Download presentation
Presentation is loading. Please wait.

1
Chronic Kidney Disease Sumit Kumar, MD, MPH Presbyterian Hospital, Dallas, TX

2
The Story of Mr. George Lopez 45 yr HM with Diabetes for 10 yrs, “reasonably well controlled” PMH: Hypertension for 7 yrs..well controlled BMI of 30 Dyslipidemia Fam Hx: Diabetes; Soc Hx: Sedentary; non smoker; Comedian Exam 139/85 – Mild Obesity, rest fairly normal Labs BUN 28, Creatinine 1.8, Urine protein (dipstick) 2+
 2+.")
3
Chronic Kidney Disease Definition Chronic, irreversible loss of kidney function attributable to loss of functional nephron mass – pathophysiologic processes for more than 3 months.

4
Pathophysiology of CKD Final Common Pathway is loss of nephron mass Structural/ Functional Hypertrophy of remnant nephrons Sclerosis of remnant nephrons Loss of Nephron Mass Mediated by vasoactive molecules, cytokines and growth factors, renin angiotensin axis Diabetes Hypertension Chronic GN Cystic Disease Tubulointerstitial disease

5
Estimation of GFR Modification of Diet in Renal Disease (MDRD) Formula Estimated GFR = 1.86 (Serum Creat) -1.154 X (age) -0.203 Multiply by 0.742 for women Multiply by 1.21 for African Americans Cockroft Gault Formula (140 – age) X Body Weight (Kg) 72 X Serum Creatinine (mg/dL) Multiply by 0.85 for women
 Formula Estimated GFR = 1.86 (Serum Creat) X (age) Multiply by for women Multiply by 1.21 for African Americans Cockroft Gault Formula (140 – age) X Body Weight (Kg) 72 X Serum Creatinine (mg/dL) Multiply by 0.85 for women")
6
Staging of Chronic Kidney Disease StageDescriptionGFR (ml/min/1.73 m 2 ) At increased risk90 (with CKD risk factors) 1Kidney damage with normal or increased GFR 90 2Mildly decreased GFR60-89 3Moderately decreased GFR30-59 4Severely decreased GFR15-29 5Renal Failure<15 (or dialysis)
 At increased risk90 (with CKD risk factors) 1Kidney damage with normal or increased GFR 90 2Mildly decreased GFR Moderately decreased GFR Severely decreased GFR Renal Failure<15 (or dialysis)")
7
Who is at Risk for CKD? Family history of heritable renal disease Diabetes Hypertension Auto-immune disease Old age Prior episode of ARF Current evidence of renal damage, even with normal or increased GFR

8
MDRD GFR for Mr Lopez Diabetic, Hypertension, Metabolic Syndrome X Stage 3 CKD GFR = 44 ml/min/1.73 m 2

10
Etiology and Epidemiology 6% of the US population has CKD (Stage 1 and 2) Additional 4-5% have Stage 3 and 4 CKD Diabetic nephropathy Hypertension – chronic ischemic nephropathy Very high CV disease burden
 Additional 4-5% have Stage 3 and 4 CKD Diabetic nephropathy Hypertension – chronic ischemic nephropathy Very high CV disease burden")
11
Monitoring of CKD Serial measurements of Creatinine GFR Albumin Albumin-creatinine ratio in the 1 st morning sample Electrolytes including HCO 3, Ca, Phos; alkaline phosphatase, iron studies, intact PTH Renal sonogram Renal biopsy

12
Symptoms of CKD Stage 1 and 2 Asymptomatic, hypertension Stage 3 and 4 Anemia – loss of energy Decreasing appetite; poor nutrition Abnormalities in Calcium, Phosphorus metabolism Sodium, water, potassium and acid base abnormalities Stage 5 All of the above – accentuated; eventually overt uremia

14
Estimates of Subgroups at Increased Risk for CKD SubgroupEstimated Numbers Age > 70 yrs (8.8%)24 Million Hypertensive Patient (20%)50 Million Ethnicity (14.6%)? 38 Million Family History of ESRD? 2 Million

15
1992-931997-98 2002-03 Steady Rise in the Rate of CKD in Medicare population over the last decade

16
Common Causes and Presentation CauseClinical Presentation Diabetic kidney disease History of diabetes, proteinuria and retinopathy HypertensionElevated BP, normal UA, family history Non diabetic glomerular disease Nephritic or nephrotic presentations Cystic kidney disease Urinary symptoms, abnormal sediment, radiologic findings Tubulointerstitial disease UTI, reflux, chronic med use, drugs, imaging abnormalities, urine concentrating defects

