Download presentation
Presentation is loading. Please wait.

1
Preventing accidental exposures from new external beam radiation therapy technologies ICRP Publication 112 Task Group: P. Ortiz López (chairman), J.M. Cosset, O. Holmberg, J.C. Rosenwald, P. Dunscombe, J.J. Vilaragut, L. Pinillos, S. Vatnitsky
, J.M. Cosset, O. Holmberg, J.C. Rosenwald, P. Dunscombe, J.J. Vilaragut, L. Pinillos, S. Vatnitsky.")
2
Lessons from accidental exposures with conventional techniques are available
They have been useful in improving safety

3
The key questions are: Are lessons from conventional techniques applicable to newer technologies? Are there new lessons from new technologies? Can we anticipate “what else can go wrong?” We will address the following questions Can we apply the lessons from conventional techniques to new technologies, Do we have already new lessons i from new technologies Appart from these lessons, ¿is there anything else we have to take care of? INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

4
Applicable to new technologies?
1st question Are lessons from conventional techniques applicable to newer technologies? Applicable to new technologies? Let us start with the first of the three questions. There are lessons from conventional techniques. Are these lessons still valid

5
Overall lesson from conventional techniques
“…purchasing new equipment without a concomitant effort on education and training and on a programme of quality assurance is dangerous”. Valid for new technologies? The most general lesson is that purchashing new equipment without due attention to training is dangerous. Is it stil valid??? Of course, it is Yes, indeed

6
Lessons from conventional techniques valid for new technologies?
Beam calibration: independent verification of absorbed dose at the reference point From the accidental exposure in Costa Rica we have learnd this lesson that independent verification of absorbed dose is necessary.Is this also applicable to new technologies. Of course, yes 115 patients severely affected INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

7
Lessons from conventional techniques valid for new technologies?
Need for commissioning of treatment planning systems (TPS) Validation of procedures and of their modifications, particularly TPS For individual patients: check of the dose to a point, independently fromTPS calculations 28 patients severely overdosed in Panama 1045 patients underdosed in the UK The lesson from the wrong use of a treatment planing system and the UK and Panamá accidental exposures was that, not being TPS a radiation source, it requires proper commissioning and validation of procedures, like an accelerator does. In addition, for each individual treatment there is a need for checking the dose to a point, in a way that is independent from the TPS calculations
 Validation of procedures and of their modifications, particularly TPS. For individual patients: check of the dose to a point, independently fromTPS calculations. 28 patients severely overdosed in Panama patients underdosed in the UK. The lesson from the wrong use of a treatment planing system and the UK and Panamá accidental exposures was that, not being TPS a radiation source, it requires proper commissioning and validation of procedures, like an accelerator does. In addition, for each individual treatment there is a need for checking the dose to a point, in a way that is independent from the TPS calculations.")
8
Lessons from conventional techniques valid for new technologies?
Clear notification of maintenance and repairs to the person responsible for radiotherapy physics, before resuming patient treatments 27 patients severely affected in Spain The lesson from the accidental exposure in Spain is the need for clearly notifinying any maintenance or repair to the medical physicist before resuming treatments. And yes, this is also applicable to new technologies, as well

9
All these lessons from conventional techniques are valid for new technologies They should be part of training programmes, and incorporated into procedures in radiotherapy departments In summary, most lessons from conventional techniques are applicable and should be used for training and developing procedures

10
2nd question Are there new lessons from new technologies?
Yes, the following Let us go now to the second question Do we have new lessons from new technologies INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

11
New lessons: Software control of accelerator functions data integrity may be lost after computer “crash” or “frozen”

12
Loss of data integrity When saving data on treatment plan, the computer got “frozen”. After restarting, data on collimator setting was “lost” from the data file As a result, open fields instead of small fields were applied Consequences: one patient received 39 Gy in the first three sessions Checking procedures are required for computer “crashes”. Irradiation parameters may be wrong upon INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

