Download presentation
Presentation is loading. Please wait.

1
Acetabular Fractures Joshua Landau, MD David Seidman, MD 11/23/04

2
Overview Radiographs Classification Treatment Options Surgical Approaches

3
Radiographic Evaluation From the lateral, acetabulum is inverted Y Anterior column Posterior column Sciatic notch through obturator and inferior pubic ramus

5
AP 6 Lines Iliopectineal Ilioischial Posterior wall Anterior wall Dome Teardrop

6
Radiographs AP 6 Lines Iliopectineal Ilioischial Posterior wall Anterior wall Dome Teardrop

7
Oblique

8
Iliac Oblique Posterior column Anterior wall

9
Iliac Oblique Posterior column Anterior wall

10
Iliac Oblique Posterior column Anterior wall

11
Oblique

12
Obturator Anterior column Posterior Wall

13
Obturator Oblique

14
The Dome

16
Weight Bearing Dome:Roof arc angle Vertical line through the rotational center of acetabulum Angled line through the fracture Mata: <45 deg on any view Recently: anterior <25 Medial <45 Posterior <70 Top of the dome distally for 1 cm on CT

17
Classification: Letournel and Judet

18
Classification: Special Notes Both column essentially a T type occurring proximal to the joint No portion of the articular surface is attached to axial skeleton SPUR SIGN Division of both columns ABOVE the acetabulum Secondary congruence

19
AP view

20
Obturator oblique view

21
Iliac oblique view

22
Representative CT cuts of the fracture, demonstrating that approximately 50 percent of the posterior wall is affected.

23
Posterior Wall Beware posterior hip dislocation Sometimes completely unstable Traction to maintain reduction until fixation Osteochondral fx common: require fixation/reduction if in weight bearing portion

24
Biomechanics Weight bearing portion: Primarily posterior and superior Hip stable <20% of posterior wall Hip unstable >40% of posterior wall

25
Posterior Wall Fracture Blood supply is from capsule: do not detach Flip over leaving capsule if possible

26
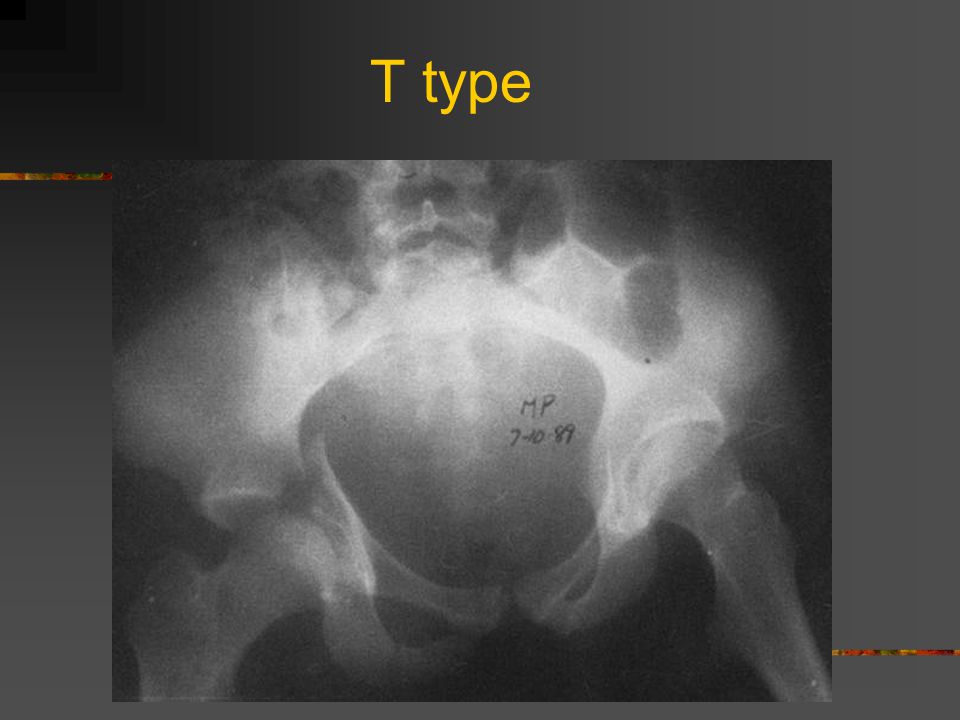
Anterior column + posterior hemitransverse vs. T type Reducing anterior column usually reduces posterior column, post capsule is not usually disrupted In contrast, in the T type, reducing the anterior does not reduce the posterior and the post capsule is disrupted

27
T type

29
Must involve obturator foramen

31
Both Column

33
Treatment options Nonoperative Traction NWB Indicated if displacement < 2mm Operative ORIF ORIF w/ THA Absolute indication is hip instability / subluxation out of traction

34
Operative vs. Non-op Classic Articles Rowe and Lowell: non-op is preferred Judet et. al: 90% good result if anatomic reduction, 74% good result overall Current Literature Rowe and Lowell 2 groups of fractures High energy forces, incongruous joint Operative management is better Low energy, minimal displacement Non-op management is satisfactory

35
Surgical Considerations Timing Surgery should be completed within 7 d results deteriorate after 3 weeks Approaches Iliofemoral Ilioinguinal Kocher-Langenbach Triradiate Extended Iliofemoral Combined

36
Iliofemoral Anterior column or anterior wall fractures w/ displacement cephalad to hip joint Lag screws into anterior column Plate only fits on crest of ilium, not on pelvic brim

