Download presentation
Presentation is loading. Please wait.

1
Optimizing Management of Pulmonary Embolism: From Threat to Therapy Samuel Z. Goldhaber, MD Cardiovascular Division Brigham and Women’s Hospital Professor of Medicine Harvard Medical School Samuel Z. Goldhaber, MD Cardiovascular Division Brigham and Women’s Hospital Professor of Medicine Harvard Medical School DVT-WRAP SlideCAST

2
Learning Objectives ► Epidemiology ► Diagnosis ► Risk Stratification ► Treatment: anticoagulation thrombolysisembolectomy ► Prevention ► Epidemiology ► Diagnosis ► Risk Stratification ► Treatment: anticoagulation thrombolysisembolectomy ► Prevention

3
Epidemiology

5
Incidence 900,000 PEs/ DVTs in USA in 2002. Estimated 296,000 PE deaths: 7% treated, 34% sudden and fatal, and 59% undetected. Heit J. ASH Abstract 2005 ----------------------------------------- 762,000 PEs/ DVTs in EU in 2004. Thromb Haemostas 2007; 98: 756 4

6
The high death rate from PE (exceeding acute MI!) and the high frequency of undiagnosed PE causing “sudden cardiac death” emphasize the need for improved preventive efforts. Failure to institute prophylaxis is a much bigger problem with Medical Service patients than Surgical Service patients. The high death rate from PE (exceeding acute MI!) and the high frequency of undiagnosed PE causing “sudden cardiac death” emphasize the need for improved preventive efforts. Failure to institute prophylaxis is a much bigger problem with Medical Service patients than Surgical Service patients.
 and the high frequency of undiagnosed PE causing sudden cardiac death emphasize the need for improved preventive efforts. Failure to institute prophylaxis is a much bigger problem with Medical Service patients than Surgical Service patients..")
7
Annual At-Risk for VTE: U.S. Hospitals ► 7.7 million Medical Service inpatients ► 3.4 million Surgical Service inpatients ► Based upon ACCP guidelines for VTE prophylaxis ► 7.7 million Medical Service inpatients ► 3.4 million Surgical Service inpatients ► Based upon ACCP guidelines for VTE prophylaxis Anderson FA Jr, et al. Am J Hematol; 2007; 82: 777-782

8
Outpatient and Inpatient VTE are Linked ► 74% of VTEs present in outpatients. ► 42% of outpatient VTE patients have had recent surgery or hospitalization. ► Only 40% had received VTE prophylaxis. ► 74% of VTEs present in outpatients. ► 42% of outpatient VTE patients have had recent surgery or hospitalization. ► Only 40% had received VTE prophylaxis. Spencer FA, et al. Arch Intern Med 2007; 167: 1471-1475

9
ICOPER Cumulative Mortality Mortality (%) Days From Diagnosis 17.5% 0 5 10 15 20 25 714306090 Lancet 1999; 353: 1386-1389
 Days From Diagnosis 17.5% Lancet 1999; 353:")
11
Progression of Chronic Venous Insufficiency From UpToDate 2006

12
Cardiovascular Risk Factors and VTE (N=63,552 meta-analysis) RFRR Obesity2.3 Hypertension1.5 Diabetes1.4 Cigarettes1.2 High Cholesterol1.2 RFRR Obesity2.3 Hypertension1.5 Diabetes1.4 Cigarettes1.2 High Cholesterol1.2 Ageno W. Circulation 2008; 117: 93-102

13
Steffen LM. Circulation 2007;115:188-195 Eat Veggies and Lower VTE Risk; Careful with Red Meat Adjusted Hazard Ratios (Quintiles) 2345p Fruits, veggie 0.730.570.47 0.59 0.03 Fish 0.580.600.55 0.70 0.30 Red Meat 1.241.211.09 2.01 0.02
 2345p Fruits, veggie Fish Red Meat")
14
Dabish 20-Year Cohort: VTE, Subsequent CV Events ► Assessed risk of MI, Stroke ► 25,199 with DVT ► 16,925 with PE ► 163,566 population controls ► Assessed risk of MI, Stroke ► 25,199 with DVT ► 16,925 with PE ► 163,566 population controls Sorensen HT. Lancet 2007; 370: 1773-1779

15
RR CV Event in PE Patients CV Event 1 Year RR 2-20 Year RR Acute MI 2.61.3 Stroke2.91.3 Sorensen HT. Lancet 2007; 370: 1773-1779

16
Reversible Risk Factors 1.Nutrition: eat fruits, veggies, fish; less red meat 2.Quit cigarettes 3.Lose weight/ exercise 4.Prevent DM/ metabolic syndrome 5.Control hypertension 6.Lower cholesterol 1.Nutrition: eat fruits, veggies, fish; less red meat 2.Quit cigarettes 3.Lose weight/ exercise 4.Prevent DM/ metabolic syndrome 5.Control hypertension 6.Lower cholesterol

17
DIAGNOSIS

18
PE SXS/ Signs (PIOPED II) ► Dyspnea (79%) ► Tachypnea (57%) ► Pleuritic pain (47%) ► Leg edema, erythema, tenderness, palpable cord (47%) ► Cough/ hemoptysis (43%) ► Dyspnea (79%) ► Tachypnea (57%) ► Pleuritic pain (47%) ► Leg edema, erythema, tenderness, palpable cord (47%) ► Cough/ hemoptysis (43%) Stein PD. Am J Med 2007; 120: 871-879