13
Interlock misadjustment Interlock understanding
Test of interlocks at equipment acceptance

14
Tolerances and interlocks
Misadjustment of the tolerance limits of a dose-rate interlock occurred on a tomotherapy unit Important: understanding interlocks and ensuring their testing at equipment acceptance INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

15
Wrong calibration files for an applicator were supplied by the manufacturer

16
Intraoperative radiotherapy
Supply of wrong calibration file for a given applicator Measurements revealed a discrepancy, the physicist asked the installation engineer and received an erroneous advice The radiotherapy department accepted the advice, assuming that the maintenance engineer was right and the measurements by the physicist may be wrong The problem was discovered later at a survey Avoid “believes or assumptions” and base the treatment on proper understanding and verification! INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

17
Errors from imaging: Wrong site treatment (right-left) Image distortion
 Image distortion")
18
Multiple imaging modalities: problem with consistency in identification and labelling
Left-right error Distorsion of images when transferring them from the TPS to the “record and verify” Potential problems of image artefacts and wrong tissue density Wiith increased use of different imaging modalities, consistency in imaging identification and image labelling becomes more critical INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

19
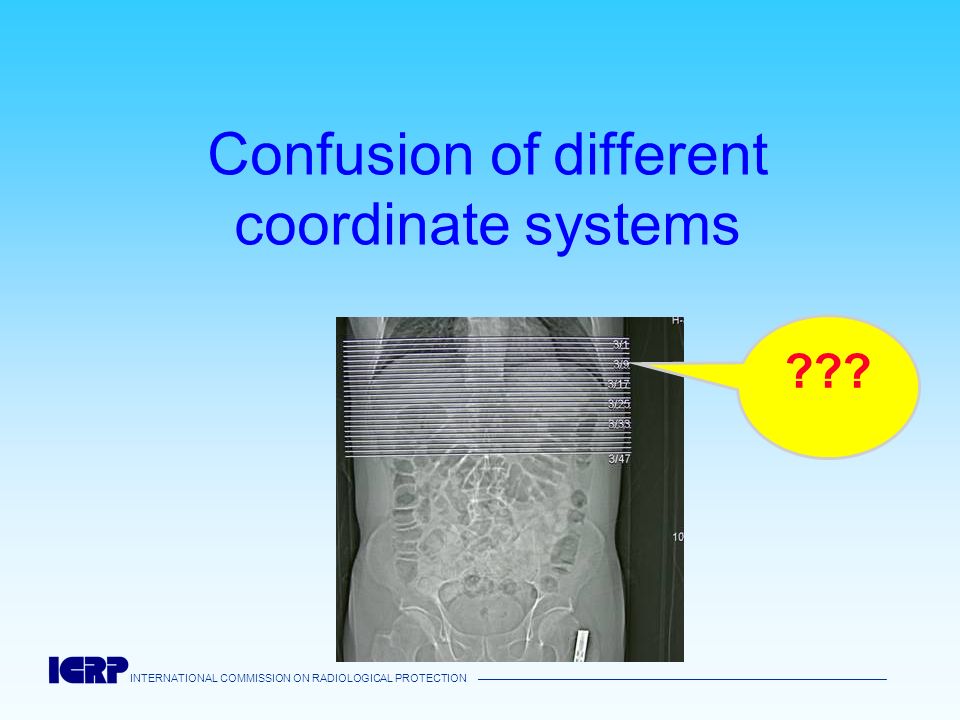
Image reconstruction Geometric distorsion of CT images, when being uploaded in the graphics memory of the TPS Misplacement of the field coordinates Attention to image data transfer: Specific verifications required INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

20
Confusion of different coordinate systems
???
21
Reference markers in virtual simulation
The tatoo for the initial plane of virtual simulation (A) was taken as the isocenter plane (B). Understanding and becoming fully familiar with details of new techniques (A) (B) INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————
 was taken as the isocenter plane (B). Understanding and becoming fully familiar with details of new techniques. (A) (B) INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————")
22
Significant radiation dose from daily imaging for verification