17
Genetic Considerations Autosomal dominant PKD Alport’s hereditary nephritis Familial FSGS Nephronopthisis Medullary cystic kidney disease Fabry’s disease

23
Natural History of CKD Most CKD has a logarithmic progression and is predictable

24
Mr. Lopez – Progressive Decline

25
Clinical Features of Diabetic CKD

26
Clinical Features of Non-Diabetic CKD

27
Pathophysiology of Uremia Azotemia – refers to the retention of nitrogenous waste products. Uremia – advanced stages of azotemia with end organ dysfunction Accumulation of products of protein metabolism Urea – anorexia, malaise, vomiting and headaches Loss of other renal functions Erythropoietin deficiency – anemia Metabolic bone disease; endocrine abnormalities Fluid, electrolyte and acid base disorders

28
Organ SystemSymptomsSigns GeneralFatigue, weaknessSallow-appearing, chronically ill SkinPruritus, easy bruisabilityPallor, ecchymoses, excoriations, edema, xerosis ENTMetallic taste in mouth, epistaxisUrinous breath / fetor Eye Pale conjunctiva PulmonaryShortness of breathRales, pleural effusion CardiovascularDyspnea on exertion, retrosternal pain on inspiration (pericarditis) Hypertension, cardiomegaly, friction rub GastrointestinalAnorexia, nausea, vomiting, hiccups GenitourinaryNocturia, impotenceIsosthenuria NeuromuscularRestless legs, numbness and cramps in legs NeurologicGeneralized irritability and inability to concentrate, decreased libido Stupor, asterixis, myoclonus, peripheral neuropathy Symptoms of Uremia
 Hypertension, cardiomegaly, friction rub GastrointestinalAnorexia, nausea, vomiting, hiccups GenitourinaryNocturia, impotenceIsosthenuria NeuromuscularRestless legs, numbness and cramps in legs NeurologicGeneralized irritability and inability to concentrate, decreased libido Stupor, asterixis, myoclonus, peripheral neuropathy Symptoms of Uremia")
29
Sodium and water Imbalance Glomerulotubular feedback is disrupted – sodium retention, contributes to hypertension; hyponatremia is unusual. Higher than usual doses for diuretics. In situations with volume depletion – can be severe, because of inadequate sodium retention. Treatment: Salt restriction; high doses of diuretics

30
Potassium Imbalance Potassium GI excretion is augmented Constipation, dietary intake, protein catabolism, hemolysis, hemorrhage, transfusion of stored blood, metabolic acidosis, Drugs: ACE inhibitors, ARBs, B blockers, K sparing diuretics and NSAIDs Hyporeninemic hypoaldosteronism: Diabetes, sickle cell disease

31
Acid Base Imbalance Damaged kidneys are unable to excrete the 1 mEq/kg/d of acid generated by metabolism of dietary proteins. NH3 production is limited because of loss of nephron mass Decreased filtration of titrable acids – sulfates, phosphates Decreased proximal tubular bicarb reabsorption, decreased positive H ion secretion Arterial pH: 7.33 - 7.37; serum HCO3 rarely below 15 – buffering offered by bone calcium carbonate and phosphate Should be maintained over 21 Treatment: Sodium bicarbonate, calcium carbonate, sodium citrate

32
Bone Disease

33
Treatment of Secondary Hyperparathyroidism Phosphorus control in diet Phosphate binders Calcium acetate (Phoslo), calcium carbonate (TUMS), sevelamer (Renagel), lanthanum (Fosrenol) Oral Vitamin D Calcimemetic agent: Cinacalcet (Sensipar)
, calcium carbonate (TUMS), sevelamer (Renagel), lanthanum (Fosrenol) Oral Vitamin D Calcimemetic agent: Cinacalcet (Sensipar)")
34
Mineral Metabolism Calciphylaxis Calcemic uremic arteriopathy Extraosseous/metastatic calcification of soft tissues and blood vessels Devastating complication Treatment: controversial Sodium thiosulfate Parathyroidectomy

35
Cardiovascular Abnormalities Leading cause of morbidity and mortality in patients with CKD at all stages Ischemic CAD Hypertension and LVH Congestive heart failure Uremic pericarditis

36
Trends in the interactions of diabetes, congestive heart failure, & CKD: 2002- 2003 LVH and dilated CM are the most ominous risk factors for excess mortality and morbidity High cardiac output Extracellular fluid overloa AV shunt Anemia Medicare: general Medicare CKD patients continuously enrolled in Medicare Parts A & B for two consecutive years (numbers estimated from 5 percent sample)
")
37
Cardiac Complications