19
Clinical Decision Rule JAMA 2006; 295: 172-179

21
CT Leg Venography & U/S: Necessary or “Overkill”? ► Incremental value of CTV (N=829): 0.7% in low-risk patients and 2.6% in high risk patients (prior VTE, cancer). CTV more than doubles radiation dose (Hunsaker. AJR 2008; 190: 322-328) ► Chest CT alone (N=1,819) was noninferior to chest CT plus leg U/S. (Lancet 2008; 371: 1343-1352) ► Incremental value of CTV (N=829): 0.7% in low-risk patients and 2.6% in high risk patients (prior VTE, cancer). CTV more than doubles radiation dose (Hunsaker. AJR 2008; 190: 322-328) ► Chest CT alone (N=1,819) was noninferior to chest CT plus leg U/S. (Lancet 2008; 371: 1343-1352)
: 0.7% in low-risk patients and 2.6% in high risk patients (prior VTE, cancer). CTV more than doubles radiation dose (Hunsaker. AJR 2008; 190: ) ► Chest CT alone (N=1,819) was noninferior to chest CT plus leg U/S. (Lancet 2008; 371: ) ► Incremental value of CTV (N=829): 0.7% in low-risk patients and 2.6% in high risk patients (prior VTE, cancer). CTV more than doubles radiation dose (Hunsaker. AJR 2008; 190: ) ► Chest CT alone (N=1,819) was noninferior to chest CT plus leg U/S. (Lancet 2008; 371: ).")
22
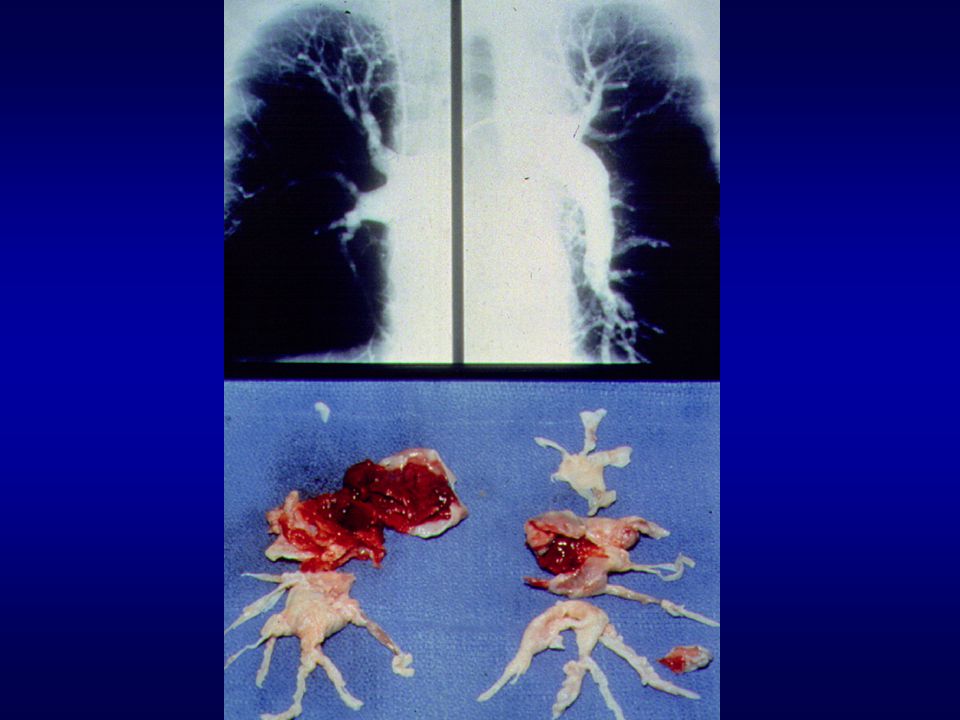
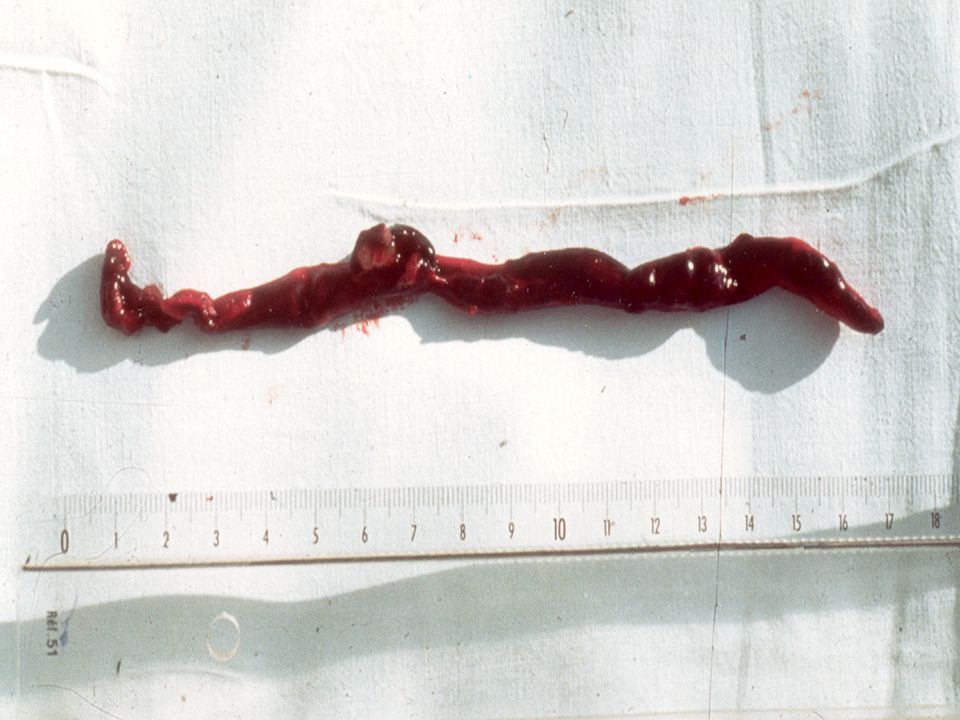
Saddle Embolus