23
Daily imaging for localization
Significant radiation dose was given from daily localization images Need to integrate significant imaging doses into the therapy dose planned by the TPS INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

24
Several events due to poor understanding of new techniques and poor communication and recording
And finally, there is risk in poor understanding of complex techniques or in poor recording and communication

25
Calibration of very small beams (micro multileaf collimators)
Partial volume irradiation of the chamber. Wrong absorbed dose determination Knowledge needs to be sharper, as well as the level of awareness of the task at hand Education and specific training essential for new technologies INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

26
Record and verify systems
Old system: TPS calculation for normalized dose (1Gy) followed by manual scaling up to the prescribed dose when transferring the plan to the record and verify system New system: direct scaling up by the TPS and automatic transfer Unusual treatment modality. Scaling up was done twice. A check procedure was not followed. About 67% overdose INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————
 followed by manual scaling up to the prescribed dose when transferring the plan to the record and verify system. New system: direct scaling up by the TPS and automatic transfer. Unusual treatment modality. Scaling up was done twice. A check procedure was not followed. About 67% overdose. INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————")
27
Dynamic wedges Erroneous selection of the type of wedges with the result of excessive monitor units Monitor units for physical wedges, treatment with dynamic wedge Misunderstanding of the acronym (enhanced wedges, EW) 23 patients overdosed, four of them died in the first year INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————
 23 patients overdosed, four of them died in the first year. INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————")
28
Small fields in stereotactic treatment with applicator
INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

29
Confusion 40 mm - 40 cm Patient died from the accidental exposure
INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

30
Avoid poor understanding of new techniques and poor communication and recording Lesson No “quick” training… A common conclusion of all these problems of poor understanding is that proper training can not be replaced by a quick or short briefing, from which many risks may not be appreciated. … but solid training

31
All these new lessons are useful in preventing reported types of risks, but
INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

32
3rd question: Can we anticipate what else can go wrong?
INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

33
The unknown or unreported
What about possible unreported events? What about other types of potential events, which have not happened yet? Do we need to wait until they occur, to learn the lesson? ¿What should be done about increasing equipment complexity and thus ever larger lists of double checks and verifications? INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————

34
There are proactive methods of safety assessment
Failure mode and effect analysis (FMEA) Probabilistic Safety Assessment (PSA) Risk Matrix Approach Examples: work done by the Ibero American FORO of Nuclear and Radiation Safety Regulatory Agencies and by the American Association of Physicists in Medicine, briefly described in ICRP 112 INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————
 Probabilistic Safety Assessment (PSA) Risk Matrix Approach. Examples: work done by the Ibero American FORO of Nuclear and Radiation Safety Regulatory Agencies and by the American Association of Physicists in Medicine, briefly described in ICRP 112. INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————")
35
Example No. 1 of major finding from probabilistic safety assessment
Much attention has been focused on major catastrophic, multiple-patient events with very low probability, but Other types of events with much higher probability, involving single patients, can also be severe, may more easily go unreported They deserve increased attention and preventive measures

36
Example No. 2 of major finding from probabilistic safety assessment
Increased software control (control of linear accelerator functions, treatment planning, virtual simulation, image guided radiotherapy, record and verify control, radiotherapy information systems, electronic charts) confers software safety a paramount importance Software deserves increased attention in standards and by regulatory bodies and professional bodies;
 confers software safety a paramount importance. Software deserves increased attention in standards and by regulatory bodies and professional bodies;")
37
Example No. 3 of major finding from probabilistic safety assessment
Safety aspects related to the approval of the treatment plan by the radiation oncology and measures on the patient directly such as in vivo dosimetry or its equivalent measures, daily observation of the patient and periodic medical control bear an important part in risk reduction, in terms of prevention and mitigation of accidental exposures

38
Take-home messages

39
Introducing new technologies
Decision to implement a new technology should be based on an evaluation of the expected benefit, rather than being driven by technology itself A step-by-step approach should be followed to ensure a safe implementation.