38
Hematological Abnormalities Anemia Chronic blood loss, hemolysis, marrow suppression by uremic factors, and reduced renal production of EPO Normocytic, normochromic Rx: Iron and Epo as needed Coagulopathy Mainly platelet dysfunction – decreased activity of platelet factor III, abnormal platelet aggregation and adhesiveness and impaired thrombin consumption Increased propensity to bleed – post surgical, GI Tract, pericardial sac, intracranial Increased thrombotic tendency – nephrotic syndrome

39
Other Abnormalities Neuromuscular Central, peripheral and autonomic neuropathy Peripheral Sensory/Motor Neuropathy Stage 4 for more than 6 months Restless leg syndrome Gastrointestinal Uremic fetor Gastritis, peptic disease, mucosal ulcerations, AVMs Endocrine Glucose metabolism Estrogen levels – amenorrhea, frequent abortions Male: oligospermia, germinal cell dysplasia, delayed sexual maturation Dermatologic Pallor, ecchymoses, hematomas, calciphylaxis, pruritus, uremic frost

40
Uremic Complications

41
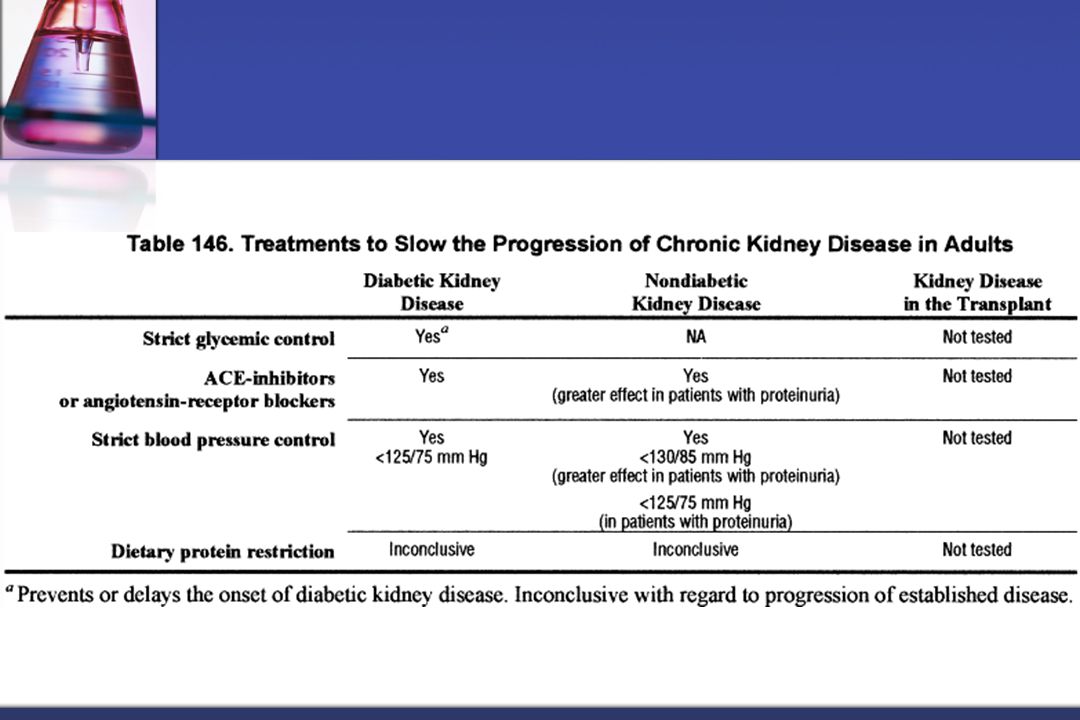
Therapeutics in CKD Non Pharmacologic Risk Factor Modification Pharmacologic Treatment of complications

43
Therapeutics in CKD Non Pharmacologic Risk Factor Modification Pharmacologic Treatment of complications

45
Therapeutics in CKD Non Pharmacologic Risk Factor Modification Pharmacologic Treatment of complications

Similar presentations











activate vitamin D (renal 1-alpha hydroxylase) produces erythropoietin.>")

>")




 Dr. Belal Hijji, RN, PhD April 18 & 23, 2012.>")









 RENAL DISEASE: CHRONIC RENAL FAILURE Pathophysiology of Disease: Chapter 16 (394-398) Jack DeRuiter, PhD.>")
