Download presentation
Presentation is loading. Please wait.

1
The Referral Is the Key 18 weeks Referral to Treatment standard Tracey Gillies National Clinical Lead for 18 weeks Service Redesign and Transformation Improvement and Support Team, SGHD

2
“ a whole journey waiting time target of 18 weeks from general practitioner referral to treatment …. by December 2011” Cabinet Secretary for Health and Wellbeing, Scottish Parliament – Official Report, 28th June 2007. “… how should the new waiting time target be defined in order to maximise its potential for improving the quality of patient care?” Better Health, Better Care, August 2007 18 Weeks Referral to Treatment Time

4
Current view of many clinicians Quality Speed of access

5
Dimensions of Quality

6
What do patients want? How can we improve patients’ experience Develop One Stop Clinics Reduce sequential testing (where possible) Develop robust pre-operative assessment processes Develop strong discharge planning processes
 Develop robust pre-operative assessment processes Develop strong discharge planning processes.")
7
Patient Flows Outpatient Assessment Diagnosis and Treatment Day Case Inpatient Whole patient journey 11.3 million contacts per annum 0.4 million contacts per annum 0.2 million planned contacts per annum

8
High Impact Changes Outpatient Day Case Inpatient Referral Management Services Eliminating unnecessary follow up Extend patient focused booking Treating day surgery as the norm Pre-operative assessment and booking Same day admission Identifying time based flows Optimising LOS profile Pre-operative assessment and booking Discharge planning on admission.

9
Patient Flows Outpatient Assessment Diagnosis and Treatment = 11.3 million contacts per annum Day Case = 0.4 million contacts per annum In patient 0.2 million planned contacts per annum

10
Percent of completed admitted and non-admitted pathways with a known clock start- May 08 DOH, England 08

11
Patient Pathway Improve referral and diagnostic pathways Treat day surgery as the norm Actively manage admissions to hospital Actively manage discharge and length of stay Actively manage follow ups Focus on 5 Simple Changes

12
Improve access, diagnostic and assessment process Actively manage admission to hospital Treat day surgery as the norm Actively manage discharge and length of stay Actively manage follow up Improve patient flow - develop and manage patient pathways Reduce variation develop protocol- driven care Utilise and develop the skills of the workforce Optimise administrative processes Improve materials management Understand and manage demand and capacity (remove carve out,reduce the number of queues)
")
13
Building on previous experience and best practice

14
GPIPOPD 18 weeks GP Visit1 st Appointmen t Decision to treat Treatment The time from the first outpatient consultation to decision to treat (or not to treat) includes the most significant challenges including all diagnostics and subsequent outpatient appointments. Grey Bit!

15
Current time? OP Test OP Rx End of pathway Patient sees GP 18 weeks9 weeks18 weeks Size of gap unknown

17
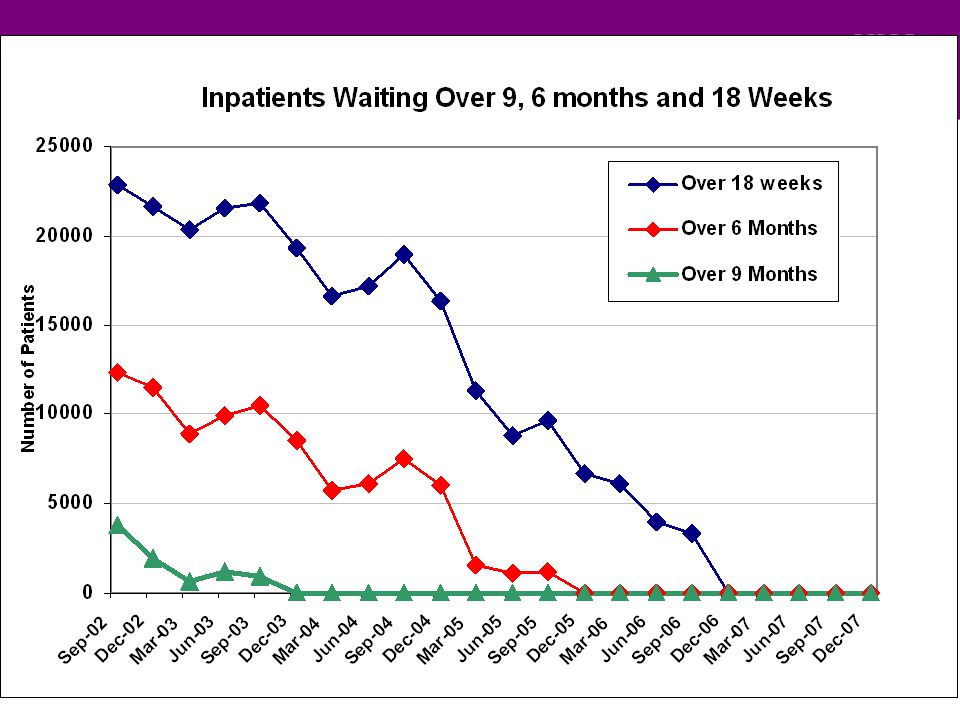
Redesign Backlog Two streams of work going on in parallel Towards an 18 week total journey by 2011 Temporary increase in throughput between 2008 and 2011

