderness, palpable cord (thrombosed vessel), phlegmasia cerulea dolens in occasional patients. Non specific signs and symptoms.
, phlegmasia cerulea. dolens in occasional patients. Non specific signs and. symptoms.")
17
Differential Diagnosis DVT
Cellulitis Popliteal cyst Lymphatic obstruction Muscle strain/tear Direct twisting injury to leg If think about DVT – MUST objectively exclude

18
Pulmonary Embolism – Clinical Features
Symptoms variable Transient Dyspnoea, tachypnoea Tachycardia Pleuritic chest pain, cough, haemoptysis, CVS collapse with hypotension, syncope ( massive pulmonary embolism) Clinically silent Clinical features are non specific ONCE again must objectively exclude
 Clinically silent. Clinical features are non specific. ONCE again must objectively exclude.")
19
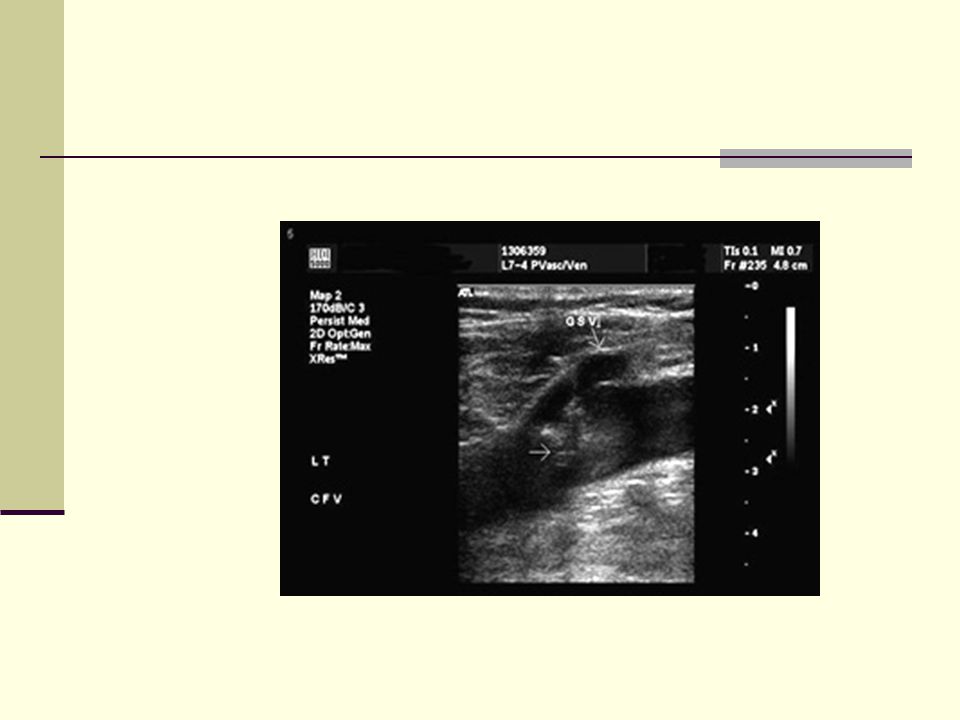
Laboratory investigations
D-Dimer assay Compression ultrasound(DVT) Venography (DVT) Spiral CT (highly sensitive for PE MRI Work up for thrombophilic state when confirm diagnosis
 Venography (DVT) Spiral CT (highly sensitive for PE. MRI. Work up for thrombophilic state when confirm diagnosis.")
21
Clinical course Untreated proximal vein thrombosis – potentially lethal – fatal PE Extension of thrombus proximally Post thrombotic syndrome frequent complication of deep DVT. Heaviness, swelling cramps, itching, ulceration Chronic thromboembolic pulmonary hypertension.

22
Treatment – Anticoagulant Therapy
Heparin: Unfractionated or Low Molecular Weight Heparins e.g Enoxaprin(Clexane), Dalteprin, Fondaparinux Vitamin K antagonists e.g Warfarin Oral anti Xa (clinical trials) Direct thrombin inhibitors
, Dalteprin, Fondaparinux. Vitamin K antagonists e.g Warfarin. Oral anti Xa (clinical trials) Direct thrombin inhibitors.")
23
Initiation of treatment
Must cover with Clexane when initiating Rx with Warfarin – Why? ( short T1/2, Protein C) – relative prothrombotic state
 – relative prothrombotic state.")
24
Treatment – how long? Individualise each case
Look at risk factors present Transient vs permanent vs no risk factors 1st episode vs recurrent thrombosis Reassess D-Dimer levels Risk –Benefit ratio of anticoagulant therapy

25
Treatment – how long ? First onset ,transient risk factor – 6 months , recheck D-Dimer levels . If raised continue ? Indefinite therapy. First onset, idiopathic thrombosis – consider life long Warfarin. Reassess risk-benefit ratio Recurrent DVT – indefinite anticoagulation Patients with APL antibodies or 2 more inherited risk factors – 12 months anticoagulation and reassess

26
Treatment how long First episode thombosis – with deficiency of natural anticoagulants e.g. antithrombin, Prot C, Prot S or FVLeiden/Prothrombin gene mutation – 12 months and reassess ? indefinite therapy

27
Side effects of anticoagulant therapy
Bleeding Heparin Induced thrombocytopenia and thrombosis Heparin induced osteoporosis, increased transaminase levels, hypersensitivity reactions e.g. necrosis, alopecia, hyperkalaemia

28
Treatment – Thrombolytic therapy – When?
Indicated in patients with PE – haemodynamically unstable , evidence of R ventricular failure Threatened limb in setting of DVT

29
Prophylaxis – venous thrombosis
Important to identify those patient at increased risk of thrombosis Prevention Use of LMWH, compression stockings Awareness – patients and health care professionals

30
CONCLUSION Venous thromboembolism – major cause of morbidity and mortality Identify risk factors early -institute prophylaxis Prophylaxis imperative measure to decrease incidence of thrombotic events If suspect thrombosis must objectively test Duration of treatment – varies -individualise

Similar presentations







 is produced by a shift in the balance between.>")





 around valves propagation Virchow’s triad.>")






