Download presentation
Presentation is loading. Please wait.

1
Beyond LDL Cholesterol: Reduction of Small Dense LDL and of Oxidized LDL With Combined Lipid Therapy
Rabih R. Azar, MD, MSc, FACC Associate Professor of Medicine Division of Cardiology Hotel Dieu de France Saint Joseph University

2
Risk of CAD according to LDL and HDL

5
IS LDL CHOLESTEROL THE “ONLY” PLAYER IN ATHEROSCLEROSIS?

6
Stages of Atherosclerosis
LUMEN LDL INTIMA Here the proposed mechanism of action of Lp-PLA2 in coronary heart disease is presented in graphic form Lp-PLA2 co-traffics in circulation with LDL-cholesterol LDL penetrates the intima where it undergoes oxidative modification MEDIA

7
Stages of Atherosclerosis
LUMEN Adhesion molecules Oxidized LDL Lp-PLA2 INTIMA Oxidized LDL is the favored substrate for the enzyme Lp-PLA2 Lp-PLA2 acts on oxidatively-modified phosphatidylcholine to produce lysophosphatidylcholine (lyso-PC) and oxidized fatty acid (oxFA) Lyso-PC triggers a host of pro-inflammatory activities, including the upregulation of adhesion molecules such as VCAM-1 and ICAM-1 Lyso-PC OxFA MEDIA
 and oxidized fatty acid (oxFA) Lyso-PC triggers a host of pro-inflammatory activities, including the upregulation of adhesion molecules such as VCAM-1 and ICAM-1. Lyso-PC. OxFA. MEDIA.")
8
Stages of Atherosclerosis
LUMEN Monocytes Plaque formation Cytokines Adhesion molecules Oxidized LDL Lp-PLA2 Foam cell INTIMA The pro-inflammatory actions of lysophosphatidylcholine (lyso-PC), as well as those of oxidized fatty acid (oxFA), result in a cascade of events leading to atherosclerotic plaque formation. The upegulation of adhesion molecules and the expression of cytokines result in the recruitment of monocytes to the intimal space Monocytes differentiate into macrophages that engulf the oxidized LDL, developing into foam cells Foam cells aggregate to form a fatty streak covered by a fibrous cap Cytokines and proteases secreted by the plaque break down the collagen within the fibrous cap, making it weak and prone to rupture Plaque rupture can result in the formation of an atherothrombotic clot that can block the artery, resulting in a coronary event This model also suggests that Lp-PLA2 is a novel therapeutic target; if its activity could be blocked, the sequence of events leading to plaque formation and rupture could be interrupted Macrophage Lyso-PC OxFA MEDIA
, as well as those of oxidized fatty acid (oxFA), result in a cascade of events leading to atherosclerotic plaque formation. The upegulation of adhesion molecules and the expression of cytokines result in the recruitment of monocytes to the intimal space. Monocytes differentiate into macrophages that engulf the oxidized LDL, developing into foam cells. Foam cells aggregate to form a fatty streak covered by a fibrous cap. Cytokines and proteases secreted by the plaque break down the collagen within the fibrous cap, making it weak and prone to rupture. Plaque rupture can result in the formation of an atherothrombotic clot that can block the artery, resulting in a coronary event. This model also suggests that Lp-PLA2 is a novel therapeutic target; if its activity could be blocked, the sequence of events leading to plaque formation and rupture could be interrupted. Macrophage. Lyso-PC. OxFA. MEDIA.")
9
Stages of Atherosclerosis
LUMEN LDL Monocytes Plaque formation Cytokines Adhesion molecules Oxidized LDL Lp-PLA2 Foam cell INTIMA The pro-inflammatory actions of lysophosphatidylcholine (lyso-PC), as well as those of oxidized fatty acid (oxFA), result in a cascade of events leading to atherosclerotic plaque formation. The upegulation of adhesion molecules and the expression of cytokines result in the recruitment of monocytes to the intimal space Monocytes differentiate into macrophages that engulf the oxidized LDL, developing into foam cells Foam cells aggregate to form a fatty streak covered by a fibrous cap Cytokines and proteases secreted by the plaque break down the collagen within the fibrous cap, making it weak and prone to rupture Plaque rupture can result in the formation of an atherothrombotic clot that can block the artery, resulting in a coronary event This model also suggests that Lp-PLA2 is a novel therapeutic target; if its activity could be blocked, the sequence of events leading to plaque formation and rupture could be interrupted Macrophage Lyso-PC OxFA MEDIA
, as well as those of oxidized fatty acid (oxFA), result in a cascade of events leading to atherosclerotic plaque formation. The upegulation of adhesion molecules and the expression of cytokines result in the recruitment of monocytes to the intimal space. Monocytes differentiate into macrophages that engulf the oxidized LDL, developing into foam cells. Foam cells aggregate to form a fatty streak covered by a fibrous cap. Cytokines and proteases secreted by the plaque break down the collagen within the fibrous cap, making it weak and prone to rupture. Plaque rupture can result in the formation of an atherothrombotic clot that can block the artery, resulting in a coronary event. This model also suggests that Lp-PLA2 is a novel therapeutic target; if its activity could be blocked, the sequence of events leading to plaque formation and rupture could be interrupted. Macrophage. Lyso-PC. OxFA. MEDIA.")
10
Risk of CAD according to LDL and HDL

