Download presentation
Presentation is loading. Please wait.

1
Multidisciplinary approaches on chest tumors Radiation Oncology Case Reports

2
Name: A. E. DOB: 1942 Metastatic NSCLC T1 N2 M1 G3 History: Metastatic NSCLC (diagnosis 2000) - initial stage T1 N2 M1(multiple tumors in different lobes RUL 3 cm, RLL 2 cm, multilevel N2 )
 - initial stage T1 N2 M1(multiple tumors in different lobes RUL 3 cm, RLL 2 cm, multilevel N2 ).")
3
Name: A. E. DOB: 1942 Metastatic NSCLC T1 N2 M1 G3 History: Metastatic NSCLC (diagnosis 2000) - initial stage T1 N2 M1(multiple lung tumors in different lobes) - 6 cycles Carboplatin/Navelbine 2000 - mediastinal tumor progression 2001. no further treatment - clinical and radiological progression with SOB 2005
 - initial stage T1 N2 M1(multiple lung tumors in different lobes) - 6 cycles Carboplatin/Navelbine mediastinal tumor progression no further treatment - clinical and radiological progression with SOB")
4
Name: A. E. DOB: 1942 Metastatic NSCLC T1 N2 M1 G3 History: Metastatic NSCLC (diagnosis 2000) - initial stage T1 N2 M1(multiple lung tumors in different lobes) - 6 cycles Carboplatin/Navelbine 2000 - mediastinal tumor progression 2001. no further treatment - clinical and radiological progression with SOB 2005 - Tarceva 05-09/05, - PD (lung parenchyma) Status: current problems:a) post-stenotic pneumonia b) singular brain metastasis right parietal with perifocal oedema
 - initial stage T1 N2 M1(multiple lung tumors in different lobes) - 6 cycles Carboplatin/Navelbine mediastinal tumor progression no further treatment - clinical and radiological progression with SOB Tarceva 05-09/05, - PD (lung parenchyma) Status: current problems:a) post-stenotic pneumonia b) singular brain metastasis right parietal with perifocal oedema.")
5
Name: A. E. DOB: 1942 Metastatic NSCLC T1 N2 M1 G3 History: Metastatic NSCLC (diagnosis 2000) - initial stage T1 N2 M1(multiple lung tumors in different lobes) - 6 cycles Carboplatin/Navelbine 2000 - mediastinal tumor progression 2001. no further treatment - clinical and radiological progression with SOB 2005 - Tarceva 05-09/05, - september PD (lung parenchyma) Status: current problems:a) post-stenotic pneumonia b) singular brain metastasis right parietal with perifocal oedema Radiotherapy Concept:
 - initial stage T1 N2 M1(multiple lung tumors in different lobes) - 6 cycles Carboplatin/Navelbine mediastinal tumor progression no further treatment - clinical and radiological progression with SOB Tarceva 05-09/05, - september PD (lung parenchyma) Status: current problems:a) post-stenotic pneumonia b) singular brain metastasis right parietal with perifocal oedema Radiotherapy Concept:.")
6
Name: A. E. DOB: 1942 Metastatic NSCLC T1 N2 M1 G3 History: Metastatic NSCLC (diagnosis 2000) - initial stage T1 N2 M1(multiple lung tumors in different lobes) - 6 cycles Carboplatin/Navelbine 2000 - mediastinal tumor progression 2001. no further treatment - clinical and radiological progression with SOB 2005 - Tarceva 05-09/05, - september PD (lung parenchyma) Status: current problems:a) post-stenotic pneumonia b) singular brain metastasis right parietal with perifocal oedema Radiotherapy Concept: a) palliative RT to mediastinum and primary lung tumour with 10 x 3 Gy b) whole brain radiotherapy with 10 x 3 Gy followed by a boost of 2 x 3 Gy to the singular metastasis (4 fractions a week)
 - initial stage T1 N2 M1(multiple lung tumors in different lobes) - 6 cycles Carboplatin/Navelbine mediastinal tumor progression no further treatment - clinical and radiological progression with SOB Tarceva 05-09/05, - september PD (lung parenchyma) Status: current problems:a) post-stenotic pneumonia b) singular brain metastasis right parietal with perifocal oedema Radiotherapy Concept: a) palliative RT to mediastinum and primary lung tumour with 10 x 3 Gy b) whole brain radiotherapy with 10 x 3 Gy followed by a boost of 2 x 3 Gy to the singular metastasis (4 fractions a week).")