23
PE Diagnosis Suspect PE: CXR, ECG, Oximetry CDR < 4 D-dimer High: get CT Normal: stop W/U CDR > 4 Chest CT Pos: Rx for PE Neg: stop W/U

24
Risk Stratification

25
Risk Stratification: PE is essential to decide: 1.Anticoagulation alone versus anticoagulation plus thrombolysis/ embolectomy 2.Triage to Intensive Care Unit 3.Consider RFs for fatal PE: massive PE, immobilization, age > 75 years, cancer. Risk Stratification: PE is essential to decide: 1.Anticoagulation alone versus anticoagulation plus thrombolysis/ embolectomy 2.Triage to Intensive Care Unit 3.Consider RFs for fatal PE: massive PE, immobilization, age > 75 years, cancer. Circulation 2008; 117: 1711-1716

26
TROPONIN META-ANALYSIS: Indicates RV Micro Infarct (Even “Leaks” Are Important) ► 1,985 patients from 20 PE studies ► 20% of 618 with elevated levels died ► 3.7% of 1,367 with WNL levels died ► In hemodynamically stable PE patients, elevated troponin levels increased mortality 6-fold. ► 1,985 patients from 20 PE studies ► 20% of 618 with elevated levels died ► 3.7% of 1,367 with WNL levels died ► In hemodynamically stable PE patients, elevated troponin levels increased mortality 6-fold. Circulation 2007; 116: 427-433

27
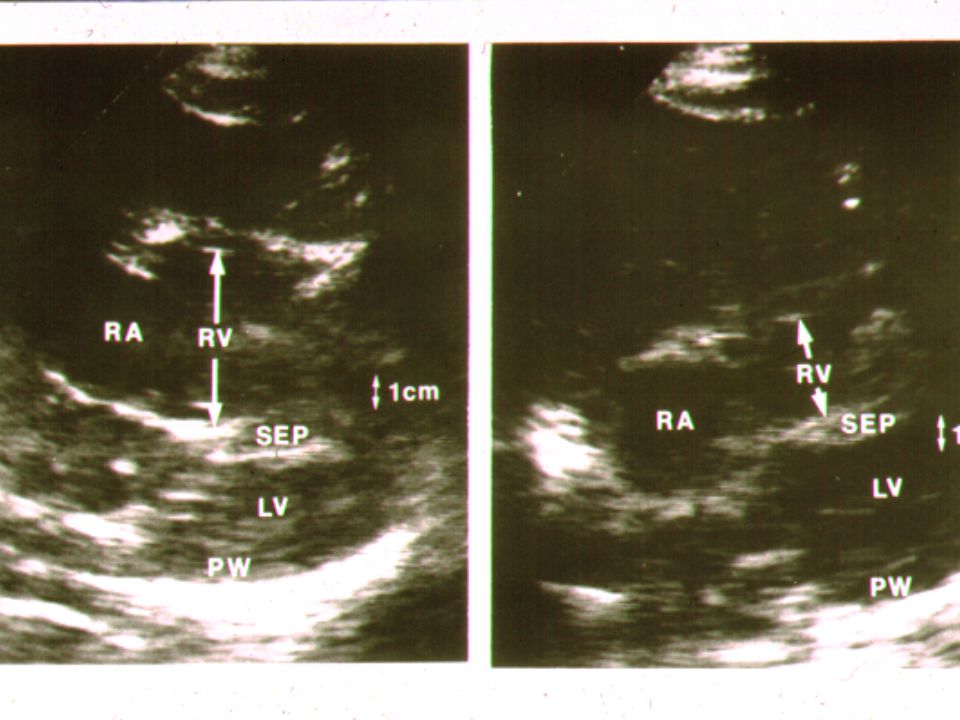
Risk Stratify PE: Assess RV Size, Function ► ECHO: RV/LV EDD > 0.9 predicts increased hospital mortality (OR=2.6) (Fremont B. CHEST 2008;133: 358) and recurrent (often fatal) PE (Arch Intern Med 2006; 166: 2151) ► Chest CT: an alternative to ECHO to compare RV/LV size ► ECHO: RV/LV EDD > 0.9 predicts increased hospital mortality (OR=2.6) (Fremont B. CHEST 2008;133: 358) and recurrent (often fatal) PE (Arch Intern Med 2006; 166: 2151) ► Chest CT: an alternative to ECHO to compare RV/LV size
 and recurrent (often fatal) PE (Arch Intern Med 2006; 166: 2151) ► Chest CT: an alternative to ECHO to compare RV/LV size ► ECHO: RV/LV EDD > 0.9 predicts increased hospital mortality (OR=2.6) (Fremont B. CHEST 2008;133: 358) and recurrent (often fatal) PE (Arch Intern Med 2006; 166: 2151) ► Chest CT: an alternative to ECHO to compare RV/LV size.")
28
RV ENLARGEMENT: CHEST CT Circulation 2004; 110: 3276

