Download presentation
Presentation is loading. Please wait.

1
Learning Session 1 Cape Town, February 2011

2
To reduce Healthcare Associated Infection (HAI) using a Systems Improvement approach Overall goal of BCA Campaign
 using a Systems Improvement approach Overall goal of BCA Campaign")
3
How are you doing so far? How are you doing with Overall Progress Measurement Team work

4
Make your mark! Overall Progress Measurement Team work Excellent Not good Fair 0 5 10

5
Make your mark! Overall Progress Measurement Team work Excellent Not good Fair 0 5 10

6
Gauteng BCA Learning Network

8
Biggest challenges Leadershi p invloveme nt Understan ding the bundles Implement ing bundles Diagnosin g the infection measure ment Feeding back progress Team work Mentoring and support

9
Biggest challenges x xx xxxx xxxx xxxxxxxx Leadershi p involveme nt Understan ding the bundles Implement ing bundles Diagnosin g the infection measure ment Feeding back progress Team work Mentoring and support

10
Will Ideas Execution What we need for success

11
Why spend our time and energy reducing Healthcare Associated Infections? Building Will The business case

12
Patients get “recommended care” ~ 50% of the time. Adverse events occur in 10% of hospital patients. –50% are preventable. –7.5% of these patients die....the gap between evidence and practice 12 NEJM 2003; 348:2635-2645 Qual Safety in Health Care 2008;17:216-223

13
Healthcare-Associated Infection –Infection rates 5-10% –1.4 million patients affected each day –USA 100,000 deaths, $6.5 billion / yr JAMA 2009;301(12):1285-1287 Lancet 2008;372(9651):1719-1720 13
: Lancet 2008;372(9651):")
14
Delegate Survey, FIDSSA Conference Aug 20-23 2009 85.1% In the hospital(s) with which I am associated… 14
 with which I am associated… 14")
15
Allegranzi B. Burden of endemic health-care-associated infection in developing countries: systematic review and meta- analysis. Lancet Dec 2010. Number of HAI studies 1995-2008 15

16
Healthcare-associated infections are 2-3 x more common in developing countries 16 Allegranzi B. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet Dec 2010.

17
SA Hospitals? –9.7% HAI point prevalence –28.6% in ICU Prof A Duse. SA-HISC study (unpublished) 17 Private + Public Hospitals in Gauteng
 17 Private + Public Hospitals in Gauteng.")
18
1 in 7 patients who enter SA Hospitals are at risk for developing an HAI Brink A et al., SAMJ 2006; 96(7) 18
 18")
19
HAI Impact On the patient & family On you? On the hospital? Financial? 19

20
IHI and others wondered if something could be done IHI (US) 100,000 lives campaign – 6 interventions including 3 of ours Canadian Safer Healthcare Now Scotland NHS Patient Safety Alliance ….and other successes around the world
 100,000 lives campaign – 6 interventions including 3 of ours Canadian Safer Healthcare Now Scotland NHS Patient Safety Alliance ….and other successes around the world")
21
Interventions were made into bundles What is a bundle and how does it work? A grouping of best practices that individually improve care, but when applied together result in substantially greater improvement. The science behind the bundle is so well established that it should be considered standard of care. Bundle elements are dichotomous and compliance can be measured: yes/no answers. Bundles shun the piecemeal application of proven therapies in favor of an “all elements” approach.

22
What was achieved when the bundles were implemented reliably i.e. all elements of the bundle to every patient every time?

23
Results…Michigan (Keystone) 66% reduction in line-related infection Saved > 1,500 lives Saved $200 million in 18 months New England Journal of Medicine. 2006; 355(26): 2725-2732 23
:")
24
24

25
HAI : SSI RATE 25

26
26

27
Why BCA? Better care, less harm Build the capacity to improve 27

28
Learning together 28

29
29

30
30 Finding leverage and synergy to achieve sustainable, high quality health care …more quickly …at greater scale Power of leverage and synergy Leverage: doing something smart that has a much bigger impact. Synergy: two or more people produce more together than the sum of what they could have produced separately. 30

31
Will Ideas Execution What we need for success

32
4 infection prevention bundles VAP (ventilator associated pneumonia) CLABSI (central line associated bloodstream infection) SSI (surgical site infections) CAUTI (catheter associated urinary tract infections) Ideas for improvement
 CLABSI (central line associated bloodstream infection) SSI (surgical site infections) CAUTI (catheter associated urinary tract infections) Ideas for improvement")
33
The size of the challenge at your facility Ventilato rs Central lines Surgical Sites Urinary Catheter s Unit 1 Unit 2 Unit 3 Unit 4 Exercise: i) mark the procedures relevant to each of your ICU or high care units with an ‘X’. ii) Prioritise the intervention most relevant to each unit by circling one of the X’s in each unit
 Prioritise the intervention most relevant to each unit by circling one of the X’s in each unit.")
34
The challenge at your facility Ventilator s Central lines Surgical Sites Urinary Catheter s ICUXXXX TheatreXXX High CareXXXX Medical Ward XX Surgical Ward XX Emergency Unit XX Exercise: i) mark the procedures relevant to each of your ICU or high care units with an ‘X’. ii) Prioritise the intervention most relevant to each unit by circling one of the X’s in each unit
 Prioritise the intervention most relevant to each unit by circling one of the X’s in each unit.")
35
Will Ideas Execution What we need for success