40
Staff training, availability and dedication
Replacement of proper training with a short briefing or demonstration should be avoided, because important safety implications of new techniques cannot be fully appreciated from a short briefing. Certain safety-critical tasks, such as calibration, beam characterization, complex treatment planning and pretreatment verification, require a substantial increase in staff allocation.

41
Safety awareness of responsible persons for radiotherapy
Independent verification of beam calibration remains essential. Investigating discrepancies in dose measurements before applying the beam to patient treatments. Hospital administrators of radiation therapy departments should provide a work environment that encourages working with awareness, facilitates concentration and avoids distraction.

42
Manufacturers Manufacturers should be aware of their responsibility for delivering the correct equipment with the correct calibration files and accompanying documents. They also have a responsibility to provide correct information and advice, upon request, from users. Procedures to meet these responsibilities should be developed and quality controlled.

43
Programme of purchasing, acceptance and commissioning
Programmes for purchasing, acceptance testing and commissioning should not only address treatment machines but also treatment planning systems, radiation therapy information systems, imaging equipment used for radiation therapy, software, procedures and entire clinical processes. Devices and processes should be re-commissioned after equipment modifications including software upgrades and updates.

44
Need for new protocols for treatment prescription and dosimetry
Protocols for treatment prescription, reporting and recording, such as found in ICRU reports, should be revised to accommodate new technologies. They should be adopted at a national level with the support of professional bodies. Similarly, dosimetry protocols should be developed for small and non-standard radiation fields.

45
Dose escalation Dose escalation without a concomitant increase in normal tissue complication probability generally implies a reduction of geometrical margins. Such a reduction is only possible with conformal therapy accompanied by precise, image-guided patient positioning and effective immobilization together with a clear understanding of the accuracy achieved in clinical practice. Without these features, target dose escalation could lead to severe patient complications

46
Safety-critical communication and notifications
Unambiguous, well structured communication is essential, considering the complexity of radiation therapy and the multidisciplinary nature of the health care environment. In particular, procedures to notify physicists of maintenance and repair activities, identified as crucial in conventional technology, are even more necessary with new technologies.

47
Computers and data integrity
Procedures should be in place to deal with situations created by computer “crashes”, which may cause loss of data integrity and lead to severe accidental exposures.

48
Updating of quality control tests
When conventional tests and checks are not applicable or not effective for new technologies, the safety philosophy should aim at finding measures to maintain the required level of safety. This may require the design of new tests or the modification and validation of the old ones.

49
Using lessons from experience
Lessons learned from past accidental exposure should be incorporated into training. Radiation therapy facilities are encouraged to share their experiences of actual and potential safety incidents through participation in databases such as Radiation Oncology Safety Information System (ROSIS), often referred to in this report.
, often referred to in this report.")
50
Overcoming the lack of experience when introducing new technologies
Prior to the introduction of new techniques and technologies, there is little or no operational experience to share. Two complementary measures are recommended: Prospective safety assessments should be undertaken in order to develop risk-informed and cost-effective quality assurance programmes. Moderated electronic networks and panels of experts supported by professional bodies should be established in order to expedite knowledge sharing at the early phase of introducing a new technology.

51
Recap Most lessons from conventional techniques are applicable to new technologies Additional lessons for new technologies have become available (ICRP 112) Anticipative approaches provide a risk-informed and rational choice of safety provisions INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————
 Anticipative approaches provide a risk-informed and rational choice of safety provisions. INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION ——————————————————————————————————————")
52
Thank you You are invited to use these lessons for training and to apply them in practice More details in ICRP publication 112

Similar presentations



 and Safety Management System (SMS) in the Context of the Seveso II Directive.>")
![[Organisation’s Title] Environmental Management System](/9/2492851/big_thumb.jpg "[Organisation’s Title] Environmental Management System>")




 IAEA Training Course.>")