29
Treatment

30
VTE: Immediate Anticoagulation 1.Unfractionated heparin: target PTT between 60 to 80 seconds 2.Low molecular weight heparins: enoxaparin, dalteparin, tinzaparin 3.Fondaparinux 4.Direct thrombin inhibitors (HIT): argatroban, lepirudin, bivalirudin 1.Unfractionated heparin: target PTT between 60 to 80 seconds 2.Low molecular weight heparins: enoxaparin, dalteparin, tinzaparin 3.Fondaparinux 4.Direct thrombin inhibitors (HIT): argatroban, lepirudin, bivalirudin
: argatroban, lepirudin, bivalirudin 1.Unfractionated heparin: target PTT between 60 to 80 seconds 2.Low molecular weight heparins: enoxaparin, dalteparin, tinzaparin 3.Fondaparinux 4.Direct thrombin inhibitors (HIT): argatroban, lepirudin, bivalirudin")
31
Cancer and VTE ► 3-fold higher recurrence and bleeding, when treating cancer patients (Prandoni. Blood 2002; 100: 3484) ► LMWH Monotherapy halves recurrence, compared with warfarin. (Lee AYY. NEJM 2003; 349:146) (FDA approved May 2007) ► 3-fold higher recurrence and bleeding, when treating cancer patients (Prandoni. Blood 2002; 100: 3484) ► LMWH Monotherapy halves recurrence, compared with warfarin. (Lee AYY. NEJM 2003; 349:146) (FDA approved May 2007)
 ► LMWH Monotherapy halves recurrence, compared with warfarin. (Lee AYY. NEJM 2003; 349:146) (FDA approved May 2007) ► 3-fold higher recurrence and bleeding, when treating cancer patients (Prandoni. Blood 2002; 100: 3484) ► LMWH Monotherapy halves recurrence, compared with warfarin. (Lee AYY. NEJM 2003; 349:146) (FDA approved May 2007).")
32
Aggressive VTE Therapy ► Surgical embolectomy (Stein PD. Am J Cardiol 2007; 99: 421) ► Catheter embolectomy (Kucher N. CHEST 2007; 132: 657-663) ► PE Thrombolysis (Wan S. Circulation 2004; 110: 744) ► Catheter-based DVT therapies (Chang R. Radiology 2008; 246: 619) (Vasc Interv Radiol 2008; 19: 372-376) ► Surgical embolectomy (Stein PD. Am J Cardiol 2007; 99: 421) ► Catheter embolectomy (Kucher N. CHEST 2007; 132: 657-663) ► PE Thrombolysis (Wan S. Circulation 2004; 110: 744) ► Catheter-based DVT therapies (Chang R. Radiology 2008; 246: 619) (Vasc Interv Radiol 2008; 19: 372-376)
 ► Catheter embolectomy (Kucher N. CHEST 2007; 132: ) ► PE Thrombolysis (Wan S. Circulation 2004; 110: 744) ► Catheter-based DVT therapies (Chang R. Radiology 2008; 246: 619) (Vasc Interv Radiol 2008; 19: ) ► Surgical embolectomy (Stein PD. Am J Cardiol 2007; 99: 421) ► Catheter embolectomy (Kucher N. CHEST 2007; 132: ) ► PE Thrombolysis (Wan S. Circulation 2004; 110: 744) ► Catheter-based DVT therapies (Chang R. Radiology 2008; 246: 619) (Vasc Interv Radiol 2008; 19: ).")
33
47 EMERGENCY EMBOLECTOMIES Survival = 94 % J Thorac Cardiovasc Surg 2005;129:1018 N=47

34
Surgical Embolectomy at BWH: Surgeon’s Cell Phone

35
PE Thrombectomy Device Dimension: 11 French Spiral CoilSuction Ports

40
Heparin “Catches Up” with Lysis: Lung Perfusion Arch Intern Med 1997; 157: 2550

41
Thrombolysis in submassive PE remains controversial. A multinational European clinical trial (85 centers/ 12 countries) will enroll about 1,100 submassive PE patients with normal BP, elevated Troponin, and RV enlargement on ECHO. Reduce death/ CV collapse from 12.9% to 7.6% in 1 week? (1 st patient enrolled 11/10/2007; 65 th on 8/25/2008) Thrombolysis in submassive PE remains controversial. A multinational European clinical trial (85 centers/ 12 countries) will enroll about 1,100 submassive PE patients with normal BP, elevated Troponin, and RV enlargement on ECHO. Reduce death/ CV collapse from 12.9% to 7.6% in 1 week? (1 st patient enrolled 11/10/2007; 65 th on 8/25/2008)
 will enroll about 1,100 submassive PE patients with normal BP, elevated Troponin, and RV enlargement on ECHO. Reduce death/ CV collapse from 12.9% to 7.6% in 1 week. (1 st patient enrolled 11/10/2007; 65 th on 8/25/2008) Thrombolysis in submassive PE remains controversial. A multinational European clinical trial (85 centers/ 12 countries) will enroll about 1,100 submassive PE patients with normal BP, elevated Troponin, and RV enlargement on ECHO. Reduce death/ CV collapse from 12.9% to 7.6% in 1 week. (1 st patient enrolled 11/10/2007; 65 th on 8/25/2008).")
42
LYSIS VS. Filter: Massive PE (N=108) Lysis Filter
 Lysis Filter")
43
8 YEAR F/U IVC FILTERS: RCT PREPIC. Circulation 2005; 112: 416-422

