Download presentation
Presentation is loading. Please wait.

1
Monitoring Renal Disease Gary Coxon BVetMed MRCVS Veterinary Advisor Vetoquinol UK and Ireland

2
Agenda Consequences of renal failure Aims of management Medications and monitoring

3
IRIS (International Renal Interest Society) Website at www.iris-kidney.comwww.iris-kidney.com Group of specialists that have created guidelines for Staging kidney disease Treatment at various stages of kidney disease in cats and dogs Good education section on proteinuria, urine collection, USG etc
 Website at Group of specialists that have created guidelines for Staging kidney disease Treatment at various stages of kidney disease in cats and dogs Good education section on proteinuria, urine collection, USG etc")
4
Renal Failure Multiple underlying causes with same outcome Progressive and dynamic condition Clinical signs vary and only appear when 66- 75% of functional tissue has been lost Replaced by fibrous or scar tissue GFR no longer adequate

5
Diagnosis Clinical signs Changes in urine specific gravity Changes in blood levels (Urea / Creatinine) Urine changes (specific gravity) Blood changes (urea/creat) ¾ Loss 2/3 Loss Clinical signProportion of cats affected Dehydration67% Anorexia64% Lethargy/depression52% Weight loss47% PU/PD32% Vomiting30% Macrorenale25% Microrenale19% Pale mucosae7% Oral ulceration5% Diarrhoea4% Retinal detachment4% Less common clinical signsHaematuria/dysuria, Poor coat, Halitosis, Osteodystrophy, Constipation
 Urine changes (specific gravity) Blood changes (urea/creat) ¾ Loss 2/3 Loss Clinical signProportion of cats affected Dehydration67% Anorexia64% Lethargy/depression52% Weight loss47% PU/PD32% Vomiting30% Macrorenale25% Microrenale19% Pale mucosae7% Oral ulceration5% Diarrhoea4% Retinal detachment4% Less common clinical signsHaematuria/dysuria, Poor coat, Halitosis, Osteodystrophy, Constipation")
6
Management Directed at complications of decreased kidney function “Conservative medical management” Needs to be monitored

7
Goals of Management Correct imbalances and deficits in fluids and electrolytes Limit progressive loss of functional tissue Manage clinical signs Ensure adequate but correct nutrition

8
Major Factors That Lead to Progression HYPERPHOSPHATEMIA HYPERTENSION and PROTEINURIA FIBROSIS (Scarring) NEPHRON LOSS
 NEPHRON LOSS")
9
1. Hyperphosphataemia and its consequences Controlling phosphate proven to increase life expectancy The earlier treatment is started the better the prognosis Prevent mineralisation and therefore prevent chronic inflammation Complexes and mineralisation PTH also mobilises calcium Only helps a little but PTH is still produced ↑PTH has effect to ↑phosphate clearance ↑Serum phosphate = hyperphosphataemia ↓ Phosphate excretion ↓GFR (Renal disease) Renal secondary hyperparathyroidism
 Renal secondary hyperparathyroidism.")
10
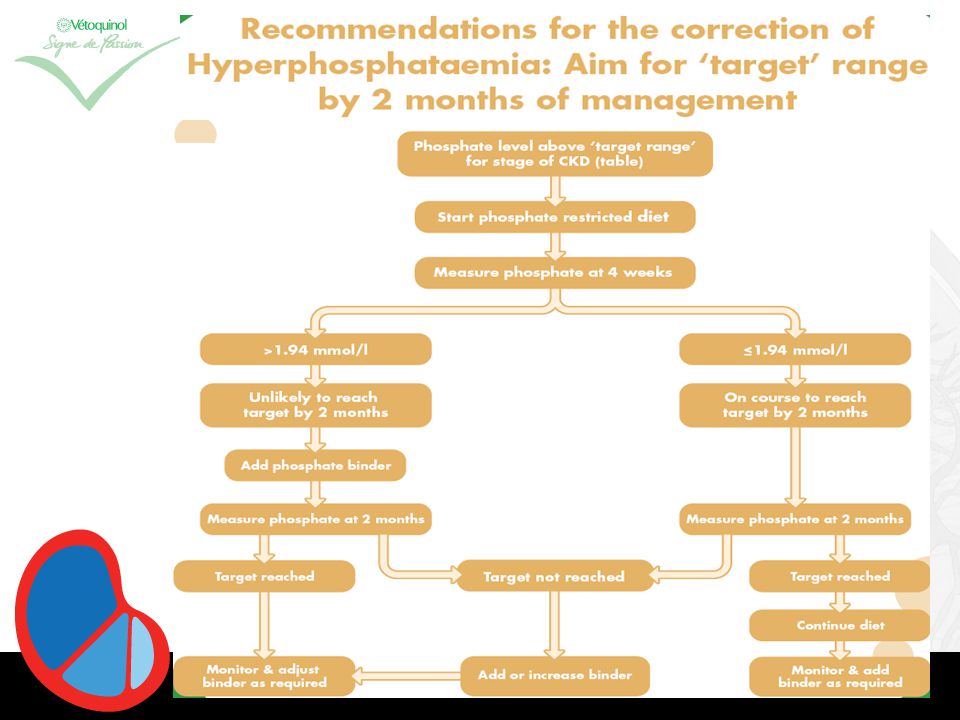
Phosphate Management Restrict dietary phosphorus Decrease intake Decrease absorption eg. Ipakitine Maintain phosphate in levels set out by experts Gives extension to lifespan