11
Cholesterol distribution in CHD and non-CHD populations
In spite of major advances made in the screening, detection, and management of heart disease, a major need exists for more accurate ways to predict CV risk Approximately 50% of individuals diagnosed with coronary artery disease do not have high blood cholesterol levels Therefore, other factors must be involved Framingham Heart Study — 26-year follow-up 35% of CHD occurs in people with TC considered optimal (<200mg/dL) No CHD CHD Most of the focus on the prevention and treatment of coronary heart disease has been on the role of lipids, particularly cholesterol, and the identification and treatment of hypertension It has been shown that approximately 35% of individuals diagnosed with coronary artery disease have blood cholesterol levels that are within the recommended desirable range (<200 mg/dL) Data from the Framingham Heart Study 26-year follow-up shows that 50% of coronary heart disease cases occur in patients who have below-average total cholesterol levels (<240 mg/dL) Factors other than traditional risk factors appear to be involved in the development of atherosclerosis Castelli W. Atherosclerosis 1996;124(suppl):S1-S9 150 200 250 300 Total cholesterol (mg/dL) Adapted from Castelli W. Atherosclerosis 1996
 No CHD. CHD. Most of the focus on the prevention and treatment of coronary heart disease has been on the role of lipids, particularly cholesterol, and the identification and treatment of hypertension. It has been shown that approximately 35% of individuals diagnosed with coronary artery disease have blood cholesterol levels that are within the recommended desirable range (<200 mg/dL) Data from the Framingham Heart Study 26-year follow-up shows that 50% of coronary heart disease cases occur in patients who have below-average total cholesterol levels (<240 mg/dL) Factors other than traditional risk factors appear to be involved in the development of atherosclerosis. Castelli W. Atherosclerosis 1996;124(suppl):S1-S Total cholesterol (mg/dL) Adapted from Castelli W. Atherosclerosis")
12
Prevalence of major risk factors in men with CHD
Traditional risk factors are a useful first step in determining who could be at risk for a coronary event Exposure to one or more CHD risk factors is also highly prevalent in individuals who do not develop clinical CHD Less than 10% of patients have 3 or 4 major risk factors Secondary testing can be used to further stratify individuals for CHD risk 4 major risk factors 3 major risk factors 0 major risk factors 2 major risk factors 62.4% to 1 major risk factor In a meta-analysis compiling data from 14 clinical studies, it was determined that the majority of patients with CHD had 0 to 1 of the major modifiable risk factors associated with CHD Conversely, very few of these individuals had 3 or 4 of the major modifiable risk factors A similar analysis determined that the vast majority of clinical trial patients who did not develop CHD also had at least one major risk factor above desirable levels Assessment of the major modifiable risk factors is a critical first step in identifying individuals with elevated CHD risk, but does not always provide the necessary diagnostic and prognostic information to determine the clinical management strategy for every individual patient Further testing may be useful in determining the absolute risk of an individual with a single major risk factor Khot, et al. JAMA. 2003;290: 1 major risk factor N=87,869 4 Major modifiable risk factors: hypertension, smoking, hypercholesterolemia, diabetes Khot, et al. JAMA. 2003

