Download presentation
Presentation is loading. Please wait.

1
Pressure Ulcer Prevention and Wound and Skin Documentation Update 2009

2
Significance: Law suites related to hospital acquired pressure ulcers can range from &100,000 to $1,000,000.

3
The cost: Hospital acquired pressure ulcers increase cost and length of stay for patients. Estimated cost for hospital acquired pressure ulcers can be up to $70,000. Not to mention the pain and suffering of patients who acquire pressure ulcers during their hospital stay.

4
“Never events” Hospital acquired pressure ulcers are one of the “never events” as defined by CMS that should never happen in a hospital

5
S-K-I-N Bundle The Skin Bundle has been implemented successfully at hospitals using evidence- based interventions outlined in the Institute for Health Care Improvement (IHI) 100,000 Lives Campaign.
 100,000 Lives Campaign.")
6
What is the Skin Bundle S urface Selection K eep Repositioning I ncontinence Management N utritional Support S-K-I-N is an acronym that stands for:

7
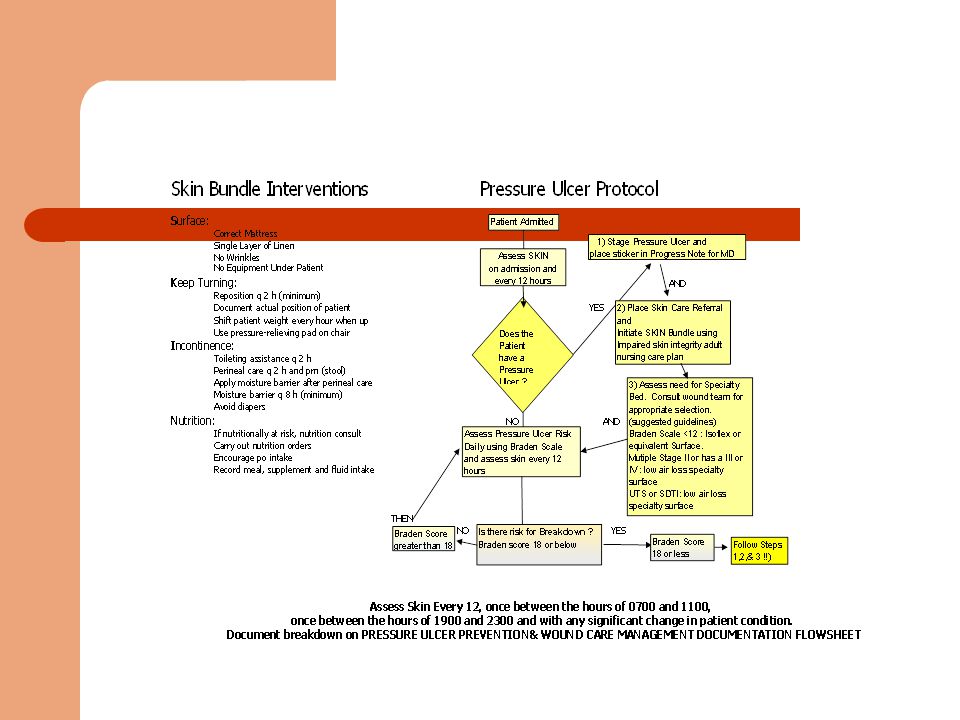
S-K-I-N Bundle Interventions S URFACE K EEP TURNING I NCONTINENCE MANAGEMENT N UTRITION Correct mattress selection Single layer of linen No wrinkles No equipment or caps under patient Repositioning patient every two hours (minimum) Shift patient weight every hour when in chair Use pressure relieving pad on chair Toileting assistance every two hours Perineal care every two hours and PRN Apply moisture barrier after Perineal care Avoid Diapers If nutritionally at risk, place nutrition consult Carry out Nutrition Orders/Recommendations Encourage PO intake Record meal, supplements and fluid intake
 Shift patient weight every hour when in chair Use pressure relieving pad on chair Toileting assistance every two hours Perineal care every two hours and PRN Apply moisture barrier after Perineal care Avoid Diapers If nutritionally at risk, place nutrition consult Carry out Nutrition Orders/Recommendations Encourage PO intake Record meal, supplements and fluid intake")
8
Implementation: The SKIN bundle has been incorporated into the Impaired Skin Integrity Care Plan/Adult CC_#15 Implement this care plan when your patient has a Braden score of 18 or below