7
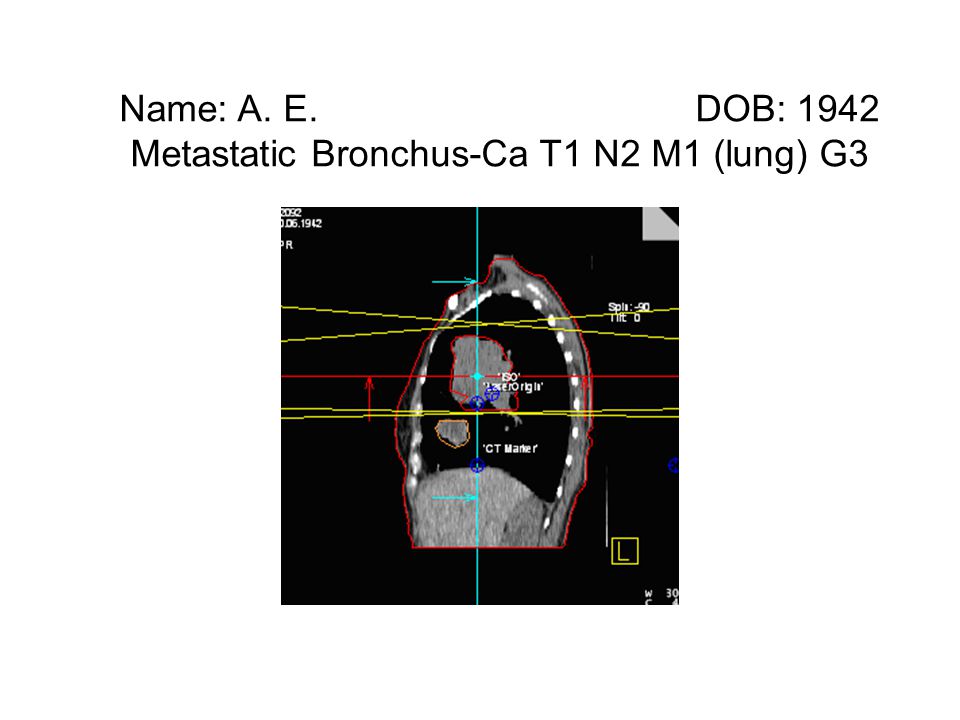
Name: A. E. DOB: 1942 Metastatic Bronchus-Ca T1 N2 M1 (lung) G3 PTV-Standard: a) tumour mass (PT and involved LyN-regions) + 1cm margin in all directions b) whole brain homogenous; boost to brain metastasis with a 2cm margin including tumour oedema Deviation from standards / Reason: a) due to the large treatment volume a compromise of the PTV was made for better lung protection -> Not all visible parenchymal tumour lesions included b) no deviation Case discussion could include role of radiation for brain metastases: Armstrong JG., JCO, 1994.Treatment of brain metastasis. Mintz AP., JAMA, 1998.Postoperative radiotherapy in single brain metastases. Patchell RA., JAMA, 1998.Controversies in management of brain metastases. Chan AW., Cancer, 2001.Review of initial management of brain metastases. Sneed PK., Radiat Oncol Biol Phys, 2002. Status at last f/u (5 months after tt): Primary tumor: „PR“/minor response (-50% atelectatic areas and tumor) on Chest X-Ray, no local clinical sy. Brain metastases: no clinical symptoms, no steroids needed, no CT-Scan performed
 G3 PTV-Standard: a) tumour mass (PT and involved LyN-regions) + 1cm margin in all directions b) whole brain homogenous; boost to brain metastasis with a 2cm margin including tumour oedema Deviation from standards / Reason: a) due to the large treatment volume a compromise of the PTV was made for better lung protection -> Not all visible parenchymal tumour lesions included b) no deviation Case discussion could include role of radiation for brain metastases: Armstrong JG., JCO, 1994.Treatment of brain metastasis. Mintz AP., JAMA, 1998.Postoperative radiotherapy in single brain metastases. Patchell RA., JAMA, 1998.Controversies in management of brain metastases. Chan AW., Cancer, 2001.Review of initial management of brain metastases. Sneed PK., Radiat Oncol Biol Phys, Status at last f/u (5 months after tt): Primary tumor: „PR /minor response (-50% atelectatic areas and tumor) on Chest X-Ray, no local clinical sy. Brain metastases: no clinical symptoms, no steroids needed, no CT-Scan performed.")
