Download presentation
Presentation is loading. Please wait.

1
Lecturer: Dr Lucy Patston lpatston@unitec.ac.nz

2
Lundy: Chapter 10/11 Lundy: Chapter 12 (traumatic injury to peripheral nerves) Lundy-Ekman. Neuroscience: Fundamentals for Rehabilitation, 4th Edition. W.B. Saunders Company, 2013. Kandel et al. Principles of Neural Science, 5 th Edition. McGraw Hill, 2012. Tortura & Derrickson. Principles of anatomy and physiology, 13 th Edition. Wiley. 2012.

3
Disorders of LMNs (Polio) Disorders of UMNs Basal Nuclei Movement Disorders ◦ Hypokinetic Disorders Parkinson’s Disease - seminar ◦ Hyperkinetic Disorders Huntington’s Disease - seminar Cerebellar Disorders Cerebral Palsy
 Disorders of UMNs Basal Nuclei Movement Disorders ◦ Hypokinetic Disorders Parkinson’s Disease - seminar ◦ Hyperkinetic Disorders Huntington’s Disease - seminar Cerebellar Disorders Cerebral Palsy")
4
Have an understanding of different types of disorders that can affect the motor system Gain an appreciation for difficulties experienced by people with CP and how, as an osteo, these can be mitigated

5
Paresis or paralysis ◦ Decreased ability or inability to generate muscle force Muscle atrophy ◦ Loss of muscle bulk as pattern of muscle protein production changes Involuntary muscle contraction ◦ Spasms, cramps, fasciculations (eye twitch), tremors Abnormal muscle tone ◦ Muscle tone: resistance to stretch in resting muscle ◦ Hypotonia and flaccidity are abnormally low resistance to, or lack of resistance to passive stretch ◦ Hypertonia is abnormally strong resistance to passive stretch
, tremors Abnormal muscle tone ◦ Muscle tone: resistance to stretch in resting muscle ◦ Hypotonia and flaccidity are abnormally low resistance to, or lack of resistance to passive stretch ◦ Hypertonia is abnormally strong resistance to passive stretch")
6
Caused by: traumatic injuries, infections like Poliomyelitis (next), degenerative or vascular disorders, tumors Interrupting LMN signals to muscle decreases or prevents muscle contraction, leading to: ◦ Loss of reflexes ◦ Atrophy ◦ Flaccid paralysis ◦ Fibrillations
, degenerative or vascular disorders, tumors Interrupting LMN signals to muscle decreases or prevents muscle contraction, leading to: ◦ Loss of reflexes ◦ Atrophy ◦ Flaccid paralysis ◦ Fibrillations")
7
Poliovirus affects only LMNs Onset marked by fever, severe headache, stiff neck/back, deep muscle pain/weakness Enters body from faeces- contaminated water (pool) Destroys cell bodies of motor neurons (ventral horn) and, therefore, denervates muscle fibers (Wallerian degeneration – plasticity lecture) Unilateral Victim may die from paralysis of respiratory muscles or cardiac arrest (if neurons in medulla oblongata are destroyed)
 Destroys cell bodies of motor neurons (ventral horn) and, therefore, denervates muscle fibers (Wallerian degeneration – plasticity lecture) Unilateral Victim may die from paralysis of respiratory muscles or cardiac arrest (if neurons in medulla oblongata are destroyed)")
8
Horizontal section of a spinal cord post polio. The section has been stained for myelin, so that the white matter appears dark. Loss of cell bodies is visible in the anterior (ventral) horn.
 horn..")
10
Epidemic in 1940s & 50s “Recovered” survivors now experience extreme lethargy, sharp burning pain in muscles, progressive muscle weakness and atrophy Postpolio syndrome Most common LMN disease in US Overextended neurons can no longer support excessive number of distal branches