44
BARD RECOVERY FILTER

46
Risks for Recurrence ► “Unprovoked” ► Strong FH; PMH of VTE ► Antiphospholipid antibody syndrome ► Cancer ► Male (Kyrle PA. NEJM 2004; 350: 2558) (McRae S. Lancet 2006; 368: 371-8) ► Presentation with PE Symptoms ► “Unprovoked” ► Strong FH; PMH of VTE ► Antiphospholipid antibody syndrome ► Cancer ► Male (Kyrle PA. NEJM 2004; 350: 2558) (McRae S. Lancet 2006; 368: 371-8) ► Presentation with PE Symptoms Eichinger. Arch Intern Med 2004;164: 92)
 (McRae S. Lancet 2006; 368: 371-8) ► Presentation with PE Symptoms ► Unprovoked ► Strong FH; PMH of VTE ► Antiphospholipid antibody syndrome ► Cancer ► Male (Kyrle PA. NEJM 2004; 350: 2558) (McRae S. Lancet 2006; 368: 371-8) ► Presentation with PE Symptoms Eichinger. Arch Intern Med 2004;164: 92).")
47
Trials of Unprovoked VTE : Favor Indefinite Duration Anticoagulation (NEJM 2003) TRIAL TAKE-HOME POINT. TRIAL TAKE-HOME POINT. PREVENTLow intensity A/C (INR 1.5-2.0) reduces recurrence rate by 2/3. ELATEStandard A/C (INR 2.0-3.0) is more effective but as safe as low intensity A/C. THRIVE-3Ximelagatran effective, safe. TRIAL TAKE-HOME POINT. TRIAL TAKE-HOME POINT. PREVENTLow intensity A/C (INR 1.5-2.0) reduces recurrence rate by 2/3. ELATEStandard A/C (INR 2.0-3.0) is more effective but as safe as low intensity A/C. THRIVE-3Ximelagatran effective, safe.
 reduces recurrence rate by 2/3. ELATEStandard A/C (INR ) is more effective but as safe as low intensity A/C. THRIVE-3Ximelagatran effective, safe. TRIAL TAKE-HOME POINT. TRIAL TAKE-HOME POINT. PREVENTLow intensity A/C (INR ) reduces recurrence rate by 2/3. ELATEStandard A/C (INR ) is more effective but as safe as low intensity A/C. THRIVE-3Ximelagatran effective, safe..")
48
Does Thrombophilia Predict Recurrent VTE? ► 474 VTE patients followed for an average of 7 years. ► Most patients were anticoagulated for < 12 months. ► 90 (20%) suffered recurrence. ► Thrombophilia did not increase likelihood of recurrence. ► 474 VTE patients followed for an average of 7 years. ► Most patients were anticoagulated for < 12 months. ► 90 (20%) suffered recurrence. ► Thrombophilia did not increase likelihood of recurrence. Christiansen SC. JAMA 2005; 293: 2352
 suffered recurrence. ► Thrombophilia did not increase likelihood of recurrence. ► 474 VTE patients followed for an average of 7 years. ► Most patients were anticoagulated for < 12 months. ► 90 (20%) suffered recurrence. ► Thrombophilia did not increase likelihood of recurrence. Christiansen SC. JAMA 2005; 293:")
49
How Often and For How Long Does CT Remain Abnormal After PE? F/UABNORMAL 6 Weeks68% 3 Months65% 6 Months57% 11 Months52% Nijkeuter M. CHEST 2006; 129: 192-197

50
Warfarin Pharmacogenomics 1.Cytochrome P450 2C9 genotyping can identify mutations associated with impaired warfarin metabolism. 2.Vitamin K receptor polymorphism testing can identify whether patients require low, intermediate, or high doses of warfarin. 1.Cytochrome P450 2C9 genotyping can identify mutations associated with impaired warfarin metabolism. 2.Vitamin K receptor polymorphism testing can identify whether patients require low, intermediate, or high doses of warfarin. Schwartz UI. NEJM 2008; 358: 999