8
Name: A. E. DOB: 1942 Metastatic Bronchus-Ca T1 N2 M1 (lung) G3
 G3")
13
Name: B. H. DOB: 1941 SCLC extensive disease Diagnosis / Histology: SCLC of the right lower lobe (diagnosis in 2006) - extensive disease (multilevel, bilateral, med. lymph nodes; 1 (2 cm) metastases left liver lobe)
 - extensive disease (multilevel, bilateral, med. lymph nodes; 1 (2 cm) metastases left liver lobe).")
14
Name: B. H. DOB: 1941 SCLC extensive disease Diagnosis / Histology: SCLC of the right lower lobe (diagnosis in 2006) - extensive disease (mediastinal lymph nodes, 1 livermetastases) - 6 cycles Carboplatin / Etopophos 6-9/06, PR after 3 cycles, progression after 6 cycles - 10/06: progression of mediastinal lymph nodes and intrapulmonary tumour
 - extensive disease (mediastinal lymph nodes, 1 livermetastases) - 6 cycles Carboplatin / Etopophos 6-9/06, PR after 3 cycles, progression after 6 cycles - 10/06: progression of mediastinal lymph nodes and intrapulmonary tumour.")
15
Name: B. H. DOB: 1941 SCLC extensive disease Diagnosis / Histology: SCLC of the right lower lobe (diagnosis in 2006) - extensive disease (mediastinal lymph nodes, 1 metastases in liver) - 6 cycles Carboplatin / Etopophos 6-9/06, PR after 3 cycles, progression after 6 cycles - 10/06: progression of mediastinal lymph nodes and intrapulmonary tumour Status: Current problems:locoregional tumor progression
 - extensive disease (mediastinal lymph nodes, 1 metastases in liver) - 6 cycles Carboplatin / Etopophos 6-9/06, PR after 3 cycles, progression after 6 cycles - 10/06: progression of mediastinal lymph nodes and intrapulmonary tumour Status: Current problems:locoregional tumor progression.")
16
Name: B. H. DOB: 1941 SCLC extensive disease Diagnosis / Histology: SCLC of the right lower lobe (diagnosis in 2006) - extensive disease (mediastinal multilevel, bilaterla lymph nodes, 1 metastases in liver) - 6 cycles Carboplatin / Etopophos 6-9/06, PR after 3 cycles, progression after 6 cycles - 10/06: progression of mediastinal lymph nodes and intrapulmonary tumour Status: Current problems:locoregional tumor progression Radiotherapy Concept: RT of the mediastinum and the primary lung tumor with 22 x 1.8 Gy = 39.6 Gy followed by 10 x1.8Gy = 18 Gy without spinal cord. Total dose 59.6 Gy.
 - extensive disease (mediastinal multilevel, bilaterla lymph nodes, 1 metastases in liver) - 6 cycles Carboplatin / Etopophos 6-9/06, PR after 3 cycles, progression after 6 cycles - 10/06: progression of mediastinal lymph nodes and intrapulmonary tumour Status: Current problems:locoregional tumor progression Radiotherapy Concept: RT of the mediastinum and the primary lung tumor with 22 x 1.8 Gy = 39.6 Gy followed by 10 x1.8Gy = 18 Gy without spinal cord. Total dose 59.6 Gy..")