17
Similar LDL Levels Do NOT Mean Similar Risk
Phenotype B LDL = 81 Phenotype A

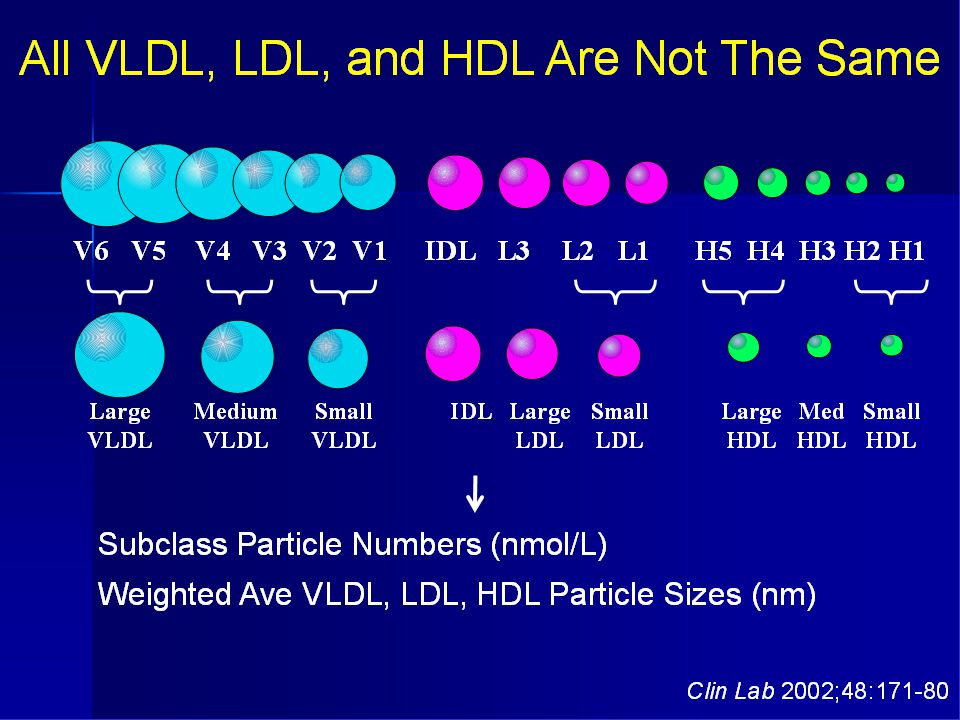
18
Small Dense LDL LDL particles are heterogeneous in size, density and composition. Individual can be classified according to their predominant LDL size into: Phenotype A: large particle size > 26.3 nm in diameter Phenotype B: Small particle size < 25.8 nm Phenotype I: Intermediate particle size, nm LDL phenotype B is in part genetically determined LDL phenotype B is also influenced by acquired conditions such as: Obesity Type 2 DM Metabolic syndrome

19
Mechanism of Increased Atherogenicity
Direct Mechanisms: Enhanced oxidative susceptibility Reduced clearance by LDL receptors in the liver with increased LDL receptor-independent binding in the arterial wall Endothelial dysfunction Indirect Mechanisms: Inverse relationship with HDL-C Marker for accumulation of atherogenic triglyceride remnant particles Insulin resistance