37
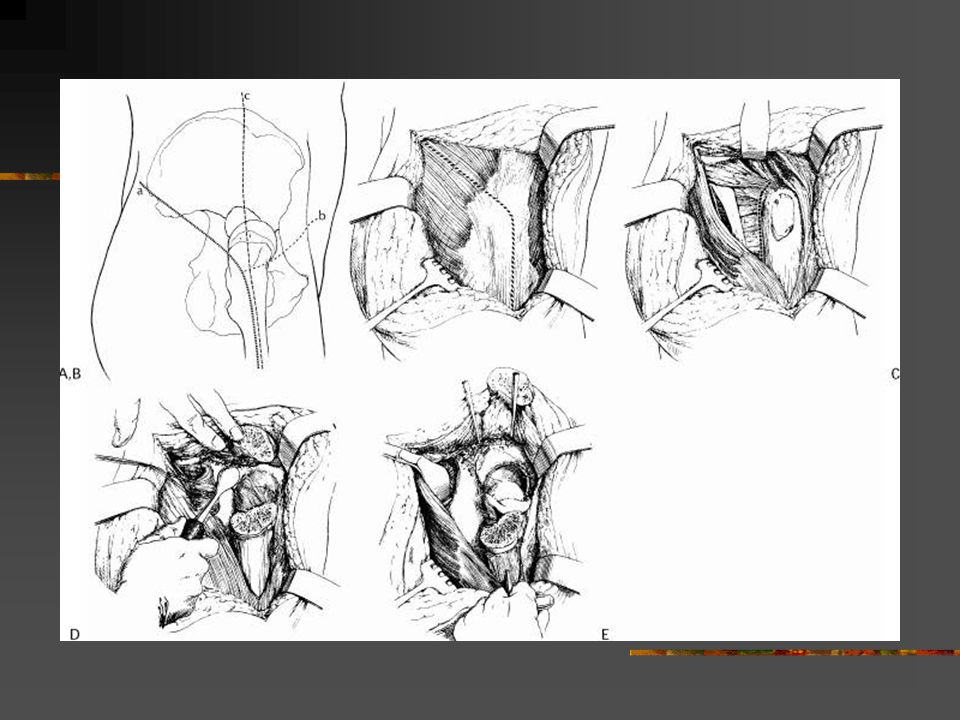
Ilioinguinal For anterior fractures where access to entire anterior column Can be used for both column fx only if posterior piece is large and intact Don’t see articular surface, only fx lines in pelvis Commonly sacrifice lateral cutaneous nerve of the thigh Divide external oblique from inguinal ring to asis, expose spermatic cord/round ligament Ligate inferior epigastric vessels

38
Ilioinguinal Complications: Femoral nerve injury LFCN Thrombosis in femoral vessels

39
Ilioinguinal Sling 1: iliopsoas Sling 2: external iliac artery and vein (aka femoral sheath) Sling 3: spermatic cord
 Sling 3: spermatic cord")
40
Kocher-Langenbach Isolated posterior wall or posterior column injuries only Exposure limited superiorly by superior gluteal vessels and greater trochanter High incidence of HO and sciatic injury May consider troch osteotomy Complications: Sciatic nerve 2-10% Damage to femoral head blood supply via medial femoral circumflex a.

42
Triradiate Both column fractures ASIS to top of sciatic notch is exposed Expose TFL, divide TFL and G. max Remove greater troch Capsulorrhaphy and joint exposure

43
Extended iliofemoral Exposes Outer table of ilium Superior dome Posterior column Anterior column to iliopubic eminence Provides exposure to bone above sciatic notch Highest risk for HO Also risk for superior gluteal artery injury leading to muscle necrosis

45
Approach by fracture type Kocher-Langenbach Posterior column Prone is best Weight of leg in lateral position causes rotation of posterior column Posterior wall Lateral is OK Posterior column + posterior wall Prone is best Anterior column + posterior hemitransverse Ilioinguinal approach usually adequate Transverse fxs Depends on location of displacement T type is most difficult

46
Approach by fracture type Both Column If posterior column is a single large fragment, then ilioinguinal approach is preferred If posterior column is not reduced, then add Kocher- Langenbach If significant posterior wall fracture, choose extensile or combined approach

47
Reduction Traction Fracture table Direct pull on femoral neck Corkscrew into femoral neck T handled bone hook on greater troch External distractors 5 or 6 mm Schanz threaded pin through the ischial tuberosity as joystick for T type or posterior column fxs Farabeuf clamps on screws inserted on either side of fx

48
Reduction Cerclage wires may help through the greater or lesser sciatic notch

49
Fixation Interfrag lag screws 3.5 mm cortical screws, even in cancellous bone No tap necessary except in dense bone of sciatic butress 3.5 mm recon plate contoured

50
Outcomes THA after ORIF of acetabulum does better than THA after unreduced acetabulum fx

51
Complications Thromboembolism: 60% of cases HO Use XRT or indomethacin peri/post op for prophylaxis w/ Kocher-Langenbach approach Neurologic injury AVN 18% of posterior fracture patterns Post-traumatic DJD Abductor weakness Intra-articular hardware

Similar presentations









 Pelvic girdle.>")














 Waleed M. Awwad, MD. FRCSC Assistant professor and Consultant Orthopedic Surgery department.>")