Download presentation
Presentation is loading. Please wait.

1
Polio Eradication Dr Marvin Hsiao Division of Medical Virology NHLS/UCT/Groote Schuur Hospital

2
The virus Single strand positive sense RNA virus Non-enveloped Family Picornaviridae Genus Enterovirus 3 types, poliovirus 1-3 Grows well in cell culture

3
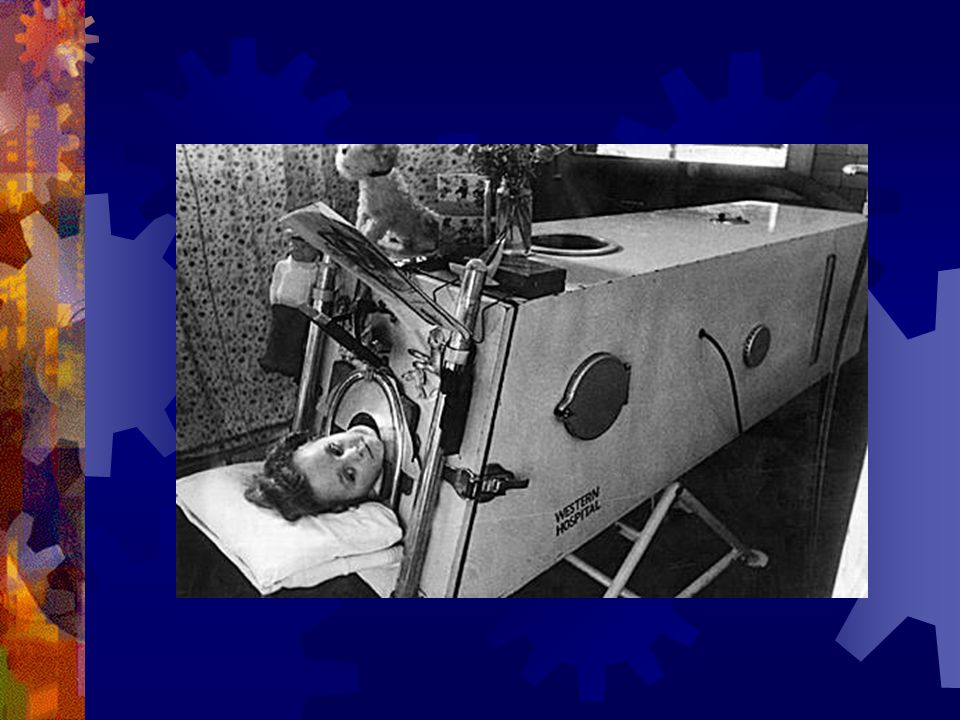
The pathogenesis Faecal oral transmission (+respiratory) Replicate in the lymphoid tissue in throat and gut - Viraemia Replication in neuronal cell – especially motor neuron in spinal cord (polios: grey muelos: marrow) Lytic infection of neurons Anterior horn cell Axon degeneration LMN (flaccid) paralysis
 Replicate in the lymphoid tissue in throat and gut - Viraemia Replication in neuronal cell – especially motor neuron in spinal cord (polios: grey muelos: marrow) Lytic infection of neurons Anterior horn cell Axon degeneration LMN (flaccid) paralysis")
4
The disease Poliovirus infection asymptomatic Full recovery Mild Febrile Illness Meningitic Stage Acute Flaccid Paralysis (+/-1%) Death Post polio syndrome Adapted from Collier & Oxford Human Virology 2 nd Edition
 Death Post polio syndrome Adapted from Collier & Oxford Human Virology 2 nd Edition")
7
The vaccines Oral Polio vaccine (OPV) Inactivated Polio vaccine (IPV) DeveloperAlbert SabinJonas Salk Production Method Serial passage to attenuate strain (live) Formalin inactivated Tissue culture supernatant Costcheapexpensive RouteOralIM injection Type of immunity Produce good gut immunity Less robust gut immunity
 Inactivated Polio vaccine (IPV) DeveloperAlbert SabinJonas Salk Production Method Serial passage to attenuate strain (live) Formalin inactivated Tissue culture supernatant Costcheapexpensive RouteOralIM injection Type of immunity Produce good gut immunity Less robust gut immunity")
8
The vaccines Oral Polio vaccine (OPV) Inactivated Polio vaccine (IPV) Predictable immunity Erratic, affected by enteric disease Predictable, not affected by enteric disease Revert to neuro- virulence Reported. Recombination with other enteroviruses Not reported. Virus is inactivated VAPP*1 in 2.4-3.3 millionNot reported ProtectionContact immunityOnly vaccinated individual *VAPP = Vaccine associated paralytic poliomyelitis