51
► Rapid turnaround CYP2C9 and VKORC1 testing vs. “empiric” ► Primary endpoint: TTR ► Smaller and fewer dosing changes with genetic testing ► No difference in TTR ► Rapid turnaround CYP2C9 and VKORC1 testing vs. “empiric” ► Primary endpoint: TTR ► Smaller and fewer dosing changes with genetic testing ► No difference in TTR Genotype vs Standard Warfarin Dosing (n=206) Couma-Gen Trial Circulation 2007; 116: 2563-2570
 Couma-Gen Trial Circulation 2007; 116:")
52
Self-Monitoring INR: Meta-Analysis of 14 RCTS ► Reduced TE events (55% fewer) ► Reduced all-cause mortality (39% less) ► Reduced major bleeds (35% fewer) Benefits increase further with self-dosing ► 73% fewer TE events ► 63% lower all-cause mortality Heneghan C. Lancet 2006; 367: 404-411 ► Reduced TE events (55% fewer) ► Reduced all-cause mortality (39% less) ► Reduced major bleeds (35% fewer) Benefits increase further with self-dosing ► 73% fewer TE events ► 63% lower all-cause mortality Heneghan C. Lancet 2006; 367: 404-411
 ► Reduced all-cause mortality (39% less) ► Reduced major bleeds (35% fewer) Benefits increase further with self-dosing ► 73% fewer TE events ► 63% lower all-cause mortality Heneghan C. Lancet 2006; 367:")
53
March 19, 2008: Medicare Expanded Reimbursement for Home INR Monitoring ► Medicare used to cover only mechanical heart valves ► Now will reimburse VTE (after 3 months of warfarin) and chronic atrial fibrillation ► Aetna follows new Medicare guidelines (and surely others will, too) ► Medicare used to cover only mechanical heart valves ► Now will reimburse VTE (after 3 months of warfarin) and chronic atrial fibrillation ► Aetna follows new Medicare guidelines (and surely others will, too)
 and chronic atrial fibrillation ► Aetna follows new Medicare guidelines (and surely others will, too) ► Medicare used to cover only mechanical heart valves ► Now will reimburse VTE (after 3 months of warfarin) and chronic atrial fibrillation ► Aetna follows new Medicare guidelines (and surely others will, too)")
54
Novel Oral Anticoagulants 1.Dabigatran: an oral DTI—twice daily fixed dose (renal clearance) 2.Rivaroxaban: direct factor Xa inhibitor (renal clearance)—once daily fixed dose 3.Apixaban: direct factor Xa inhibitor (hepatic clearance)—twice daily fixed dose 1.Dabigatran: an oral DTI—twice daily fixed dose (renal clearance) 2.Rivaroxaban: direct factor Xa inhibitor (renal clearance)—once daily fixed dose 3.Apixaban: direct factor Xa inhibitor (hepatic clearance)—twice daily fixed dose Gross PL, Weitz JI; ATVB 2008; 28: 380)
 2.Rivaroxaban: direct factor Xa inhibitor (renal clearance)—once daily fixed dose 3.Apixaban: direct factor Xa inhibitor (hepatic clearance)—twice daily fixed dose 1.Dabigatran: an oral DTI—twice daily fixed dose (renal clearance) 2.Rivaroxaban: direct factor Xa inhibitor (renal clearance)—once daily fixed dose 3.Apixaban: direct factor Xa inhibitor (hepatic clearance)—twice daily fixed dose Gross PL, Weitz JI; ATVB 2008; 28: 380)")
55
Prevention

56
VTE Prophylaxis in 19,958 Medical Patients/ 9 Studies (Meta-Analysis) ► 62% reduction in fatal PE ► 57% reduction in fatal or nonfatal PE ► 53% reduction in DVT ► 62% reduction in fatal PE ► 57% reduction in fatal or nonfatal PE ► 53% reduction in DVT Dentali F, et al. Ann Intern Med 2007; 146: 278-288

57
Hull RD et al. July 2007; ISTH; Geneva EXCLAIM: Extended-Duration Enoxaparin Prophylaxis in High-Risk Medical Patients End points Outcome, extended prophylaxis, n=2052 (%) Outcome, placebo, n=2062 (%) RR reduction (%) p VTE events 2.8 2.8 4.9 4.9 44% 44%0.001 Symptomatic 0.3 0.3 1.1 1.1 73% 73%0.004 No Sxs 2.5 2.5 3.7 3.7 34% 34%0.032
 Outcome, placebo, n=2062 (%) RR reduction (%) p VTE events % 44%0.001 Symptomatic % 73%0.004 No Sxs % 34%")
58
The Amin Report: Prophylaxis Rates in the US ► Studied 196,104 Medical Service discharges from 227 hospitals (Premier® database). ► VTE prophylaxis rate was 62%. ► ACCP-deemed appropriate prophylaxis rate was 34%. ► Studied 196,104 Medical Service discharges from 227 hospitals (Premier® database). ► VTE prophylaxis rate was 62%. ► ACCP-deemed appropriate prophylaxis rate was 34%. J Thromb Haemostas 2007; 5: 1610-6
. ► VTE prophylaxis rate was 62%. ► ACCP-deemed appropriate prophylaxis rate was 34%. J Thromb Haemostas 2007; 5:")
59
Medical Patient Prophylaxis in Canada ► Studied 1,894 Medical Service discharges from 29 hospitals. ► VTE prophylaxis was indicated in 90% of patients. ► ACCP-deemed appropriate prophylaxis rate was 16%. ► Studied 1,894 Medical Service discharges from 29 hospitals. ► VTE prophylaxis was indicated in 90% of patients. ► ACCP-deemed appropriate prophylaxis rate was 16%. Thrombosis Research 2007; 119: 145-155