11
UMNs damaged by spinal cord injury, spastic CP, MS, trauma, loss of blood supply (stroke) Changes in movement control include: ◦ Paresis or paralysis ◦ Loss of fractionation of movement ◦ Abnormal reflexes ◦ Velocity-dependent hypertonia
 Changes in movement control include: ◦ Paresis or paralysis ◦ Loss of fractionation of movement ◦ Abnormal reflexes ◦ Velocity-dependent hypertonia")
12
Paresis or paralysis ◦ Paresis common following stroke, CP, trauma ◦ Leads to muscle disuse -> secondary changes in muscles and nervous system (causes adaptive muscle contracture and atrophy, and decreases motor cortex representation, further exacerbating paresis) ◦ Paralysis occurs from complete spinal cord lesion ◦ Loss of all somatosensory and motor function below level of lesion Loss of fractionation of movement ◦ Fractionation is ability to move individual muscles independently (piano) ◦ Lower limbs: interferes with dorsiflexion of ankle – plantarflexion instead
 ◦ Paralysis occurs from complete spinal cord lesion ◦ Loss of all somatosensory and motor function below level of lesion Loss of fractionation of movement ◦ Fractionation is ability to move individual muscles independently (piano) ◦ Lower limbs: interferes with dorsiflexion of ankle – plantarflexion instead")
13
Abnormal reflexes ◦ Babinski’s sign (usual for infants under 7mo – WHY?) ◦ Extension of big toe in response to stroking sole of foot – mechanism not understood Velocity-dependent hypertonia ◦ Limits joint range of motion, interfering with function E.g., toe walking due to lack of ankle dorsiflexion (prevents heels from touching floor)
 ◦ Extension of big toe in response to stroking sole of foot – mechanism not understood Velocity-dependent hypertonia ◦ Limits joint range of motion, interfering with function E.g., toe walking due to lack of ankle dorsiflexion (prevents heels from touching floor)")
14
Disease destroys only somatic motor neurons UMNs and LMNs bilaterally resulting in UMN and LMN signs concurrently Paresis, myoplasticity (changes in the muscles), hyperreflexia (overactive reflexes), Babinski’s sign, atrophy, fasciculations, fibrillations Loss LMNs in cranial nerves causes difficulty breathing, swallowing, speaking Death occurs ~5yrs, onset 50yrs+ Astrocytes fail to clean up excessive glutamate, causing excitotoxicity (more on this in plasticity lecture)
, hyperreflexia (overactive reflexes), Babinski’s sign, atrophy, fasciculations, fibrillations Loss LMNs in cranial nerves causes difficulty breathing, swallowing, speaking Death occurs ~5yrs, onset 50yrs+ Astrocytes fail to clean up excessive glutamate, causing excitotoxicity (more on this in plasticity lecture)")
16
Spinal cord section, stained for myelin, showing loss of upper motor neurons (UMNs) in amyotrophic lateral sclerosis (ALS). The loss is visible dorsolaterally, where the lateral corticospinal and rubrospinal axons should be, and ventromedially, where the medial UMNs should be

17
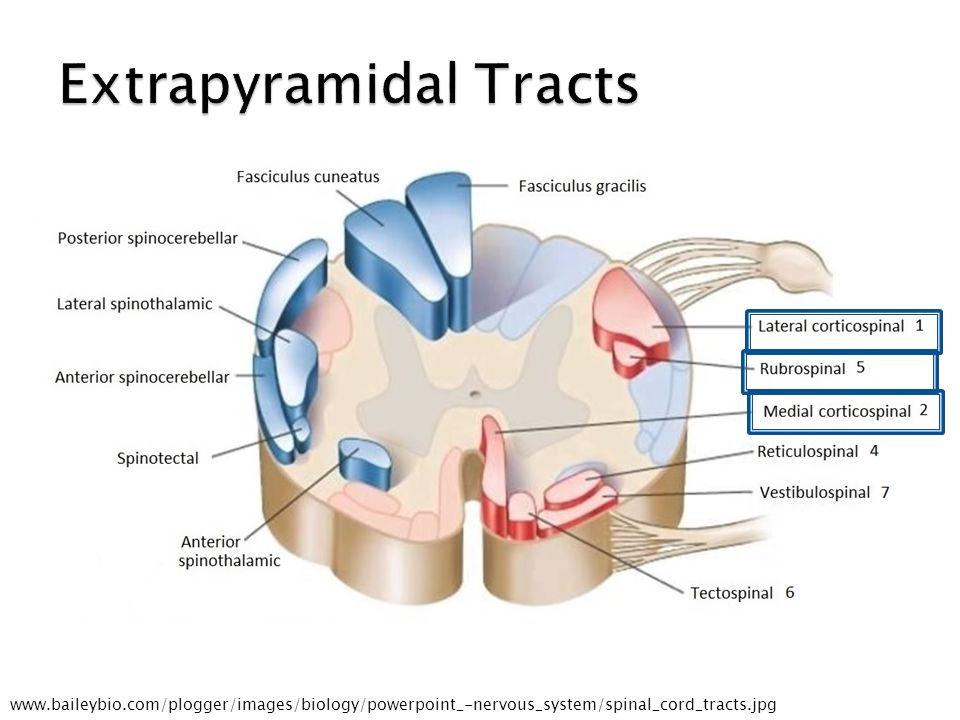
www.baileybio.com/plogger/images/biology/powerpoint_-nervous_system/spinal_cord_tracts.jpg
19
TABLE 10-4 TERMS DESCRIBING IMPAIRMENTS COMMON IN UPPER MOTOR NEURON LESIONS*