36
Learning Network Learning session 1 © Institute for Healthcare Improvement Learning session 2 Activity phase: Activity phase: Learning session 3 18 -24 months Support, support, support preparation

37
Make it do-able Prioritise ONE bundle/ or aspect of the problem size of the problem size of the impact leadership preference Start small then build up as you gain confidence one ICU/high care small improvement team one aspect of the bundle expand as confidence grows (data) Start where you’ll get the best results the most support
 Start where you’ll get the best results the most support")
38
Start small to gain confidence i) Choose one intervention bundle that will have the greatest effect ii) Choose one unit where you have the greatest chance of success iii) Who will you have on your team? Ventilator s Central lines Surgical Sites Urinary Catheter s ICUXXXX TheatreXXX High CareXXXX Medical Ward XX Surgical Ward XX Emergency Unit XX Exercise:

39
Choosing the improvement team Late Majority Early Majority Early Adopters Tradition- alists Innovators 2% 13%35% 15%

40
Getting Started Kit Team Exercise: i) look up the elements of your selected ‘Bundle’ ii) What reduction in the level of infection has been achieved using the bundle you selected ? Adult Ventilator Associated Pneumonia pg 9 & 10 Central Line Associated Bloodstream Infections pg 8 & 9 Surgical Site Infections Catheter Associated Urinary Tract Infection pg 5 & 6

41
Know where you’re heading What’s Possible with the bundles? 1.Adult Ventilator Associated Pneumonia Average 45% reduction. With every bundle element every time – Zero cases for over long periods of time (pg 7) 2. Central Line Associated Blood Stream Infections Nearly eliminate CLABSI (pg 7&8) 3. Surgical Site Infections (incidence in clean cases 2-3% USA) 40 – 60 % infections are preventable (pg 6) 4. Catheter Associated Urinary Tract Infection Reductions of 46% - 81% have been achieved (pg 6)
 2. Central Line Associated Blood Stream Infections Nearly eliminate CLABSI (pg 7&8) 3. Surgical Site Infections (incidence in clean cases 2-3% USA) 40 – 60 % infections are preventable (pg 6) 4. Catheter Associated Urinary Tract Infection Reductions of 46% - 81% have been achieved (pg 6).")
42
Define an Aim (for your bundle) must have a number must have a time frame must stretch you - not achievable in the current system - requires change benchmark against what has been achieved elsewhere Statement of where you want to go - you don’t need to know how to get there yet
 must have a number must have a time frame must stretch you - not achievable in the current system - requires change benchmark against what has been achieved elsewhere Statement of where you want to go - you don’t need to know how to get there yet")
43
Defining the Aim To reduce (VAP, CLA-BSI, SSI, CA-UTI) By ……………. amount By implementing the whole ………bundle to every patient every time By August 2012 (in 18 months)
.")
44
A systems approach

45
12/2008 Understanding Systems 1)choose two people in the room, don’t tell them who they are 2) one of them must be a person selected by the facilitator 3) keep the same distance between yourself and each of the two people you have chosen
choose two people in the room, don’t tell them who they are 2) one of them must be a person selected by the facilitator 3) keep the same distance between yourself and each of the two people you have chosen")
46
Complete each of the steps in this process Step 1: Pick a number from 3 to 9 Step 2: Multiply your number by 9 Step 3: Add 12 to the number from step 2 Step 7: Write down the name of a city that begins with your letter Step 4: Add your 2 digits together Step 5: Divide # from step 4 by 3 to get a 1 digit number Step 6: Convert your Number to a letter: 1=A 2=B 3=C 4=D 5=E 6=F 7=G 8=H 9 = I Step 8: Go to the next Letter: A to B, B to C, C to D, etc. Step 9: Write down the name of an animal (not bird, fish, or insect) that begins with your letter from Step 8 Step 10: Write down the color of your animal Do you have a 2-digit Number? NO YES Output: Color____________ Animal___________ City__________
 that begins with your letter from Step 8 Step 10: Write down the color of your animal Do you have a 2-digit Number. NO YES Output: Color____________ Animal___________ City__________.")
47
“Every system is perfectly designed to achieve the result it gets” 12/2008

