Download presentation
Presentation is loading. Please wait.

1
QI, in a nutshell Quality and Safety Educator’s Academy, Society of Hospital Medicine and Georgia McIntosh, MD

2
6 Steps to QI 1. Understand the problem 2. Identify areas for change/improvement 3. Explicitly state your goals 4. How will you measure progress 5. Create effective, reliable improvements 6. Build upon success and sustain the process

3
6 Steps to QI 1. Understand the problem 2. Identify areas for change/improvement 3. Explicitly state your goals 4. How will you measure progress 5. Create effective, reliable improvements 6. Build upon success and sustain the process

4
Process Modeling Tools
Cause and Effect Diagram or Fishbone diagram Standard Flow diagram Deployment Flowchart or Swim-lane Diagram Mind Map

5
Process Modeling Tools
Cause and effect diagram ( “fishbone or ishikawa”) Process Map
 Process Map.")
6
Process Modeling Tools Mind Map

7
Process Modeling Tools Deployment Flowchart or Swim-lane Diagram
Deployment flowchart- AKA swim-lane diagram. Standard flowchart but looks at each individual who interacts with the patient at certain stages. Includes columns ofr measures of each stage of the process and opportunities for improvement at each stage of the process.

8
Error Reduction Strategies
Strong actions Intermediate Actions Weak Actions

9
6 Steps to QI 1. Understand the problem 2. Identify areas for change/improvement 3. Explicitly state your goals 4. How will you measure progress 5. Create effective, reliable improvements 6. Build upon success and sustain the process

10
Donabedian’s Topology of Quality Measures
Structure How was care delivered to the patient Process What was done to the patient Outcome What happened to the patient Balancing Unintended, undesirable consequences

11
Structure, Process or Outcome?
30 day mortality after CABG Bone densitometry ordered in women over 65 Computerized order entry ACE or ARB for CHF pts with low EF Last BP of < 140/90 in pts with HTN Physician boarded in critical care medicine responding to codes at all times

12
6 Steps to QI 1. Understand the problem 2. Identify areas for change/improvement 3. Explicitly state your goals 4. How will you measure progress 5. Create effective, reliable improvements 6. Build upon success and sustain the process

13
“VCUHS will be the safest hospital in the United States.”
Aim Statement “VCUHS will be the safest hospital in the United States.”

14
Aim Statement VCUHS’ mission is “to become America’s safest health system with the goal of zero events of preventable harm to patients, team members and visitors.”

15
Aim Statement VCUHS’ mission is “to become America’s safest health system with the goal of zero events of preventable harm to patients, team members and visitors.” For whom? How good? By when?

16
6 Steps to QI 1. Understand the problem 2. Identify areas for change/improvement 3. Explicitly state your goals 4. How will you measure progress 5. Create effective, reliable improvements 6. Build upon success and sustain the process

17
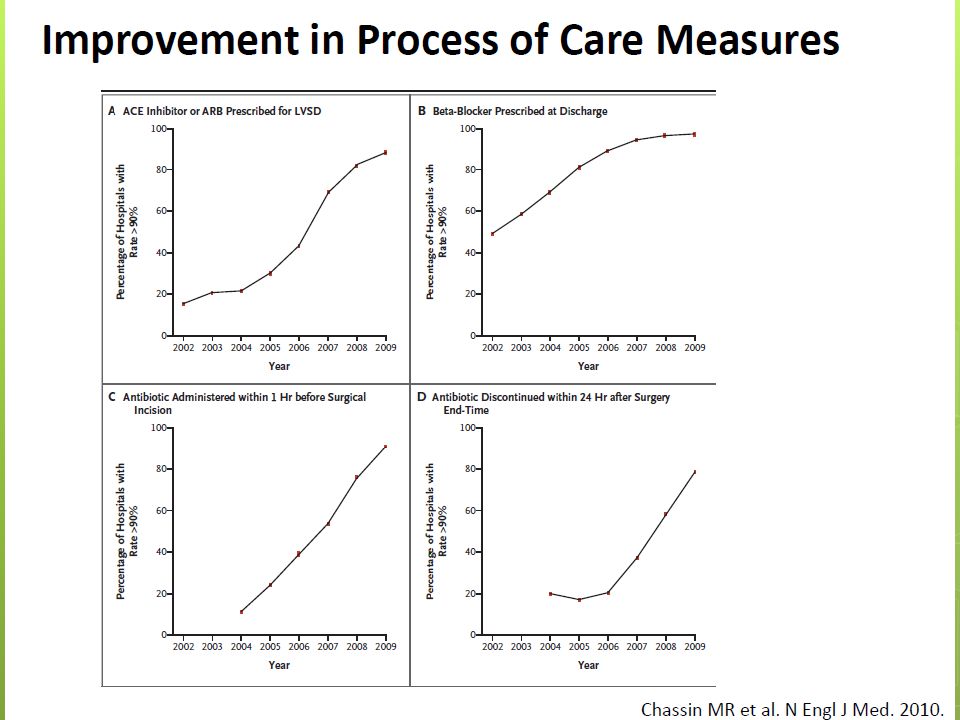
Measurement Payers Demanding Increased Accountability
Voluntary reporting to payer Pay for reporting to payer Public reporting Pay for performance

24
6 Steps to QI 1. Understand the problem 2. Identify areas for change/improvement 3. Explicitly state your goals 4. How will you measure progress 5. Create effective, reliable improvements 6. Build upon success and sustain the process

31
6 Steps to QI 1. Understand the problem 2. Identify areas for change/improvement 3. Explicitly state your goals 4. How will you measure progress 5. Create effective, reliable improvements 6. Build upon success and sustain the process