21
Inverse Relationship Between Small Dense LDL and HDL-C

22
The “Good” and “Bad” LDL
Large LDL subclasses 1 and 2 are the “good or normal” LDL that are responsible for the transport of cholesterol throughout the body Small LDL subclasses 3 through 7 are “bad or abnormal” that are easily oxidized and promote cardiovascular disease

23
Role of Small Dense LDL in Predicting Ischemic Heart Disease: The Quebec Cardiovascular Study
2034 men; all initially free of IHD Followed for 5 years 108 first IHD recorded Polyacrylamide gradient gel electrophoresis was used to measure small dense LDL Circulation 2001, 104:2295-9

24
The Quebec Cardiovascular Study: Risk Factors for IHD
Variable IHD free IHD Cases p Age <0.001 BMI 0.07 Systolic BP < 0.001 Type 2 DM 4.4% 14.8% 0.003 Cholesterol, mmol/L HDL, mmol/L 0.002 Cholesterol/HDL ratio TG, mmol/L Apo B, mg/L Lp(a), mg/dL 0.01
, mg/dL")
25
Small Dense LDL (<255Å) is the Best Predictor of Ishemic Heart Disease (IHD) in a Multivariate Model RRs of IHD according to baseline LDL, apoB, and TG and small dense LDL (proportion of small dense LDL above or below median of 39.6%). RR were adjusted for age, BMI, BP, DM, medication use at baseline and family history. Circulation 2001, 104:2295-9
. RR were adjusted for age, BMI, BP, DM, medication use at baseline and family history. Circulation 2001, 104:")
26
The Quebec Cardiovascular Study RESULTS:
Among all lipid parameters, small dense LDL (< 255 Å) showed the strongest association with the risk of IHD (RR in men = 4.6; p < 0.001) This was independent of all nonlipid risk factors and of LDL cholesterol, HDL, TG and Lp(a)
 showed the strongest association with the risk of IHD (RR in men = 4.6; p < 0.001) This was independent of all nonlipid risk factors and of LDL cholesterol, HDL, TG and Lp(a)")
27
LDL particle number and risk of future cardiovascular disease in the Framingham Offspring Study (J Clin Lipidol 2007;1:583-92)
")
30
Stages of Atherosclerosis
LUMEN Monocytes Plaque formation Cytokines Adhesion molecules Lp-PLA2 Foam cell Oxidized LDL INTIMA The pro-inflammatory actions of lysophosphatidylcholine (lyso-PC), as well as those of oxidized fatty acid (oxFA), result in a cascade of events leading to atherosclerotic plaque formation. The upegulation of adhesion molecules and the expression of cytokines result in the recruitment of monocytes to the intimal space Monocytes differentiate into macrophages that engulf the oxidized LDL, developing into foam cells Foam cells aggregate to form a fatty streak covered by a fibrous cap Cytokines and proteases secreted by the plaque break down the collagen within the fibrous cap, making it weak and prone to rupture Plaque rupture can result in the formation of an atherothrombotic clot that can block the artery, resulting in a coronary event This model also suggests that Lp-PLA2 is a novel therapeutic target; if its activity could be blocked, the sequence of events leading to plaque formation and rupture could be interrupted Macrophage Lyso-PC OxFA MEDIA
