Download presentation
Presentation is loading. Please wait.

1
PRIMARY & SECONDARY ANTIBODY DEFICIENCY

2
ANTIBODIES & IMMUNOGLOBULINS

3
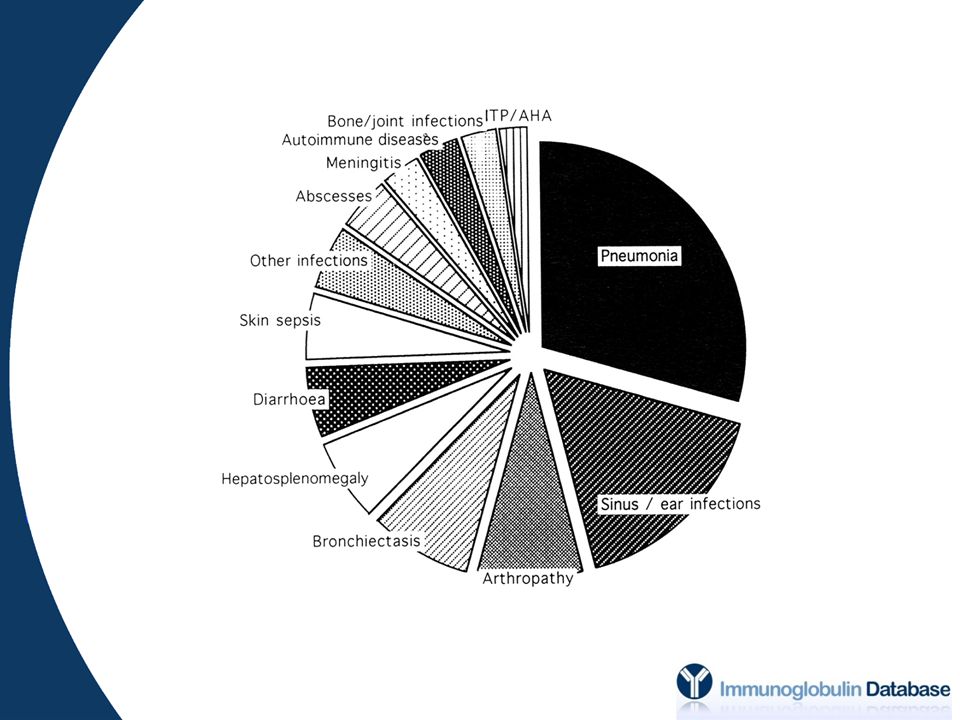
PRIMARY ANTIBODY DEFICIENCY
The European internet-based patient and research database for primary immunodeficiencies: results Gathman et al., Clin Exp Immunol (2009); 157 Suppl 1: 3-11.
; 157 Suppl 1:")
5
Brit Med J (1989); 298: 516-7
; 298: 516-7")
6
THERAPEUTIC IMMUNOGLOBULIN
1970s - IMIg 1980s - IVIg 1990s - IVIg, SCIg 2000s - product safety - infusion rates / concentration - immunoglobulin retrieval

7
REPLACEMENT THERAPY

8
TREATMENT OUTCOMES Wood et al. Clin Exp Immunol (2007); 149:
; 149:")
9
EFFICACY & ADVERSITY Immunoglobulin Excipients Soluble CD4/ CD8/ HLA
Cytokines Clin Exp Immunol (2004); 136: 111-3
; 136:")
10
IVIg & SCIg ESID Register 2009

11
HOME THERAPY

12
2008 and 2011

13
SAME OLD SAME OLD Core of PID management No alternatives
Lifelong requirement (usually) Effective (bacterial infection, antibiotic usage, QoL, hospitalisation, life expectancy) Dose requirement in: - frequent breakthrough infections - chronic inflammation / tissue damage - poor prognosis disease variants
 Effective. (bacterial infection, antibiotic usage, QoL, hospitalisation, life expectancy) Dose requirement in: - frequent breakthrough infections. - chronic inflammation / tissue damage. - poor prognosis disease variants.")
14
WHAT’S NEW? The three Rs: Reorganisation Reclassification Aarrrgh
- ongoing uncertainties over dosing / target levels

15
DOSE? Impact of trough IgG on pneumonia incidence in primary immunodeficiency: A meta-analysis of clinical studies. Orange JS et al. Clinical Immunology (2010); 137: 21-30
; 137:")
16
DOSE: INDIVIDUALISATION
‘The goal of replacement therapy should be to improve clinical outcome and not to reach a particular IgG trough level.’ J Allergy Clin Immunol (2010);125:
;125:")
17
DOSE: INDIVIDUALISATION
‘….individualizing the dosage….is preferable to using mean pharmacokinetic parameters.’ Clin Immunol (2011);139:133-41
;139:")
18
RECLASSIFICATION Specific Antibody Deficiency Kawasaki Disease
‘Other’ Section