21
Range from hypokinetic (too little movt) to hyperkinetic (too much movt) disorders BN INHIBIT motor thalamus, PPN and MLR Excessive inhibition -> hypokinetic disorder (PD) Inadequate inhibition -> hyperkinetic disorder (HD) Red facilitation Black inhibition
 to hyperkinetic (too much movt) disorders BN INHIBIT motor thalamus, PPN and MLR Excessive inhibition -> hypokinetic disorder (PD) Inadequate inhibition -> hyperkinetic disorder (HD) Red facilitation Black inhibition")
22
Seminar topic: Emma, Chelsea, Amanda, Russell Hypokinetic disorder Akinetic/rigid 50% Tremor-dominant 40% Mixed 10% Let’s cover pathology: ◦ Death of dopaminergic cells in substantia nigra compacta (cell death occurs to 80% before signs of PD become apparent)
")
25
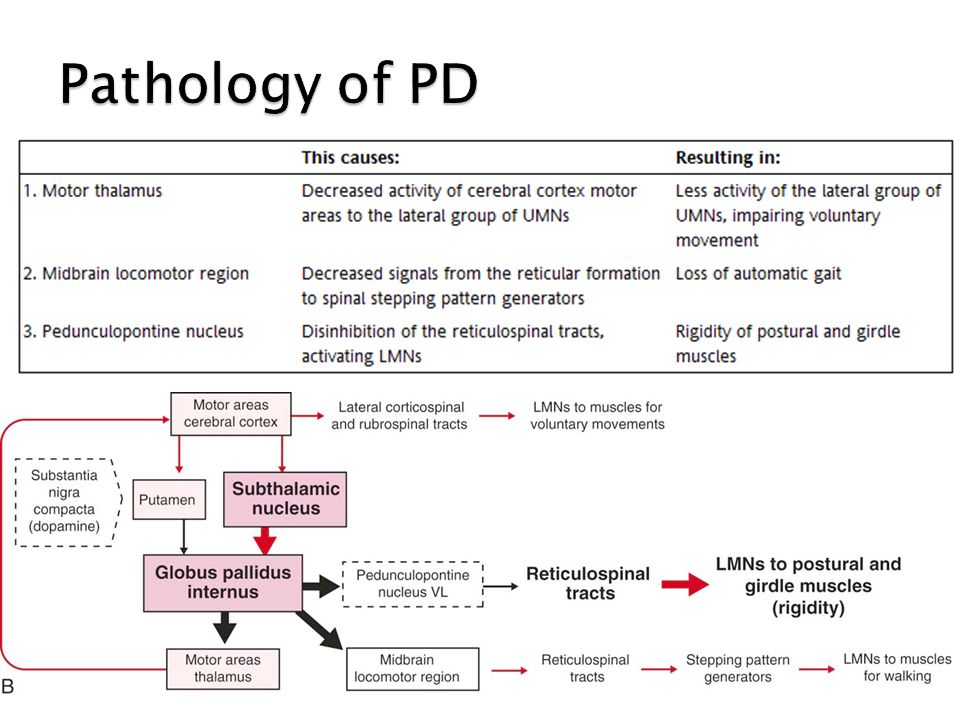
Loss of dopamine to putamen reduces level of inhibition provided to GP internus Therefore GP internus provides excessive inhibition to 3 pathways Downstream effects are: Decreased voluntary movts Excessive contraction of postural muscles Loss of automatic gait