, as well as those of oxidized fatty acid (oxFA), result in a cascade of events leading to atherosclerotic plaque formation. The upegulation of adhesion molecules and the expression of cytokines result in the recruitment of monocytes to the intimal space. Monocytes differentiate into macrophages that engulf the oxidized LDL, developing into foam cells. Foam cells aggregate to form a fatty streak covered by a fibrous cap. Cytokines and proteases secreted by the plaque break down the collagen within the fibrous cap, making it weak and prone to rupture. Plaque rupture can result in the formation of an atherothrombotic clot that can block the artery, resulting in a coronary event. This model also suggests that Lp-PLA2 is a novel therapeutic target; if its activity could be blocked, the sequence of events leading to plaque formation and rupture could be interrupted. Macrophage. Lyso-PC. OxFA. MEDIA.")
31
Lipid entry into the vascular wall Content points:
After penetrating the arterial wall, LDL adheres to proteoglycans, which entrap it and increase its susceptibility to oxidation by lipoxygenases (LO), myeloperoxidase (MPO), and inducible nitric oxide synthase (iNOS).1 Scavenger receptors such as CD36 and SRA take up oxLDL, resulting in foam cell formation by macrophages. VLDL is modified by lipoprotein lipase (LPL) to form remnants that are trapped by proteoglycans, oxidized, and taken up by macrophages. 1 Li AC, Glass CK. The macrophage foam cell as a target for therapeutic intervention. Nat Med ;8:
, myeloperoxidase (MPO), and inducible nitric oxide synthase (iNOS).1. Scavenger receptors such as CD36 and SRA take up oxLDL, resulting in foam cell formation by macrophages. VLDL is modified by lipoprotein lipase (LPL) to form remnants that are trapped by proteoglycans, oxidized, and taken up by macrophages. 1 Li AC, Glass CK. The macrophage foam cell as a target for therapeutic intervention. Nat Med. 2002;8:")
33
Pro-atherogenic effects of oxidized LDL
Oxidized LDL is degraded at a faster rate than native LDL by macrophages leading to lipid accumulation. Oxidized LDL is chemotactic to monocytes, smooth muscle cells, and T lymphocytes, and induces T-cell activation and monocyte differentiation. Oxidized LDL inhibits macrophage motility, potentially trapping macrophages in the artery. Components of oxidized LDL are cytotoxic to cells. Oxidized LDL inhibits endothelium-dependent relaxation factor. Oxidized LDL enhances monocyte adhesion to endothelium. Oxidized LDL induces the expression of monocyte chemotactic protein-1 and granulocyte-macrophage colony stimulating factors. Oxidized LDL inhibits the migration of endothelial cells. Oxidized LDL induces the expression of adhesion molecules on the endothelium.Components of oxidized LDL induces interleukin-1 synthesis and secretion by macrophages