18
Typical non admitted pathway Referral Outpatient visit Diagnostic test Outpatient visit Appointment

19
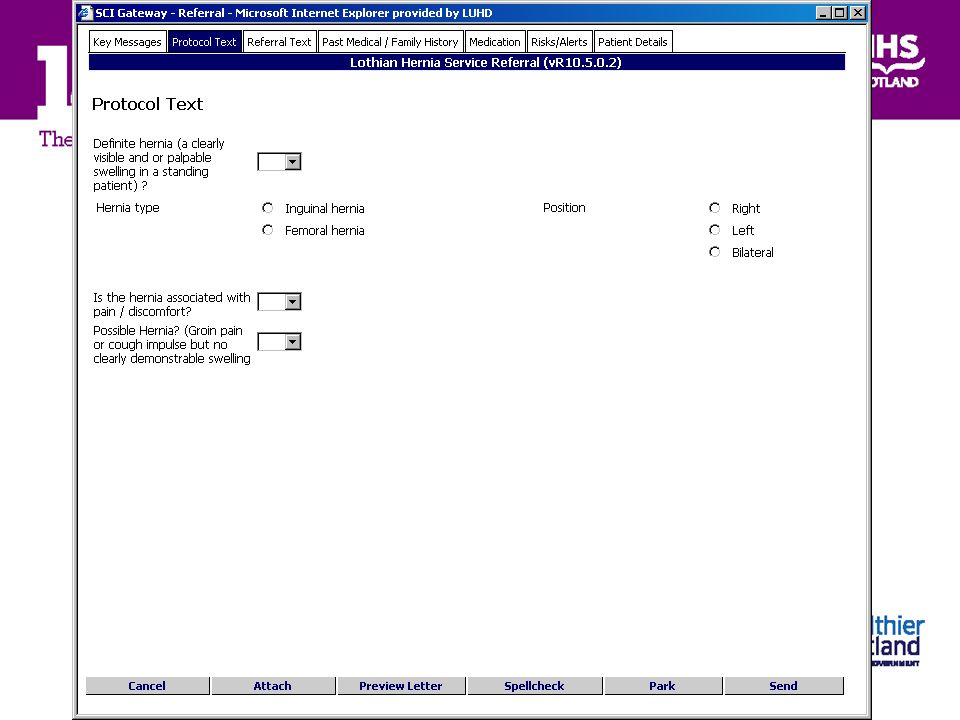
GPHospRegistrationSortTriage Make Appoint 0 – 11 days 1 - 9 days 2 – 8 days 1 – 36 days 1 – 14 days 4 – 58 days 70% SCI Gateway 99% manual

20
What exactly do we mean by e triage? Deal with referral electronically Attribute clinical priority/destination/PFB queue Make this information available to referrer Role of e triage in referral management Reduction in waste Right referral to right place/person Benefits for referrer- transparency of process Improve demand and capacity work

21
Recording of decision as part of management of the pathway Straight to test / one stop 126 days Reduce time to appoint Patient choice Communicate decision and information Non admitted pathway in the future

22
Is the purpose of the referral clear? Are there useful referral protocols in place? What information does the patient have or need? Is the timescale appropriate?

24
Natural History of referrals

25
Online Knowledge service Joint development between NES and 18 weeks Owned at board level Local pathways, linked to available evidence Patient area

28
Evidence based condition specific pathways Health board local modifications 18 week website IST toolkit SIGN Primary care Patient

29
Using headache as an example SIGN Specialty literature Neurology ENT Radiology Oral Surgery Primary care Patient evidence based pathways Local pathways Health board level Community pharmacy Self help groups Patient association NHS 24 LTC

30
Advantages Management of patient expectation Pace of change between now and 2011 rapid and difficult to maintain communication Dissemination of information Up to each board to use as much as wished Addresses in part the mutuality and shifting the balance of care agenda Needs to be “living “ not once only

Similar presentations




 Dr Martin Connor Associate Director (Health Reform) Greater Manchester Strategic Health.>")













 Development Team.>")



 NHS Connecting for Health Health Informatics and the Chronic Conditions.>")