48
‘Every improvement needs a change’ The changes: 1)Infection Control Bundles 1)A way of overcoming the implementation gap Every element of the bundle To every patients Every time
Infection Control Bundles 1)A way of overcoming the implementation gap Every element of the bundle To every patients Every time")
49
I The Implementation Gap PLAN IMPLEMENT FAIL PROBLEM EVIDENCE BASED SOLUTION “traditional” attempts to change

50
I DO STUDY ACT IMPLEMENT SUCCEED/ SUSTAIN Overcoming the Implementation Gap GREAT IDEAS SYSTEM ANALYSIS to identify barriers to care PROBLEM PLAN

51
‘Every improvement needs a change Not every change is an improvement’

52
Rapid Cycle Change –start small on one part of the bundle/system PLAN DO STUDY ACT PLAN DO STUDY ACT PLAN DO STUDY ACT

53
Improving many parts of the bundle/system at once. PLA N DO STU DY ACT PLA N DO STU DY ACT PLA N DO STU DY ACT part 3 part 4 part 1 part 2 PLA N DO STU DY ACT PLA N DO STU DY ACT PLA N DO STU DY ACT PLA N DO STU DY ACT PLA N DO STU DY ACT PLA N DO STU DY ACT PLA N DO STU DY ACT PLA N DO STU DY ACT PLA N DO STU DY ACT

54
Model for Improvement What can we change that will result in an improvement? PLAN DO STUDY ACT How will we know that a change is an improvement ? What are we trying to accomplish? AIM MEASUREMENTCHANGE

55
Measurement Are we getting closer to our target? Outcome measure

56
Measurement Did we use the whole bundle in every patient every time? Process measure (Bundle compliance)
.")
57
Measurement Was the change an improvement? Measuring the impact of a change

58
Measuring over time a volunteer to write a volunteer to measure graph paper

59
Annotated Run Chart Community Need I Change Made in June

60
Interpreting Data: what is the story? I Before (Feb) After (Aug)
 After (Aug)")
61
What is the real story? Change Made Change Made in June FebAug FebAug FebAug FebAug FebAug I Change Made

63
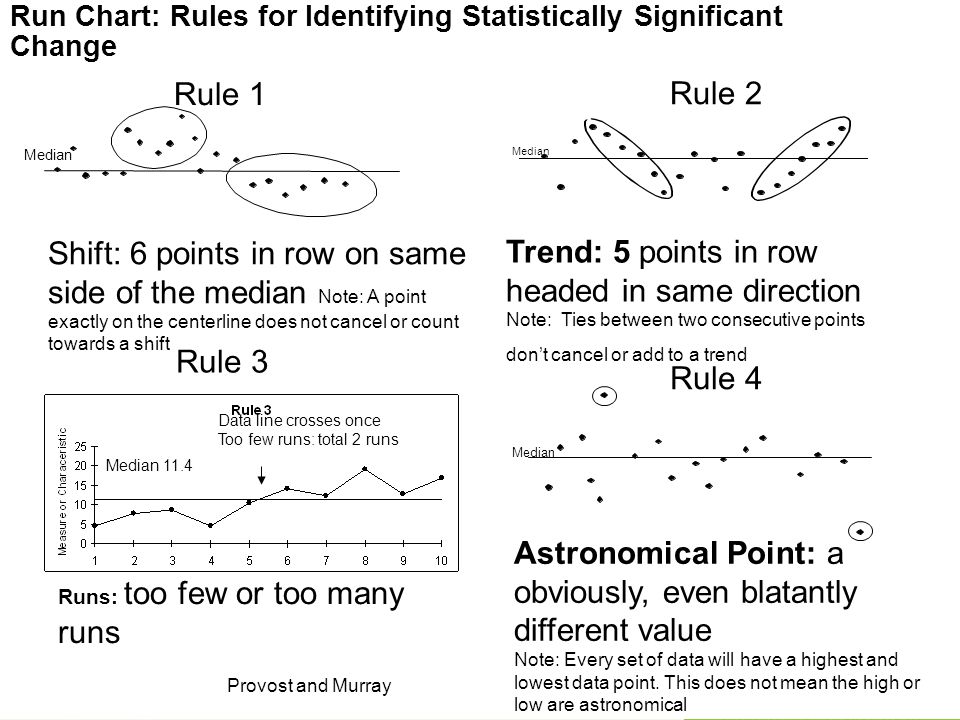
Run Charts One of the most powerful tools for improvement Describe a process over time Shows trends the process is experiencing Can be used to analyse whether the change was an improvement Data can be used to drive change

64
Outcome measurement Are we getting to our target? Was the change an improvement? How do we measure HAIs?

65
Measuring infection rates Lessons from an ICU

66
Quality Improvement 101 Problem?

67
Measuring Infection Rates Total number of infective cases per 1,000 device days: Total No. of VAP cases Ventilator days X 1,000 Numerator Denominator