41
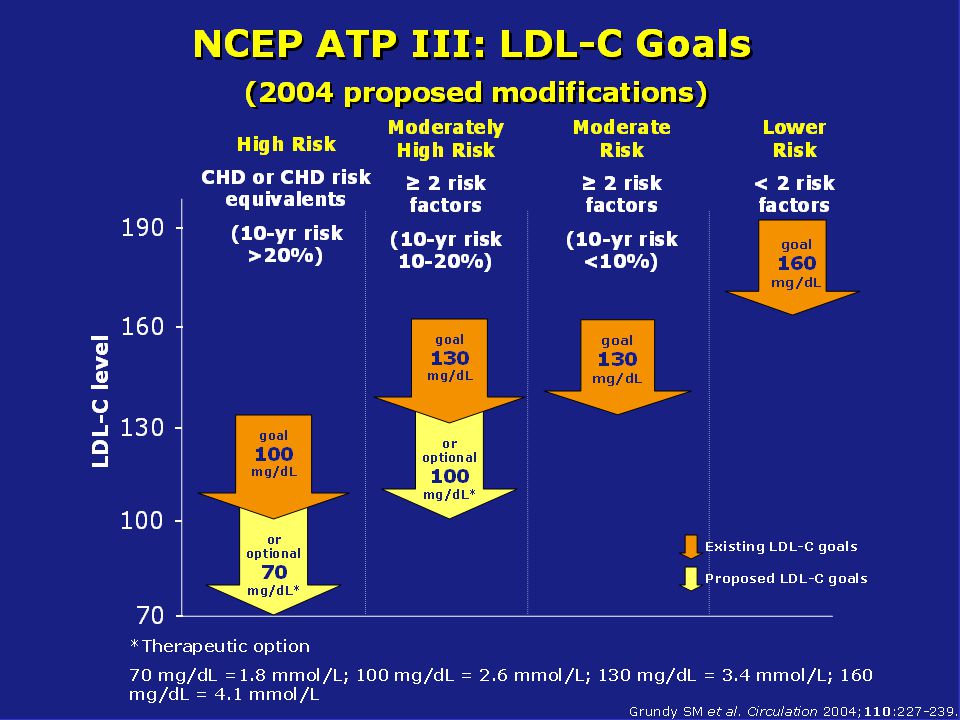
Refining cardiac risk assessment in asymptomatic patients
Initial risk assessment and physical examination Low risk 35% Intermediate risk 40% High risk 25% No major risk factors and low Framingham risk score At least one major risk factor or family history Established CHD or CHD risk equivalent Initial risk assessment and physical examination are the first steps in assessing absolute coronary risk Once this is done, a risk level should be determined for the individual patient and they should be counseled on their risk status Low-risk patients (35% of the population) should be provided reassurance of their low risk status and can avoid further risk assessment for about 5 years High-risk patients (25% of population) are candidates for intensive risk factor intervention and aggressive goals are recommended High-risk patients can have established CHD, other clinical forms of atherosclerosis, type 2 diabetes, or are older adults with multiple CHD factors According to the NCEP ATP III guidelines, such patients should have all of their CHD risk factors treated to reduce the risk of CHD and total cardiovascular disease Intermediate-risk patients (40% of population) do not qualify for the most intensive risk factor interventions; however, they may benefit from non-invasive testing for further risk assessment These individuals should be counseled about their intermediate CHD risk and offered general dietary and lifestyle modifications in order to reduce their risk. Some of these patients may be eligible to receive cholesterol-lowering drugs Further non-invasive testing can be useful in determining the most appropriate clinical strategy moving forward Greenland P, et al. Circulation. 2001;104: Further testing required to determine appropriate clinical direction 5-year follow up Intensive risk intervention CRP; Lp-PLA2; Small dense LDL; Ox LDL Greenland P, et al. Circ. 2001
 should be provided reassurance of their low risk status and can avoid further risk assessment for about 5 years. High-risk patients (25% of population) are candidates for intensive risk factor intervention and aggressive goals are recommended. High-risk patients can have established CHD, other clinical forms of atherosclerosis, type 2 diabetes, or are older adults with multiple CHD factors. According to the NCEP ATP III guidelines, such patients should have all of their CHD risk factors treated to reduce the risk of CHD and total cardiovascular disease. Intermediate-risk patients (40% of population) do not qualify for the most intensive risk factor interventions; however, they may benefit from non-invasive testing for further risk assessment. These individuals should be counseled about their intermediate CHD risk and offered general dietary and lifestyle modifications in order to reduce their risk. Some of these patients may be eligible to receive cholesterol-lowering drugs. Further non-invasive testing can be useful in determining the most appropriate clinical strategy moving forward. Greenland P, et al. Circulation. 2001;104: Further testing required to determine appropriate clinical direction. 5-year follow up. Intensive risk intervention. CRP; Lp-PLA2; Small dense LDL; Ox LDL. Greenland P, et al. Circ")
42
Effect of Ezetimibe/Atorvastatin Combination on Oxidized LDL-Cholesterol in Patients With CAD or CAD Equivallent Rabih Azar, Georges Badaoui, Antoine Sarkis, Mireille Azar, Hermine Aydanian, Serge Harb, Guy Achkouty and Roland Kassab Will be presented on March 14 at the Meeting of the American College of Cardiology in Atlanta, USA In press: J Am Coll Cardiol March 2010 (abstract) In press: Am J Cardiol July 2010 (manuscript) Sponsored by Pharmaline
 In press: Am J Cardiol July 2010 (manuscript) Sponsored by Pharmaline.")
43
RATIONAL Ox-LDL is a more potent predictor of cardiovascular risk than standard lipid parameters The majority of clinical trials have tested the efficacy of lipid lowering therapy against standard lipid parameters Rare trials: statins decrease ox-LDL Ezetimibe allows potent reductions of LDL when added to statin therapy The effect of ezetimibe on ox-LDL has however, never been studied This effect is important to investigate given the controversy surrounding ezetimibe’s use