19
REORGANISATION

20
PRIMARY ANTIBODY DEFICIENCY DISORDERS

21
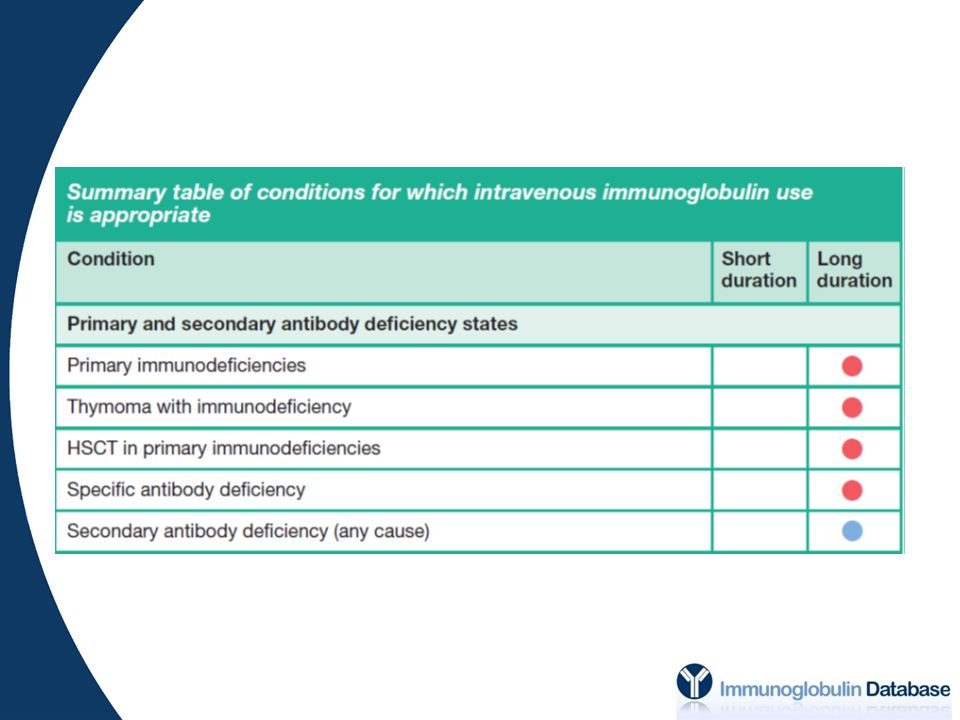
SPECIFIC DISORDERS Thymoma with immunodeficiency (Good’s Syndrome)
Combined immunodeficiencies requiring haemopoietic stem cell transplantation (HSCT) Specific antibody deficiency (SAD) Transient hypogammaglobulinaemia of infancy (THI)
 Specific antibody deficiency. (SAD) Transient hypogammaglobulinaemia of infancy. (THI)")
22
RECOMMENDATION / REQUIREMENT
SPECIFIC DISORDERS DISORDER RECOMMENDATION / REQUIREMENT GOOD’S Profound B cell depletion / significant antibody deficiency HSCT Duration based on B cell reconstitution post-transplantation SAD Robust application of selection criteria THI Define planned duration of therapy prior to initiation (GRADE C, LEVEL III)
")
23
SUMMARY: PID

24
SECONDARY ANTIBODY DEFICIENCY
PRIMARY SECONDARY Malignant disease Drugs Protein-losing states Infection (cause & effect) Systemic disease Iatrogenic causes Chromosomal abnormalities
 Systemic disease. Iatrogenic causes. Chromosomal abnormalities.")
25
WHAT’S NEW? Secondary Antibody Deficiency
Revision / collation into a single indication + review outcomes (infection / hospitalisation) + dosing (minimum IgG trough 6 g/L)
 + dosing (minimum IgG trough 6 g/L)")
26
RECOMMENDATIONS Irreversible hypo-
Hypo- associated with CLL/NHL/MM etc. and

27
GUIDELINES Evidence-based use Consistency of care
‘Systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances’ Evidence-based use Consistency of care Access to safe, high quality products Security of supply Utilising scarce resource

29
OUTCOMES COMPLICATIONS PROGRESSION OF COMPLICATIONS QUALITY OF LIFE
WORKING CAPACITY LIFE EXPECTANCY OPTIMISED GROWTH / DEVELOPMENT

Similar presentations











 + standard of care (SOC)>")

 -Risk factors for poor HRQL ESID-INGID-IPOPI Meeting 2012 Ann Gardulf.>")


 in Patients with Secondary Myelodysplastic Syndromes (sMDS) Enrolled in the AVIDA Registry 1 Prospective Trial.>")