9
Levels of epidemiological modification by vaccination Organism present ? Surveillance ? Vaccination ? ControlYes Low level Yes Required Yes Required EliminationImport only Yes Required Yes Required EradicationNo

10
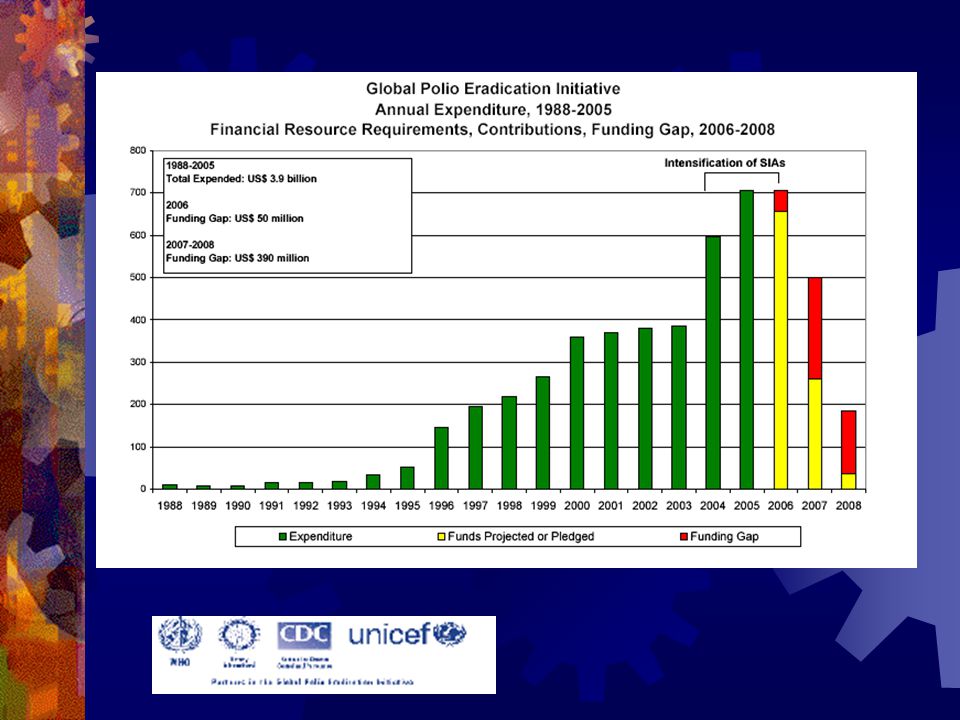
The campaign 1988 World Health Assembly passed a resolution to eradicate polio by 2000 The Global Polio Eradication Initiative was founded – Biggest Public health initiative to date Task: co-ordinate eradication of poliovirus globally and source funding

11
Global Status 1988 350 000 cases polio-1988 125 polio-endemic countries http://www.polioeradication.org/

12
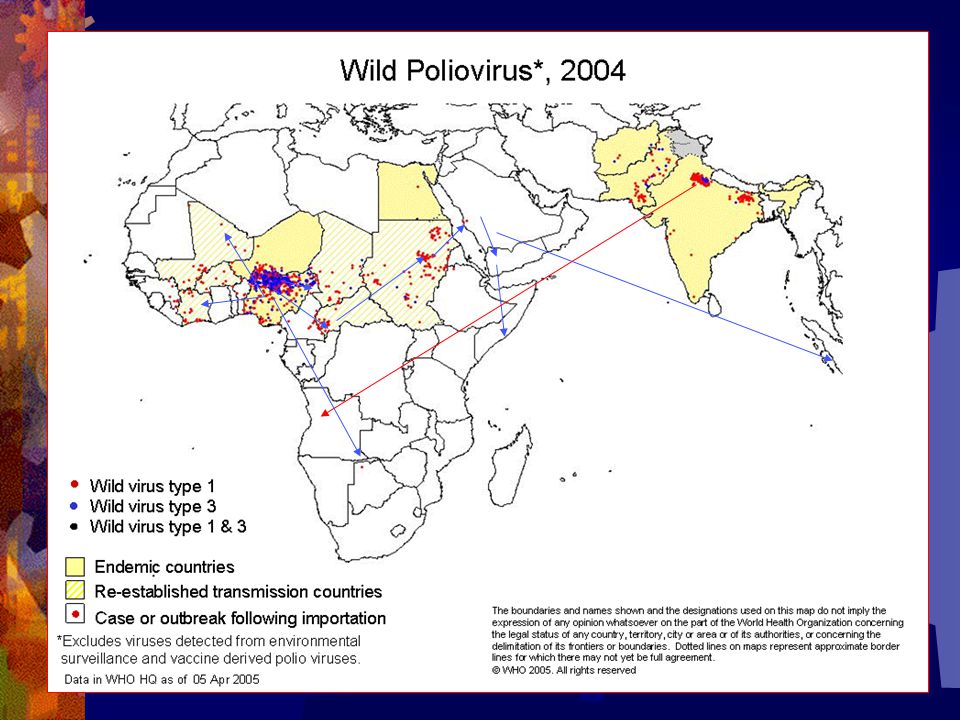
Global Status 2004 1,263 cases in 2004 (99% reduction in cases) 1000 childhood paralysis prevented per day 6 polio-endemic countries, 5 countries re-established transmission http://www.polioeradication.org
 1000 childhood paralysis prevented per day 6 polio-endemic countries, 5 countries re-established transmission")
13
Science 26 March 2005 vol 303

