Download presentation
Presentation is loading. Please wait.

1
www.tri-london.ac.uk The GARFIELD Registry is funded by an unrestricted research grant from Bayer Pharma AG Alexander G G Turpie Professor Emeritus of Medicine McMaster University Hamilton ON Canada Future Challenges

2
Disclosures for Dr A.G.G. Turpie Research SupportNone EmployeeNone Consultant and/or Honoraria Bayer HealthCare, Boehringer-Ingelheim, Bristol-Myers Squibb, Johnson and Johnson, Sanofi-Aventis, Takeda, Portola StockholderNone Speakers BureauPfizer, GSK Scientific Advisory Board Bayer HealthCare, Johnson and Johnson,

4
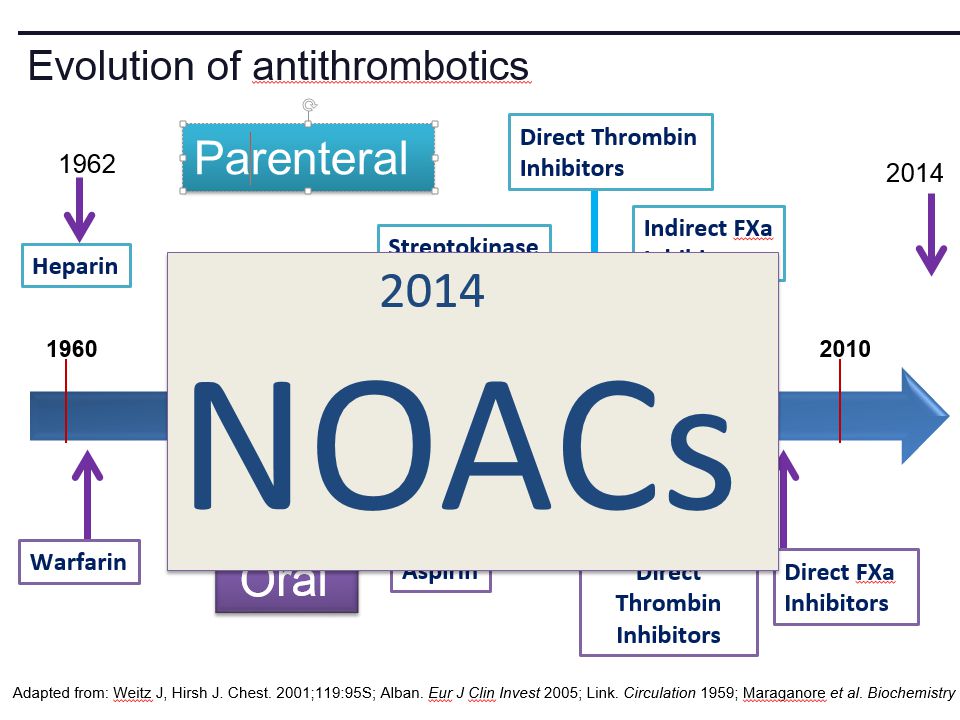
New anticoagulants Direct Thrombin Inhibitors - Dabigatran Factor Xa Inhibitors - Rivaroxaban - Apixaban - Edoxaban

5
Future challenges Management of bleeding - Prevention - Treatment Measurement Antidotes

6
All anticoagulants can cause bleeding

7
Bleeding in VKA anticoagulated patients Is common –Major bleeding 1-5% per year in AF –Intracranial bleeding 0.5-1.2% per year in AF Associated with adverse outcomes –3 to 5-fold increase in thrombotic events and death Rapid and timely control of bleeding is likely to improve clinical outcomes but the efficacy of anticoagulant reversal is unproven