32
Recently, several complaints have been filed by patients in your clinic about excessive wait times in the lobby. As a member of the quality team at your clinic, you are charged to study and fix this problem. Which of the following improvement methodologies would be most successful at reducing wait times for patients in the clinic lobby? LEAN Six Sigma Cause-and-effect diagramming Swim lane diagramming Failure mode and effects analysis

33
Recently, several complaints have been filed by patients in your clinic about excessive wait times in the lobby. As a member of the quality team at your clinic, you are charged to study and fix this problem. Which of the following improvement methodologies would be most successful at reducing wait times for patients in the clinic lobby? LEAN Six Sigma Cause-and-effect diagramming Swim lane diagramming Failure mode and effects analysis

34
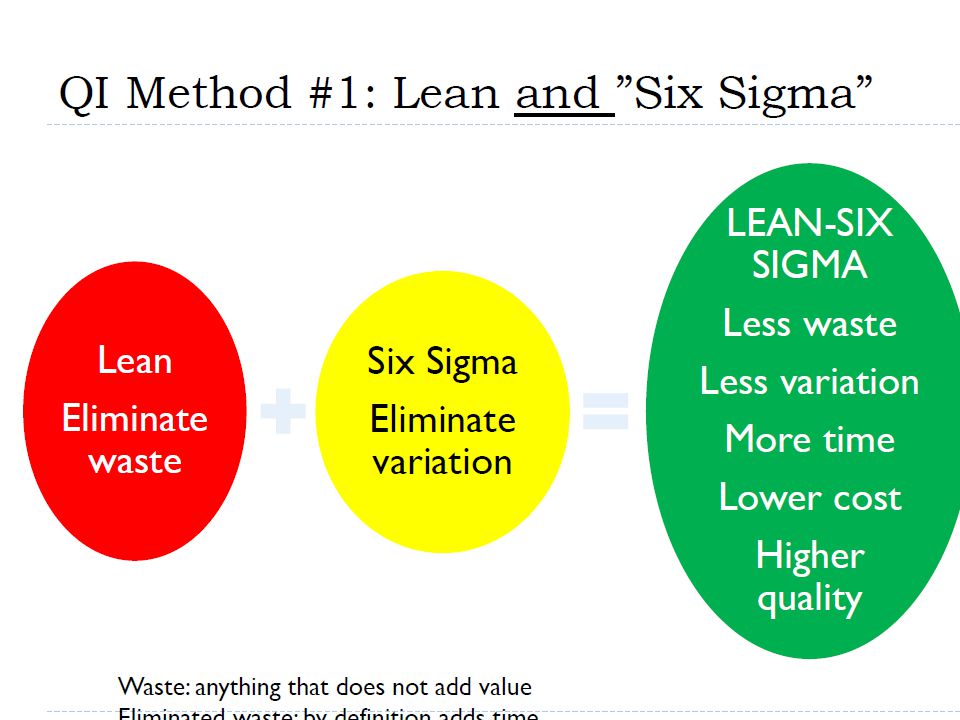
LEAN Developed by Toyota Aim to eliminate waste in the system
Most common waste is patient wait time

35
Six Sigma Invented by Motorola
Designed to remove defects and variations from a system Six sigma means 6 standard deveiations from the mean which represents 3.4 defects per 1 million opportunities Utilizes DMAIC methodology Design, Measure, Analyze, Improve, Control

36
Cause and effect diagramming
AKA Fishbone diagram Uncovers the factors that influence an outcome Hypothesis-generating tool

37
Deployment Flowchart or Swim-lane Diagram
Deployment flowchart- AKA swim-lane diagram. Standard flowchart but looks at each individual who interacts with the patient at certain stages. Includes columns ofr measures of each stage of the process and opportunities for improvement at each stage of the process.

38
Failure mode and effects analysis
Tool for classifying errors by severity and likelihood of recurrence for use in prioritizing quality initiatives

39
Failure Mode and Effects Analysis
systematic, proactive method for evaluating a process to identify where and how it might fail, and to assess the relative impact of different failures in order to identify the parts of the process that are most in need of change.

40
2. You serve on the sentinel event review committee
2. You serve on the sentinel event review committee. An event occurred in which a patient received an overdose of heparin. Your committee completes a root cause analysis and finds that the error resulted from a gap in physician knowledge about heparin dosing, the lack of an institutional consensus on heparin dosing, and a cumbersome order entry system. From the root cause analysis, which of the following interventions is most likely to have a sustained effect? Online education module on heparin dosing Distribution of a heparin dosing pocket card A heparin order set A new institutional policy on heparin dosing A physician education conference on heparin dosing

41
2. You serve on the sentinel event review committee
2. You serve on the sentinel event review committee. An event occurred in which a patient received an overdose of heparin. Your committee completes a root cause analysis and finds that the error resulted from a gap in physician knowledge about heparin dosing, the lack of an institutional consensus on heparin dosing, and a cumbersome order entry system. From the root cause analysis, which of the following interventions is most likely to have a sustained effect? Online education module on heparin dosing Distribution of a heparin dosing pocket card A heparin order set A new institutional policy on heparin dosing A physician education conference on heparin dosing

42
Error Reduction Strategies
Strong actions Intermediate Actions Weak Actions

43
How do you prevent customers from leaving behind their ATM cards?
Strong Action- Swipe card only Intermediate Action- Beeping Weak Action- signs

Similar presentations















 Robert Martin, PsyD Performance Excellence UCLA.>")



 Minds.>")



>")