60
ENDORSE : WORLDWIDE (Lancet 2008; 371: 387-394) 68,183 patients; 32 countries; 358 sites First patient enrolled August 2, 2006;Last patient enrolled January 4, 2007
 68,183 patients; 32 countries; 358 sites First patient enrolled August 2, 2006;Last patient enrolled January 4, 2007")
61
42% at Risk for VTE Medical 40% receive ACCP Rec. Px 64% at Risk for VTE 59% receive ACCP Rec. Px Surgical Worldwide Prophylaxis Status for 68,183 Patients 52% at Risk for VTE (50% receive ACCP recommended prophy)
.")
62
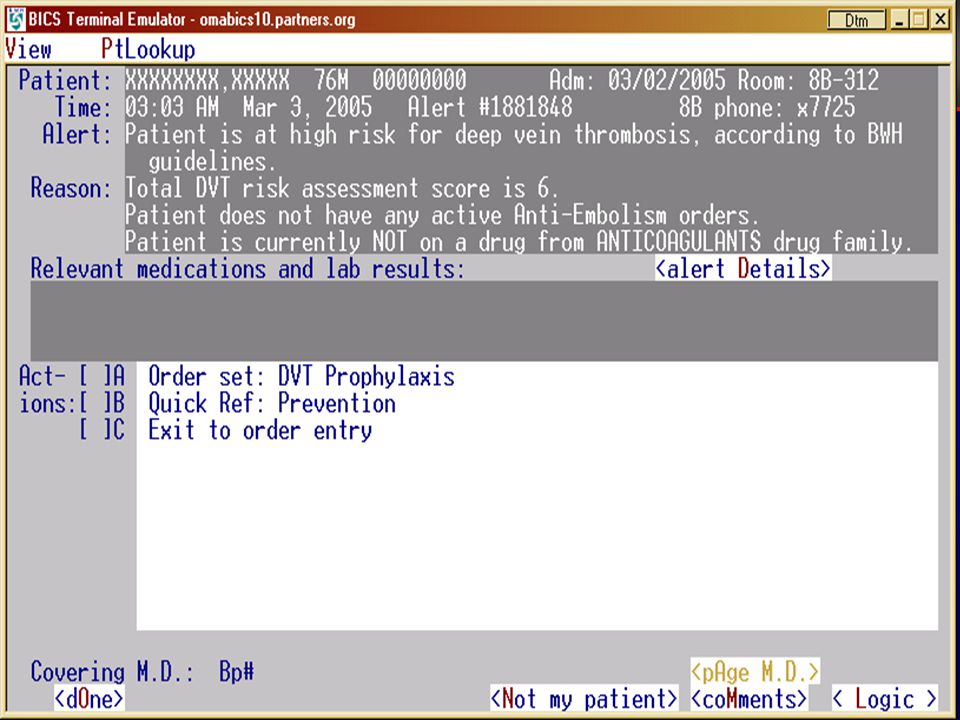
We have initiated trials to modify MD behavior and improve implementation of VTE prophylaxis—not trials of specific types of prophylaxis—electronic alerts and human alerts.

63
Definition of “High Risk” VTE risk score ≥ 4 points: ► Cancer3(ICD codes) ► Prior VTE3(ICD codes) ► Hypercoagulability3(Leiden, ACLA) ► Major surgery2(> 60 minutes) ► Bed rest1(“bed rest” order) ► Advanced age1(> 70 years) ► Obesity1(BMI > 29 kg/m 2 ) ► HRT/OC1(order entry) VTE risk score ≥ 4 points: ► Cancer3(ICD codes) ► Prior VTE3(ICD codes) ► Hypercoagulability3(Leiden, ACLA) ► Major surgery2(> 60 minutes) ► Bed rest1(“bed rest” order) ► Advanced age1(> 70 years) ► Obesity1(BMI > 29 kg/m 2 ) ► HRT/OC1(order entry)
 ► Prior VTE3(ICD codes) ► Hypercoagulability3(Leiden, ACLA) ► Major surgery2(> 60 minutes) ► Bed rest1( bed rest order) ► Advanced age1(> 70 years) ► Obesity1(BMI > 29 kg/m 2 ) ► HRT/OC1(order entry) VTE risk score ≥ 4 points: ► Cancer3(ICD codes) ► Prior VTE3(ICD codes) ► Hypercoagulability3(Leiden, ACLA) ► Major surgery2(> 60 minutes) ► Bed rest1( bed rest order) ► Advanced age1(> 70 years) ► Obesity1(BMI > 29 kg/m 2 ) ► HRT/OC1(order entry)")
64
Randomization VTE risk score > 4 No prophylaxis N = 2,506 INTERVENTION: Single alert N = 1,255 CONTROL No computer alert N = 1,251 Kucher N, et al. NEJM 2005;352:969-977