10
Position changes Remember to document position changes on page 3 of the Adult Patient Plan of care record Reposition patient every 2 hours while in bed and every 1 hour while in chair Document Sf for self if patient is able to reposition themselves without assistance. Place a checkmark ( ) if you reposition the patient. Write initials of healthcare personnel completing this section at the bottom *You no longer have to document left, back, right etc. Please cross out all options except self until the Master code sheet can be revised.
 if you reposition the patient. Write initials of healthcare personnel completing this section at the bottom *You no longer have to document left, back, right etc. Please cross out all options except self until the Master code sheet can be revised..")
11
Documentation Updates Due to feedback from many staff nurses the Wound and Skin documentation has been removed from the Adult Patient Plan of Care Record. A NEW 4 day form has been created for Wound and Skin documentation so see trends in risk, healing or worsening of wounds

12
Documentation Updates The new form is called: “PRESSURE ULCER PREVENTION WOUND CARE MANAGEMENT DOCUMENTATION FLOWSHEET” As with any documentation, all entries should be dated, timed and signed or initialed

13
Braden Scale Important!!

14
Documentation Updates The Braden Scale is done on admission and then once daily, evaluating: Sensory Perception Moisture Activity Mobility Nutrition Friction and Shear

15
Documentation Updates A patient is at risk to develop pressure ulcers if their Braden score is 18 or below A number is filled in for each score and totaled If the patient’s Braden score is 18 or below, implement the Standard Care Plan cc_#15 Impaired Skin integrity SKIN Bundle

16
Documentation Updates A complete head to toe assessment and evaluation of the patient’s skin should be completed and documented: 1. On admission 2. Every 12 hours once between the hours of 0700 and 1100 hrs., and once between the hours of 1900 and 2300 hrs. 3. And with any significant change in patients condition, (example, after surgery or transfer to critical care)
.")
17
Documentation every 12 hours You must complete this section of the flow sheet every 12 hours, once between 0700-1100 hrs. and once between 1900-2300 hrs. – see sample above. IntactNo standardNA JJ Skin intact

18
Documentation Updates Assessment and Evaluation includes: Evaluation: Intact or Not intact Pressure Ulcer Present: Yes or No Physician notified of new or worsening pressure ulcer: Yes, no, or NA (MD should be notified using the Orange Pressure Ulcer alert sticker) Pressure Ulcer
 Pressure Ulcer")
19
Documentation Updates Assessment and Evaluation continued: Pressure ulcer protocol in place Bed/Mattress type Referrals sent (Skin team and Nutrition) Outcome
 Outcome")
20
Documentation Updates If a a patient’s skin is NOT INTACT at the time of the skin evaluation an entry needs to be made on page 2 in the Pressure Ulcer/Surgical Wound Description section

21
Documentation Updates Enter the Pressure ulcer/Wound site number and letter (L=Left and R=Right) using the pre-numbered body part site Example: Right heel = R13
 using the pre-numbered body part site Example: Right heel = R13")
22
Documentation Updates: For Surgical and other wounds, number the body starting with #15 and document corresponding location on the form L5 Left shoulder incision=L5

23
Documentation Updates Document the wound type: P= Pressure ulcer SU = Surgical wound ST= Skin tear PT= Partial thickness wound FT= Full thickness wound *Remember Pressure ulcers are staged, other wounds are not. Venous and arterial wounds are identified as partial thickness or full thickness