17
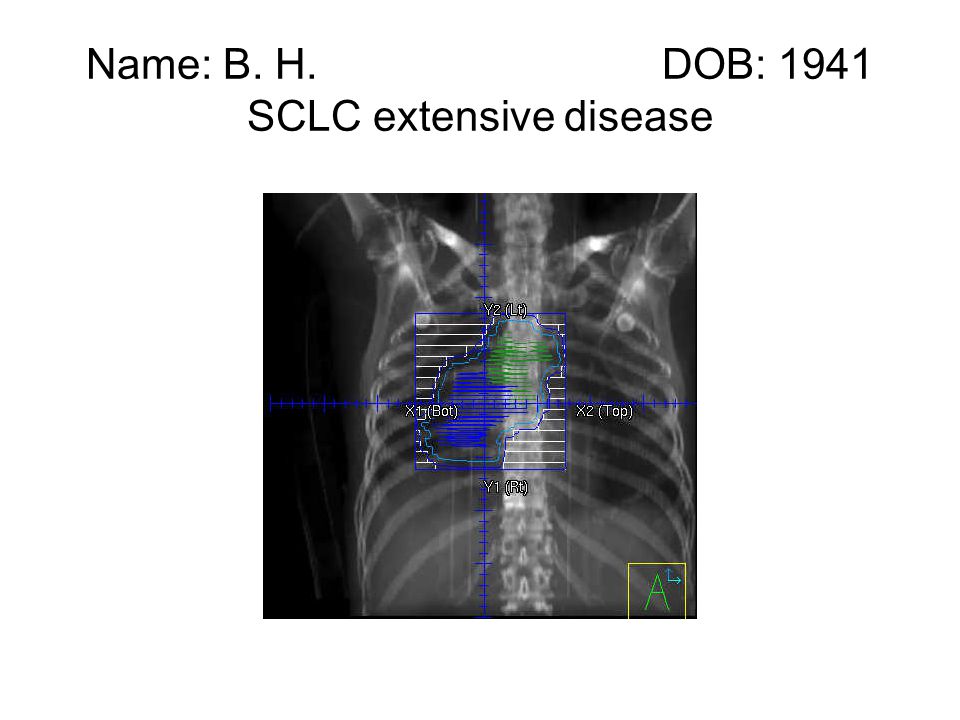
Name: B. H. DOB: 1941 SCLC extensive disease Diagnosis / Histology: SCLC of the right lower lobe (diagnosis in 2006) - extensive disease (multiple bilateral mediastinal lymph nodes, 1 2 cm met. in left liver lobe) - 6 cycles Carboplatin / Etopophos 6-9/06, PR after 3 cycles, progression after 6 cycles - 10/06: progression of mediastinal lymph nodes and intrapulmonary tumour Status: Current problems:locoregional tumor progression Radiotherapy Concept: RT of the mediastinum and the primary lung tumor with 22 x 1.8 Gy = 39.6 Gy followed by 10 x 1.8Gy = 18 Gy without spinal cord. Total dose 59.6 Gy. PTV-Standard: CTV: tumour + 0.6 – 0.8cm margin in all directions and regional lymph nodes PTV: transversal: GTV + 1cm, axial: GTV + 1.5 – 2cm
 - extensive disease (multiple bilateral mediastinal lymph nodes, 1 2 cm met. in left liver lobe) - 6 cycles Carboplatin / Etopophos 6-9/06, PR after 3 cycles, progression after 6 cycles - 10/06: progression of mediastinal lymph nodes and intrapulmonary tumour Status: Current problems:locoregional tumor progression Radiotherapy Concept: RT of the mediastinum and the primary lung tumor with 22 x 1.8 Gy = 39.6 Gy followed by 10 x 1.8Gy = 18 Gy without spinal cord. Total dose 59.6 Gy. PTV-Standard: CTV: tumour – 0.8cm margin in all directions and regional lymph nodes PTV: transversal: GTV + 1cm, axial: GTV – 2cm.")
18
Name: B. H. DOB: 1941 SCLC extensive disease Deviation from standards / Reason: none Literature: - Jeremic et all, Initial versus delayed accelerated hyperfractionated radiation therapy and concurrent chemotherapy in limited small-cell lung cancer: a randomized study. JCO 1997: 893- 900. - Murray et all, Importance of timing for thoracic irradiation in the combined modality treatment of limited-stage small-cell lung cancer. The National Cancer Institute of Canada Clinical Trials Group. JCO 1993: 336-344 - Pignon et all, A metaanalysis of thoracic radiotherapy for small-cell lung cancer. NEJM 1992;327:1618-24 - Pignon et all, Role of thoracic radiotherapy in limited-stage small-cell lung cancer: quantitative review based on the literature versus meta-analysis based on individual data. JCO 1992;10:1819- 20 - Takada et all, Phase III Study of Concurrent Versus Sequential Thoracic Radiotherapy in Combination With Cisplatin and Etoposide for Limited-Stage Small-Cell Lung Cancer: Results of the Japan Clinical Oncology Group Study 9104. JCO 2002: 3054-3060 Status at last f/u 3 months after tt: Primary tumor and regional lymphnodes: partial remission (60% on CT), no clinical symptoms Liver metastasis: tumorgrowth 20% on CT (left lobe), 2nd small suspicious lesion (caudate lobe)
, no clinical symptoms Liver metastasis: tumorgrowth 20% on CT (left lobe), 2nd small suspicious lesion (caudate lobe).")
19
Name: B. H. DOB: 1941 SCLC extensive disease

Similar presentations










 and N+, chemotherapy should be added.>")




 Mortality:8-9/100000/year Fourth most common cancer in men.>")

: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")