66
90-Day Primary Endpoint Intervent. Control Hazard Ratio p Intervent. Control Hazard Ratio p N=1255 N=1251 (95% CI) N=1255 N=1251 (95% CI) Total VTE 61 (4.9) 103 (8.2) 0.59 (0.43-0.81) 0.001 Total VTE 61 (4.9) 103 (8.2) 0.59 (0.43-0.81) 0.001 Acute PE 14 (1.1) 35 (2.8) 0.40 (0.21-0.74) 0.004 Acute PE 14 (1.1) 35 (2.8) 0.40 (0.21-0.74) 0.004 Proximal DVT 10 (0.8) 23 (1.8) 0.47 (0.20-1.09) 0.08 Proximal DVT 10 (0.8) 23 (1.8) 0.47 (0.20-1.09) 0.08 Distal DVT 5 (0.4) 12 (1.0) 0.42 (0.15-1.18) 0.10 Distal DVT 5 (0.4) 12 (1.0) 0.42 (0.15-1.18) 0.10 UE DVT 32 (2.5) 33 (2.6) 0.97 (0.60-1.58) 0.90 UE DVT 32 (2.5) 33 (2.6) 0.97 (0.60-1.58) 0.90 Intervent. Control Hazard Ratio p Intervent. Control Hazard Ratio p N=1255 N=1251 (95% CI) N=1255 N=1251 (95% CI) Total VTE 61 (4.9) 103 (8.2) 0.59 (0.43-0.81) 0.001 Total VTE 61 (4.9) 103 (8.2) 0.59 (0.43-0.81) 0.001 Acute PE 14 (1.1) 35 (2.8) 0.40 (0.21-0.74) 0.004 Acute PE 14 (1.1) 35 (2.8) 0.40 (0.21-0.74) 0.004 Proximal DVT 10 (0.8) 23 (1.8) 0.47 (0.20-1.09) 0.08 Proximal DVT 10 (0.8) 23 (1.8) 0.47 (0.20-1.09) 0.08 Distal DVT 5 (0.4) 12 (1.0) 0.42 (0.15-1.18) 0.10 Distal DVT 5 (0.4) 12 (1.0) 0.42 (0.15-1.18) 0.10 UE DVT 32 (2.5) 33 (2.6) 0.97 (0.60-1.58) 0.90 UE DVT 32 (2.5) 33 (2.6) 0.97 (0.60-1.58) 0.90 Kucher N, et al. NEJM 2005;352:969-977
 N=1255 N=1251 (95% CI) Total VTE 61 (4.9) 103 (8.2) 0.59 ( ) Total VTE 61 (4.9) 103 (8.2) 0.59 ( ) Acute PE 14 (1.1) 35 (2.8) 0.40 ( ) Acute PE 14 (1.1) 35 (2.8) 0.40 ( ) Proximal DVT 10 (0.8) 23 (1.8) 0.47 ( ) 0.08 Proximal DVT 10 (0.8) 23 (1.8) 0.47 ( ) 0.08 Distal DVT 5 (0.4) 12 (1.0) 0.42 ( ) 0.10 Distal DVT 5 (0.4) 12 (1.0) 0.42 ( ) 0.10 UE DVT 32 (2.5) 33 (2.6) 0.97 ( ) 0.90 UE DVT 32 (2.5) 33 (2.6) 0.97 ( ) 0.90 Intervent. Control Hazard Ratio p Intervent. Control Hazard Ratio p N=1255 N=1251 (95% CI) N=1255 N=1251 (95% CI) Total VTE 61 (4.9) 103 (8.2) 0.59 ( ) Total VTE 61 (4.9) 103 (8.2) 0.59 ( ) Acute PE 14 (1.1) 35 (2.8) 0.40 ( ) Acute PE 14 (1.1) 35 (2.8) 0.40 ( ) Proximal DVT 10 (0.8) 23 (1.8) 0.47 ( ) 0.08 Proximal DVT 10 (0.8) 23 (1.8) 0.47 ( ) 0.08 Distal DVT 5 (0.4) 12 (1.0) 0.42 ( ) 0.10 Distal DVT 5 (0.4) 12 (1.0) 0.42 ( ) 0.10 UE DVT 32 (2.5) 33 (2.6) 0.97 ( ) 0.90 UE DVT 32 (2.5) 33 (2.6) 0.97 ( ) 0.90 Kucher N, et al. NEJM 2005;352:")
67
Primary End Point Intervention Control Number at risk 1255977900853 1251976893839 Intervention Control Time (days) 0306090 %Freedom from DVT/ PE 90 92 94 96 98 100 Kucher N, et al. NEJM 2005;352:969-977

68
“Take Home” Points 1.VTE causes CVI, pulmonary hypertension, disability, and death. 2.Diagnose PE: CDR, D-dimer, CT. 3.Risk stratify PE patients: clinical evaluation, biomarkers, RV size/ function (ECHO/ CT)— ”window into future,” even if patient appears stable. 4.Thrombolysis remains controversial. 5.Consider indefinite duration anticoagulation for idiopathic VTE 6.Prophylaxis against PE/ DVT is crucial. 1.VTE causes CVI, pulmonary hypertension, disability, and death. 2.Diagnose PE: CDR, D-dimer, CT. 3.Risk stratify PE patients: clinical evaluation, biomarkers, RV size/ function (ECHO/ CT)— ”window into future,” even if patient appears stable. 4.Thrombolysis remains controversial. 5.Consider indefinite duration anticoagulation for idiopathic VTE 6.Prophylaxis against PE/ DVT is crucial.
— window into future, even if patient appears stable. 4.Thrombolysis remains controversial. 5.Consider indefinite duration anticoagulation for idiopathic VTE 6.Prophylaxis against PE/ DVT is crucial. 1.VTE causes CVI, pulmonary hypertension, disability, and death. 2.Diagnose PE: CDR, D-dimer, CT. 3.Risk stratify PE patients: clinical evaluation, biomarkers, RV size/ function (ECHO/ CT)— window into future, even if patient appears stable. 4.Thrombolysis remains controversial. 5.Consider indefinite duration anticoagulation for idiopathic VTE 6.Prophylaxis against PE/ DVT is crucial..")
69
Which Risk Factor is Most Predictive of Recurrent VTE (After Stopping Anticoagulation)? 1.Factor V Leiden 2.Prothrombin gene mutation 3.Postoperative state 4.Unprovoked, idiopathic VTE—etiology unknown 5.Birth control or pregnancy associated 1.Factor V Leiden 2.Prothrombin gene mutation 3.Postoperative state 4.Unprovoked, idiopathic VTE—etiology unknown 5.Birth control or pregnancy associated

70
Which Parameter is Most Predictive of a Benign Clinical Course After Diagnosis of PE? 1.Systolic BP between 110-130 mm Hg 2.HR between 60-80 bpm 3.RR between 12-16/minute 4.Normal right ventricular size and function on ECHO or CT 5.Absence of dyspnea or chest pain 1.Systolic BP between 110-130 mm Hg 2.HR between 60-80 bpm 3.RR between 12-16/minute 4.Normal right ventricular size and function on ECHO or CT 5.Absence of dyspnea or chest pain

Similar presentations











:>")