24
Documentation Updates Enter the stage of the pressure ulcer if it is one. Measure the Pressure Ulcer or wound minimally on admission and weekly on Wednesday, including length, depth and width

25
Documentation Updates Document wound appearance: G-Granulation S-Slough N-Necrotic D-Discoloration E-Ecchymotic Example of SLOUGH

26
Documentation Updates Document exudate consistency: Ser-serous Ss-Sero-sanguinous S-Sanguinous P-Purulent B-Billiary F-Fecal

27
Documentation Updates Document exudate amount and type Document if odor is present Document appearance of surrounding skin: ER-Erythema M-Macerated ED-Edematous

28
Documentation Updates Document if any tunneling or undermining is present. As with any documentation, all entries should be dated, timed and signed or initialed Amount of undermining

29
Documentation Updates ** Until the 6 page flow sheet (Adult patient Plan of Care Record) is revised: Cross out the Wound and Skin section on the TOP page 5, and Refer to Wound and Pressure ulcer worksheet.****
 is revised: Cross out the Wound and Skin section on the TOP page 5, and Refer to Wound and Pressure ulcer worksheet.****")
30
Flow Chart The Flow chart on the next slide will be available in bedside books as a reference describing the steps when implementing the SKIN bundle The slides following the flow chart will breakdown the process more slowly

32
Skin assessment is done: A skin assessment takes place on admission And every 12 hours once between the hours of 0700 and 1100 hrs., and once between the hours of 1900 and 2300 hrs. And with any significant change in patient condition

33
If NO Pressure ulcer on admission: Braden score is done – on admission, and – daily to assess risk for pressure ulcer development

34
Patient at risk (Braden score 18 or less) If the patient is at risk for pressure ulcer development at any time during admission, (Braden score 18 or below) Implement the SKIN bundle using the Impaired Skin Integrity (Care Plan cc_#15)
 If the patient is at risk for pressure ulcer development at any time during admission, (Braden score 18 or below) Implement the SKIN bundle using the Impaired Skin Integrity (Care Plan cc_#15)")
35
Pressure Ulcer Present on Admission If the patient has a pressure ulcer on admission or at the time of any assessment Implement the SKIN bundle using the Impaired Skin Integrity Care Plan/Adult (cc_#15)
")
36
Pressure Ulcer is present Stage the pressure ulcer Place an orange sticker in the Progress Notes to alert the MD of the pressure ulcer Notify the Skin Team by entering a referral in the Powerchart Pressure Ulcer PROGRESS NOTE

37
Skin Team Location contact information Millard Fillmore Gates Circle Hospital Phone:887-4925 Buffalo General Hospital Phone:859-2222 Millard Fillmore Suburban Hospital Phone:568-6787 DeGraff Memorial Hospital Phone:690-2008 Waterfront Health Care Center Phone:847-2500

38
Pressure Ulcer Training SKIN & NDNQI Did you know Kaleida Health is participating in a National Database of Nursing Quality Indicators? Kaleida Health is providing information based on our skin care findings. Log on to http://www.nursingquality.org/http://www.nursingquality.org/ You can obtain free PRESSURE ULCER TRAINING on staging pressure ulcers, differentiating arterial ulcers, venous ulcers, & other wound types. This will give you 1.5 CE credits.

39
Documentation reminders Skin assessment and evaluation: On admission, every 12 hours (once between the hours of 0700 and 1100 and once between the hours of 1900 and 2300) and with any significant change in patient condition. Measurement of Pressure Ulcer Documented in Chart on Admission and every Wednesday A STARS Report needs to be filled out when a patient is admitted with or acquires a Pressure ulcer during hospitalization Nutrition and Skin referrals in computer Pressure Ulcer Sticker in Progress notes Pressure Ulcer Protocol in place (cc_#15) Braden Scale score Documented daily
 Braden Scale score Documented daily.")
Similar presentations


, then Skin Color.>")




.>")




: Baseline incidence rate - 4.5% Nutritional assessment - 50% Pressure.>")