12
Serum Phosphate Establish “stage” of renal failure IRIS guidelines ( www.iris-kidney.com )www.iris-kidney.com Look up target phosphate level Adjust phosphate binder and/or food
 Look up target phosphate level Adjust phosphate binder and/or food")
13
Target Phosphate Levels

14
“ Normal ” serum phosphate ranges recommended by commercial laboratories and in-house analyzers for cats

18
Formulations 50g 150g 1g/5kg BID MUST be added to food

20
2. Systemic Hypertension May be a cause or consequence of renal disease Occurs in up to 66% of cats with CRF Causes end organ damage – renal, ocular, CNS In the kidney persistent glomerular hypertension lead to hypertensive damage and nephron death Reduction in GFR Activation of RAAS Angiotensin II CO and peripheral vascular resistance BP

22
Treatment of Hypertension Calcium channel blocker Amlodipine (Istin) 5mg tablets Typical dose 0.625-1.25mg/cat SID 1/8 – 1/4 tablet! Aim to get BP<170mmHg Adjust dose as necessary ACE inhibitors Not the most effective for systemic hypertension May be used if amlodipine alone isnt effective

23
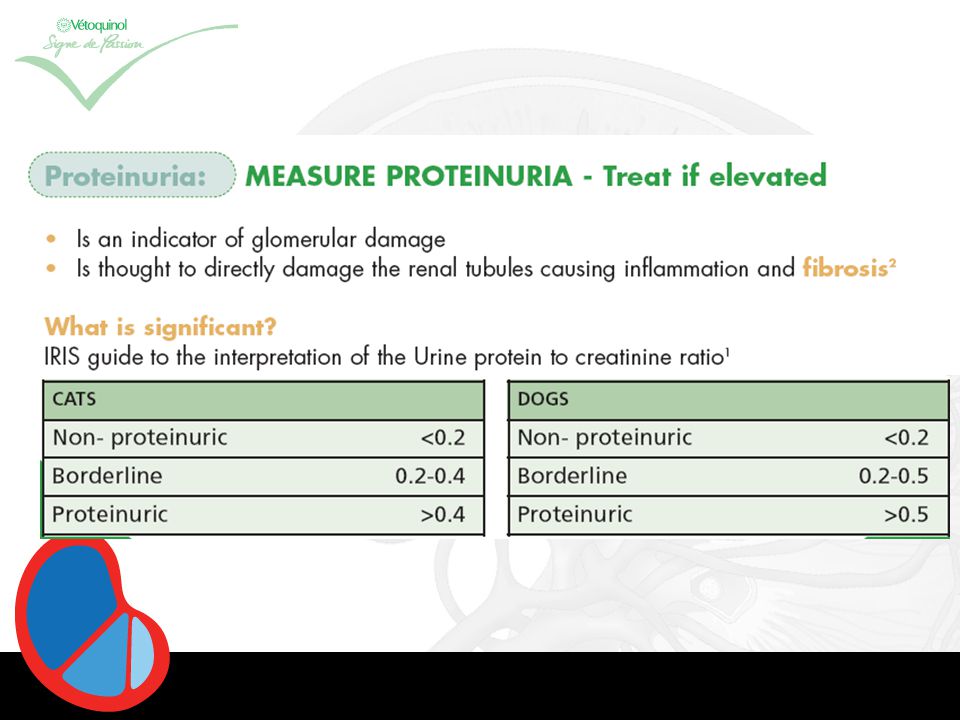
3. Proteinuria Is a marker of glomerular damage Glomerulonephritis Glomerular hypertension Amyloidosis Proteins directly damage the renal tubules causing further nephron loss Can be measured via Dipstick Urine Protein Creatinine Ratio (UP:C) Gives quantitative measure of protein and significance Prognostic indicator Treatment decisions Monitor response to treatment
 Gives quantitative measure of protein and significance Prognostic indicator Treatment decisions Monitor response to treatment.")
25
Treatment of Proteinuria Renal diet ACEi (if UP:C >0.4)
")
26
Tests Haematology Anaemia Biochemistry Urea, Creatinine, K+, Na+, Ca+, Phosphate, Proteins Urinalysis USG/dipstick, Sediment, Protein (UP:C), C&S Systolic BP
, C&S Systolic BP")
27
Case 1 – 13 y MN DSH Clinical signs PUPD, Lethargy, weight loss Bloods Urea – 14.3, Creatinine – 178, phosphate normal Urinalysis USG- 1.024, rest including UP:C normal Blood pressure 225mmHg Treatment?? Renal diet Amlodipine 1/8 tablet SID Aim to get BP<170mmHg

28
Case 2 – 8y MN Xbreed Clinical signs PUPD, lethargy, weight loss Bloods Urea-16.2, Creatinine-290, phosphate 2.3 (<1.61) Urinalysis USG-1.016, rest including UP:C normal Blood pressure 145 mmHg Treatment??? Renal diet and retest phosphate 4w later Phosphate 4w later – 1.97 Add in Ipakitine and aim for <1.61

29
Case 3 – 14y FN DSH Clinical signs PUPD, Lethargy, weight loss Bloods Urea-19.1, Creatinine-279, Phosphate – 2.7 (<1.61) Urinalysis USG 1.019, UP:C- 0.8 Blood Pressure 160 mmHg Treatment??? Renal diet ACE inhibitor But wouldn’t eat food so Ipakitine added to normal food Retest bloods(inc Phosphate) and UP:C in 4w
 and UP:C in 4w.")
30
QUESTIONS?

Similar presentations