15
The challenges Funding gap Containing polio in endemic area Nigeria Uttar Pradesh and Bihar states in NE India Containing polio epidemics due to importation (Namibia) Vaccine derived polio viruses (VDPV) Laboratory containment
 Vaccine derived polio viruses (VDPV) Laboratory containment")
17
Polio endemic area Nigeria Overcoming political and religious resistence Vaccination campaign back on track India High intensity of polio transmission combined with high incidence of enteric disease Despite good coverage unable to interrupt transmission of polio Monovalent vaccine (response to single dose mOPV is >75% compare to tOPV 25%)
")
18
The Namibian experience Prior to the outbreak Started OPV 1990, coverage of 60-80% Last case of polio reported 1996 AFP surveillance: 2.6/100,000 and 86% stool collection rate (adequate) The outbreak: Index case May 2006 185 suspected cases 20 laboratory confirmed cases 21 deaths, ¾ are adult over 15 years Gaps in immunisation – a number of susceptible adults
 The outbreak: Index case May 2006 185 suspected cases 20 laboratory confirmed cases 21 deaths, ¾ are adult over 15 years Gaps in immunisation – a number of susceptible adults")
19
The Namibian experience Virus identified as poliovirus type 1 SOAS genotype Same strain as Angolan outbreak and NE states of India Molecular distance compare to parental strain is approximately 2.5 year Unclear whether imported from Angola or India

21
The Namibian experience Massive immunisation campaign targeting the entire population. Three national immunisation days. > 2 million doses of monovalent OPV1 administered Outbreak halted

22
The Namibian experience Lessons learned: Coverage needs to be >80% -Immunisation gap Importance of disease surveillance Traditional AFP surveillance on children <15 yo is inadequate marker of polio elimination Importance of laboratory network and regional reference laboratory Constant risk of importation Political will – immunisation campaigns

23
VDPV (Vaccine derived polio virus) <1% VP1 genetic divergence = vaccine strain (Sabin-like virus) 1-15% VP1 genetic divergence = Vaccine derive polio virus (VDPV) cVDPV (evidence of circulation in the communities) iVDPV (chronically shed by immunocompromised individuals) >15% VP1 genetic divergence = wild polio virus 99 85 OPV genome
 <1% VP1 genetic divergence = vaccine strain (Sabin-like virus) 1-15% VP1 genetic divergence = Vaccine derive polio virus (VDPV) cVDPV (evidence of circulation in the communities) iVDPV (chronically shed by immunocompromised individuals) >15% VP1 genetic divergence = wild polio virus OPV genome")
24
The laboratory containment A country cannot be certified as polio free unless all laboratories are free of poliovirus If 1 country is not certified polio free, polio cannot be eradicated Potential sources polio outbreak: Stored stool specimen, past poliovirus isolates, polio vaccine manufacturing facility Past enteric pathogen research specimen Past environmental surveillance (water) samples Past respiratory specimen (routine/research) The “mystery” vial / Legacy of previous research in the –70 freezer
 samples Past respiratory specimen (routine/research) The mystery vial / Legacy of previous research in the –70 freezer")
25
Is it possible to eradicate polio? It is possible and it has to be done Prevent re-emergence of polio we need to: Keep vaccinating with routine EPI and various campaigns Good acute flaccid paralysis surveillance Rid the laboratory of wild and vaccine poliovirus Stop using OPV in the final phase of polio eradication Thank you

Similar presentations




















 but no new district in India Most recent date of onset 03 Oct 1 case (W1) but.>")