44
RATIONAL Ox-LDL and small dense LDL are more potent predictors of cardiovascular risk than standard lipid parameters The majority of clinical trials have tested the efficacy of lipid lowering therapy against standard lipid parameters Few studies have shown that statins decrease ox-LDL. The effect of ezetimibe on ox-LDL is however, unknown This effect is important to investigate given the controversy surrounding ezetimibe’s use

45
OBJECTIVE TO EVALUATE THE EFFECT OF ATORVASTATIN 40 mg and of ATORVASTATIN 40 mg + EZETIMIBE ON OX-LDL CHOLESTEROL

46
Prospective, randomized, double-blind, placebo-controlled trial
Effect of Ezetimibe/Atorvastatin Combination on Oxidized LDL-Cholesterol in Patients With CAD or CAD Equivallent Prospective, randomized, double-blind, placebo-controlled trial Inclusion criteria: Patients with CAD > 50% stenosis on angiography MI PCI or CABG Patients with CAD equivalent Diabetes requiring medications Peripheral vascular disease Stroke Lipid levels were not entry criteria

47
Exclusion Criteria Therapy with a statin more potent than atorvastatin 20 mg/day (atorvastatin 40 or above, rosuvastatin any dose) Therapy with ezetimibe, any other cholesterol absorption inhibitor, niacine, fibrate within the last 3 months MI, CABG, PCI within the last 3 months Age > 80 years EF < 35% or CHF with NYHA class > 2 Creatinin clearance < 30 mL/min CPK or SGPT > 2 times upper normal

48
Study Protocol The statin taken by the patient was stopped and replaced by atorvastatin 40 mg/day Patients were then randomized to ezetimibe 10 mg/day vs. placebo Duration of treatment 8 weeks

49
MEASURMENTS Standard lipid profile (Total cholesterol, VLDL, LDL, HDL) LDL subfractions: small dense LDL and large buoyant LDL Mean LDL particle size Oxidized LDL CPK, SGPT

50
End-Points Primary end-point Secondary end-points Safety end-points
Change in ox-LDL Secondary end-points Change in small dense LDL Change in LDL particle size Safety end-points Elevation of CPK or SGPT more than twice upper normal

51
Inclusion Criteria n = 50 n = 50 Stenosis > 50% 19 (38%) 23 (46%)
Ezetimibe Placebo n = 50 n = 50 Stenosis > 50% 19 (38%) 23 (46%) Prior MI 18 (36%) 12 (24%) PCI 23 (46%) 15 (30%) CABG 26 (52%) 21 (42%) Diabetes 18 (36%) 21 (42%) Stroke 1 (2%) 1 (2%) PVD 6 (12%) 5 (10%) The number of inclusion criteria is superior to 100% because each patient may have more than 1 criterion that defines CAD
 23 (46%) Prior MI 18 (36%) 12 (24%) PCI 23 (46%) 15 (30%) CABG 26 (52%) 21 (42%) Diabetes 18 (36%) 21 (42%) Stroke 1 (2%) 1 (2%) PVD 6 (12%) 5 (10%) The number of inclusion criteria is superior to 100% because each patient may have more than 1 criterion that defines CAD.")
52
Baseline Characteristics
Ezetimibe Placebo n = 50 n = 50 Age (year) Male 44 (88%) 41 (82%) Smoking 14 (28%) 12 (24%) Hyperlipidemia 47 (94%) 43 (86%) Hypertension 35 (70%) 38 (76%) Fam. Hist. CAD 21 (42%) 14 (28%) BMI (kg/m2)
 Male 44 (88%) 41 (82%) Smoking 14 (28%) 12 (24%) Hyperlipidemia 47 (94%) 43 (86%) Hypertension 35 (70%) 38 (76%) Fam. Hist. CAD 21 (42%) 14 (28%) BMI (kg/m2)")
53
Concomitant Medications
Ezetemibe Placebo n = 50 n = 50 Aspirin 45 (90%) 43 (86%) Clopidogrel 11 (22%) 11 (22%) ACE inhb. or ARB 41 (82%) 34 (68%) Beta-blockers 37 (74%) 35 (70%) CCB 8 (16%) 18 (36%)* Nitrates 10 (20%) 11 (22%) Diuretics 6 (12%) 6 (12%) OAD 15 (30%) 17 (34%) Insulin 6 (12%) 6 (12%) * P = 0.02
 43 (86%) Clopidogrel 11 (22%) 11 (22%) ACE inhb. or ARB 41 (82%) 34 (68%) Beta-blockers 37 (74%) 35 (70%) CCB 8 (16%) 18 (36%)* Nitrates 10 (20%) 11 (22%) Diuretics 6 (12%) 6 (12%) OAD 15 (30%) 17 (34%) Insulin 6 (12%) 6 (12%) * P =")
54
Statin Use at Baseline 90% of patients were using a statin prior to randomization Simvastatin 53% Atorvastatin 30% Fluva or pravastatin 7% None 10%