8
Management of bleeding Prevention Treatment

9
Prevention of bleeding Anticoagulant selection Patient and dose selection Appropriate management of interruption

15
Perioperative Management of NOAC-treated Patients

16
Management of interruption of treatment DrugPatientProcedure Drug half-life Renal function Bleeding risk Route of clearance Concomitant drugs (e.g., aspirin) Thrombosis risk
 Thrombosis risk")
17
Creatinine clearance (CrCl) DabigatranApixabanRivaroxaban No important bleeding risk and/or adequate local haemostasis possible: Perform at trough level (i.e. 12 h or 24 h after last intake) Low riskHigh risk Low risk High risk Low risk High risk CrCl ≥80 ml/min≥24 h≥48 h≥24 h≥48 h≥24 h≥48 h CrCl 50-80 ml/min≥36 h≥72 h≥24 h≥48 h≥24 h≥48 h CrCl 30-50 ml/min*≥48 h≥96 h≥24 h≥48 h≥24 h≥48 h CrCl 15-30 ml/min* Not indicated ≥36 h≥48 h≥36 h≥48 h CrCl <15ml/minNo official indication for use Heidbuchel et al, 2013 *Many of these patients may be on lower dose of NOAC Low risk = surgery with low risk of bleeding, high risk = surgery with high risk of bleeding Last intake of drug before elective surgical intervention
 Low riskHigh risk Low risk High risk Low risk High risk CrCl ≥80 ml/min≥24 h≥48 h≥24 h≥48 h≥24 h≥48 h CrCl ml/min≥36 h≥72 h≥24 h≥48 h≥24 h≥48 h CrCl ml/min*≥48 h≥96 h≥24 h≥48 h≥24 h≥48 h CrCl ml/min* Not indicated ≥36 h≥48 h≥36 h≥48 h CrCl <15ml/minNo official indication for use Heidbuchel et al, 2013 *Many of these patients may be on lower dose of NOAC Low risk = surgery with low risk of bleeding, high risk = surgery with high risk of bleeding Last intake of drug before elective surgical intervention.")
18
ProcedureAction Procedures with immediate and complete haemostasis: Atraumatic spinal/ epidural anaethesia Clean lumbar puncture Resume 6–8 h after surgery Procedures associated with immobilization Initiate reduced venous or intermediate dose of LMWH 6– 8 h after surgery if haemostasis achieved Procedures with post-operative risk of bleeding Restart NOACs 48–72h after surgery upon complete haemostasis Thromboprophylaxis (e.g. with LMWH) can be initiated 6-8 h after surgery Heidbuchel et al, 2013 Resumption of NOAC
 can be initiated 6-8 h after surgery Heidbuchel et al, 2013 Resumption of NOAC.")
19
Monitoring vs measuring Monitoring implies dose adjustment according to test result Measuring the drug or drug effect may be useful in: Bleeding Overdosage Questions of compliance Urgent surgery, interventions, thrombolysis Extreme body weights Children Renal insufficiency

20
Measurement of anticoagulant effects of NOACs TestDabigatranRivaroxabanApixaban Specific Assay HemoclotAnti-Xa Non-specific assays aPTT ↑↑↑↑↑ PT ↑↑↑↑ TT ↑↑↑↑ No effect

21
Future Point of care testing

22
Management of VKA bleeding Hold drug(s) Vitamin K Resuscitation (i.v. access, fluid administration, blood product transfusion) Maintain diuresis to clear drug Mechanical compression and surgical methods to stop bleeding
 Maintain diuresis to clear drug Mechanical compression and surgical methods to stop bleeding.")
23
Replace clotting factors CharacteristicFrozen plasmaPCC ConstituentsAll clotting factorsII, (VII), IX, X (C, S) Dose10-15 ml/kg25-50 IU factor IX/kg OnsetDuration of infusion15-30 min Adverse effects Fluid overload, febrile & allergic reactions, infection, TRALI Possible excess thromboembolic complications Other Vitamin K to sustain reversal* Vitamin K to sustain reversal* Quinlan D, et al. Circulation 2013; 128:1179-81. *Half life of factor VII is 6 hours

24
Frozen plasma or PCC? Sarode R, et al. Circulation 2013; 128:1234-1243.

25
Management of NOAC bleeding Hold drug(s) No Vit K Resuscitation (i.v. access, fluid administration, blood product transfusion) Maintain diuresis to clear drug Mechanical compression and surgical methods to stop bleeding
 Maintain diuresis to clear drug Mechanical compression and surgical methods to stop bleeding.")
26
Reversal of NOACs Activate coagulation to overcome the effect of the drug Remove drug Neutralize drug Lauw MN, et al. Can J Cardiol. 2014;30:381-384.