28
Seminar topic: Kaspara, Matthew, Bryan Hyperkinetic disorder Autosomal dominant hereditary disorder Degeneration of striatum and cerebral cortex Characterised by chorea (dance) – jerky, involuntary movts that interfere with daily functioning ad cognitive decline Let’s cover pathology: ◦ Death of cells in striatum lead to excessive involuntary movt (chorea)
 – jerky, involuntary movts that interfere with daily functioning ad cognitive decline Let’s cover pathology: ◦ Death of cells in striatum lead to excessive involuntary movt (chorea)")
29
Degeneration (HD disease) decreases signals from GP internus Leading to disinhibition (not enough inhibition!) of motor thalamus and PPN Downstream effects are: Insufficient activity to girdle muscles hyperkinesia Not shown: Subthalamic nucleus output decr. due to enhanced activity of Gpe. MLR omitted due to lack of data of function in HD.

31
Ataxia: inability to coordinate muscular movements Symptoms: unable to close eyes touch nose, staggered walking, changed speech pattern (ringing any alcohol-related bells???!) Alcohol inhibits activity of cerebellum http://www.hhmi.org/biointeractive/neurosci ence/spinocerebellar_ataxia.html
 Alcohol inhibits activity of cerebellum ence/spinocerebellar_ataxia.html")
32
ICD-10, WHO classification of CP: ◦ “difficult to define but is conventionally described as a group of motor disorders with or without associated sensory and intellectual deficits where the cause is injury to the immature brain” Movement and postural disorder caused by permanent, non-progressive damage to developing brain (in utero 80% of time)
")
33
Brain damage may have been: ◦ Asphyxia (oxygen deprivation during birth) ◦ Infection ◦ Trauma ◦ Metabolic disorder ◦ Unknown Type classification: ◦ Spastic ◦ Dyskinetic ◦ Ataxic ◦ Hypotonic ◦ Mixed
 ◦ Infection ◦ Trauma ◦ Metabolic disorder ◦ Unknown Type classification: ◦ Spastic ◦ Dyskinetic ◦ Ataxic ◦ Hypotonic ◦ Mixed")
34
Type classification: ◦ Spastic excessive involuntary skeletal muscle contraction (high muscle tone, stiff muscles -> toe walking) Damage is to axons adjacent to lateral ventricles In developmental spastic CP: Lesion affects corticospinal and corticobulbar tracts During normal development corticospainal axon may synapse with agonist muscle as well as synergists and antagonists. Syngerists/antagonists normally eliminated by age 4 Inappropriate connections not eliminated during dev. CP cause co-contraction of antagonist muscles, interfering with performance Also disinhibition of reticulospinal tract causing abnormal synergies, and overactivation of neck reflexes (collicular signals to reticulospianl tract)
.")
35
Type classification: ◦ Spastic ◦ Dyskinetic muscle tone fluctuates from hypotonia to hypertonia Choreoathetosis – involuntary choreiform (jerky, abrupt, irregular movts, lack of coordination) Athetosis – slow, writhing movts Dystonia – involuntary sustained muscle contraction Damage is in basal nuclei and ventrolateral thalamus
 Athetosis – slow, writhing movts Dystonia – involuntary sustained muscle contraction Damage is in basal nuclei and ventrolateral thalamus")
36
Type classification: ◦ Spastic ◦ Dyskinetic ◦ Ataxic Incoordination, weakness, shaking during voluntary movt Damage is in the cerebellum

37
Type classification: ◦ Spastic ◦ Dyskinetic ◦ Ataxic ◦ Hypotonic Low muscle tone (floppy), little or no ability to move Damage site unknown
, little or no ability to move Damage site unknown")
38
Type classification: ◦ Spastic ◦ Dyskinetic ◦ Ataxic ◦ Hypotonic ◦ Mixed If more than one type of abnormal movement coexist Philip has choreoathetosis and spasticity CP also classified as: ◦ Hemiplegic, quadriplegic, diplegic (upper limbs less severely affected)
")
39
Problems with fine motor skills (writing) Walking or balance (or both) Involuntary movements (some types of CP) Difficulties with speech, eating, swallowing Cognitive impairment Visual or auditory impairment
 Walking or balance (or both) Involuntary movements (some types of CP) Difficulties with speech, eating, swallowing Cognitive impairment Visual or auditory impairment")
Similar presentations







 (MND) are a group of neurological disorders that selectively affect motor neurons.>")


