55
Change in LDL in the Placebo/Atorva group
Additional 10% reduction in LDL when shifting to atorva 40 mg/day

56
Change in LDL 20% additional reduction 10% additional reduction
P < 0.001 P < 0.001 20% additional reduction 10% additional reduction Final LDL levels were lower in ezetimibe vs. placebo; p < 0.001

57
Change in Large, Buoyant LDL in the Placebo/Atorva Group
Additional 10% reduction in LDL when shifting to atorva 40 mg/day

58
Change in Large, Buoyant LDL
P < 0.001 P < 0.001 10% additional reduction 24% additional reduction Final levels ezetimibe vs. placebo: p = 0.007

59
Change in Small Dense LDL in the Placebo/Atorva Group
Additional 36% reduction in LDL when shifting to atorva 40 mg/day

60
Change in Small Dense LDL
P < 0.001 P < 0.001 36% additional reduction 32% additional reduction No difference between ezetimibe and placebo in lowering small dense LDL

61
Qualitative Lipid Analysis: Change in Particle Size
Particle Size in Angstrom Placebo/atorva: p = 0.002 Ezetimibe/atorva p = 0.006 Prevalence of type A phenotype increased from 62% to 70% in the placebo group and from 58% to 74% in the ezetimibe group

62
Change in VLDL in the Placebo/Atorva Group

63
Change in VLDL P = 0.07 P < 0.001

64
P = ns P = ns

65
Change in Ox-LDL p = NS p = 0.02 EZE Placebo EZE

67
Correlation Between the Changes in ox-LDL and Total LDL

68
Safety End-Point There was no elevation of CPK or SGPT in any patient of the 2 groups

69
Summary of Results: Change in Different Lipid Parameters
p = p = p = ns p = p = ns p = 0.02 Ezetimibe + Atorva Placebo + Atorva % reduction

70
Summary of Results: Effects of Atorvastatin and Ezetimibe on Various Lipid Parameters
LDL Large LDL Small dense LDL Particle size HDL VLDL Ox-LDL More potent statin Ezetimbe The changes induced by statin are quantitative and qualitative The Changes induced by ezetimibe are only quantitative

71
Conclusions Aggressive reduction of LDL is currently recommended for high risk patients Potent statins should be used as first line therapy In our study, increasing the potency of statin therapy by switching to atorvastatin 40mg: Did not affect ox-LDL Resulted in quantitative and qualitative improvement in lipid profile Was extremely safe and well tolerated Ezetimibe in combination with atorvastatin: Significantly decreased ox-LDL Resulted in quantitative improvement in lipid profile

Similar presentations

















 Clinical events (morbidity.>")



: Design Cannon CP.>")











 vs. placebo FU 5 years total cholesterol 25%; LDL.>")
>")