27
Activate coagulation Recombinant factor VIIa (rVIIa) Prothrombin complex concentrates (PCC) –II, VII, IX, X, C, S, –25-50 units per kg Activated prothrombin complex concentrates (aPCC) Antifibrinolytic agents (e.g., tranexamic acid)
 Prothrombin complex concentrates (PCC) –II, VII, IX, X, C, S, –25-50 units per kg Activated prothrombin complex concentrates (aPCC) Antifibrinolytic agents (e.g., tranexamic acid)")
28
Effect of NOACs on prothrombin time and endogenous thrombin potential with PCC

29
Prothrombin time (PT) Endogenous thrombin potential (ETP) Eerenberg et al, 2011 PCC demonstrated the potential to reverse rivaroxaban effects on PT and ETP in humans Rivaroxaban: Effect on prothrombin time and endogenous thrombin potential with PCC
 Endogenous thrombin potential (ETP) Eerenberg et al, 2011 PCC demonstrated the potential to reverse rivaroxaban effects on PT and ETP in humans Rivaroxaban: Effect on prothrombin time and endogenous thrombin potential with PCC")
30
Antidotes to anticoagulants Bleeding Emergency Intervention Elective Intervention Overdose

31
Specific antidotes to NOACs IdarucizumabPER977 Andexanet alpha Structure Humanized Fab fragment Synthetic small molecule Human rXa variant TargetDabigatranUniversalFXa inhibitors Binding Non-competit. High affinity ?Competitive Clinical studies Rapid complete reversal ? Rapid, near complete reversal Lauw M, et al. Can J Cardiol 2014 (accepted).
..")
32
Andexanet Alpha - Phase 2 clinical study overview Double blind, randomized 2:1 (9 healthy subjects per cohort) Factor Xa Inhibitor Days 1-6 (to steady state) PRT064445/ Placebo IV PRT064445/ Placebo IV Day 6 3h after last fXa inhibitor dose Study 1: Apixaban 5 mg PO Q12 Study 2: Rivaroxaban 20 mg PO QD Study 3: Enoxaparin 1 mg/kg SQ Q12 Study 4: Betrixaban 80 mg PO QD Study 5: Edoxaban TBD Study 1 - Apixaban Cohort 1: 90 mg IV x 1 Cohort 2: 210 mg IV x 1 Cohort 3: 420 mg IV x 1 Cohort 4: TBD Checkout Inpatient Unit Last Safety f/u Last Safety f/u Day 13Day 48
 Factor Xa Inhibitor Days 1-6 (to steady state) PRT064445/ Placebo IV PRT064445/ Placebo IV Day 6 3h after last fXa inhibitor dose Study 1: Apixaban 5 mg PO Q12 Study 2: Rivaroxaban 20 mg PO QD Study 3: Enoxaparin 1 mg/kg SQ Q12 Study 4: Betrixaban 80 mg PO QD Study 5: Edoxaban TBD Study 1 - Apixaban Cohort 1: 90 mg IV x 1 Cohort 2: 210 mg IV x 1 Cohort 3: 420 mg IV x 1 Cohort 4: TBD Checkout Inpatient Unit Last Safety f/u Last Safety f/u Day 13Day 48")
33
Mean ± SEM Anti-fXa activityApixaban free fraction Dose-dependent reversal of Apixaban-induced Anti-FactorXa activity correlates with reduction in Apixaban plasma free fraction

34
Andexanet Alpha FDA designated breakthrough therapy Phase III Clinical Trials - ANNEXA-A: apixaban - ANNEXA-R: rivaroxaban

35
Conclusions NOACs provide opportunity to minimize growing burden of potentially preventable thromboembolism (especially AF) Reductions in both stroke and bleeding translate into important benefits for patients Most bleeding can be managed without specific antidotes Specific antidotes in development will provide reassurance to physicians Education to overcome the fear of bleeding as a barrier to appropriate anticoagulant use important
 Reductions in both stroke and bleeding translate into important benefits for patients Most bleeding can be managed without specific antidotes Specific antidotes in development will provide reassurance to physicians Education to overcome the fear of bleeding as a barrier to appropriate anticoagulant use important")
Similar presentations






: New Advances and Trends 28 February 2015 Scott Kaatz, DO, MSc, FACP,>")








 Apixaban (oral) Betrixiban (oral) Edoxaban (oral)>")