68
Definition of VAP “VAP is suspected when a patient on mechanical ventilation develops: a new or progressive pulmonary infiltrate with fever / leucocytosis and purulent tracheobronchial secretions” “Pneumonia is considered as ventilator associated if the patient was intubated and ventilated at the time or within 48hrs before the onset of the infection”

69
Overcoming Numerator Issues Total No. of VAP cases Ventilator days X 1,000 Numerator Denominator

70
Overcoming Numerator Issues Checklists for Diagnosing the HA Infection used by the team

71
Overcoming Denominator Issues At the same time every day the Unit manager counts devices in use in the ward

72
Additional Tools

73
Measuring HAI Percentages and rates % (or rate) = Numerator/ denominator eg Rate of infection = readmissions for septic caesarian section wounds per week / number of Caesarian Sections performed per week Rate of infection = Number of VAP / 1000 device days
 = Numerator/ denominator eg Rate of infection = readmissions for septic caesarian section wounds per week / number of Caesarian Sections performed per week Rate of infection = Number of VAP / 1000 device days")
74
Safety Calendar Welsh 1000 lives campaign I Developed by Annette Bartley

75
Welsh Patient Safety Project

76
Measuring HAI The concept of ‘days between’ infections For measure ‘rare’ events (occur < 10%)
")
77
Off the internet, Google pictures

79
Off the internet, Google pictures

80
Off the internet, Google pictures

81
Maternal deaths – Malawi For the “NO Maternal Death” Campaign a colorful, laminated A4 paper that said “Days without a Maternal Death: ______”. were hung in every Labour Ward for all (providers, patients and guardians) to see and the number was filled in daily with a dry erase marker
 to see and the number was filled in daily with a dry erase marker.")
82
Days between icecreams Days between icecream Icecream 1st2nd3rd4th5th 5 10 15 20 25

83
Days between events (infection) Days Between events (eg Infection) Sequence of events (eg Infection) 1st2nd3rd4th5th 5 10 15 20 25
 Days Between events (eg Infection) Sequence of events (eg Infection) 1st2nd3rd4th5th")
84
Neonatal deaths – Malare Health Centre, 5’s Alive! Project, Ghana I

85
I Measuring rare events and time-between measures. James Benneyan IHI

86
JulyAugSepOct 5/713/87/95/10 5/79/98/10 6/712/915/10 11/715/919/10 25/720/10 27/721/10 25/10 ICU: Sequence of VAP infections by date 2010

87
Use the tools to Display the data JulyAugSepOct 5/713/87/95/10 5/79/98/10 6/712/915/10 11/715/99/10 25/720/10 27/721/10 25/10

88
Date of infection # Days since last infection Days Be- tween Infecti on Sequence of Infections

89
So far we have: 1.Mapped the size of the project in your facility 2.Prioritise a unit and bundle to start with 3.Written an aim

90
Now, write down: 1.Your aim 2.The outcome measures i)Rate = numerator/denominator (describe) ii)Days between iii) Welsh Safety calendar iv) Other 3.How you will feedback the data every month to i)The frontline staff ii)Management Mark with a * areas that you want to strengthen
Rate = numerator/denominator (describe) ii)Days between iii) Welsh Safety calendar iv) Other 3.How you will feedback the data every month to i)The frontline staff ii)Management Mark with a * areas that you want to strengthen")
91
Improving your Outcome Measure 1) Numerator Standardised diagnosis of infection 2) What is the measure for HAI? Rate = Infection/device day Days between (CLABSI, VAP, UTI) Days or cases between SSI 3) Collecting and collating data: What (definition)/ Where/ How (tools)/ Who/ When 4) Presenting the data: Format - Safety Cross, Graphs Feedback/presentation - Management platform
 Days or cases between SSI 3) Collecting and collating data: What (definition)/ Where/ How (tools)/ Who/ When 4) Presenting the data: Format - Safety Cross, Graphs Feedback/presentation - Management platform.")
92
PDSA –testing a change MARU What is Maru trying to achieve? How many ideas does he try? Is he successful? What was the possible negative outcome? From YouTube

93
Rapid Cycle Change What can we change that will result in an improvement? PLAN DO STUDY ACT How will we know that a change is an improvement? What are we trying to accomplish? PLAN DO STUDY ACT PLAN DO STUDY ACT PLAN DO STUDY ACT

94
AIM of this change: PROBLEM :

95
AIM: make our project and outcome measure ‘visible’ in the ward PROBLEM : our staff are not engaged in the project Use the Welsh Safety Cross

96
AIM of this change: HOMEWORK Do a PDSA to solve a problem at home

Similar presentations









: Baseline incidence rate - 4.5% Nutritional assessment - 50% Pressure.>")










