Download presentation
Presentation is loading. Please wait.

1
DRUG POLICY OF THE EUROPEAN UNION SIVIGLIA 15 May 2007 SILVIO GARATTINI

2
BIAS IN CLINICAL TRIALS EUROPEAN LEGISLATION

3
Institutional location Industry, consumers or public health?

5
Quality, efficacy, safety Necessary, not always sufficient

6
IS JUSTIFIED? MINORITY POSITION REASONS FOR WITHDRAWAL RESULTS OF COMMITTMENTS CONFIDENTIALITY

7
ADDED VALUE TOO MANY TRIALS USE PLACEBO OR NO-CONTROLS

8
ADDED VALUE TOO MANY TRIALS USE PLACEBO OR NO-CONTROLS WHEN COMPARISONS ARE MADE DESIGNS OF EQUIVALENCE OR NON INFERIORITY ARE

9
ADDED VALUE TOO MANY TRIALS USE PLACEBO OR NO-CONTROLS WHEN COMPARISONS ARE MADE DESIGNS OF EQUIVALENCE OR NON INFERIORITY ARE SELECTION OF COMPARATOR IS FREQUENTLY INADEQUATE

10
ADDED VALUE TOO MANY TRIALS USE PLACEBO OR NO-CONTROLS WHEN COMPARISONS ARE MADE DESIGNS OF EQUIVALENCE OR NON INFERIORITY ARE SELECTION OF COMPARATOR IS FREQUENTLY INADEQUATE FOCUS ON SELECTED ADVERSE REACTIONS

11
ADDED VALUE TOO MANY TRIALS USE PLACEBO OR NO-CONTROLS WHEN COMPARISONS ARE MADE DESIGNS OF EQUIVALENCE OR NON INFERIORITY ARE SELECTION OF COMPARATOR IS FREQUENTLY INADEQUATE FOCUS ON SELECTED ADVERSE REACTIONS SMALL ADVANTAGES FOR NIGH PRICES

13
18ANTICANCER AGENTS 21INDICATIONS 12ONLY PHASE II 9PHASE III 6EQUIVALENCE OR NON INFERIORITY 3SUPERIORITY

14
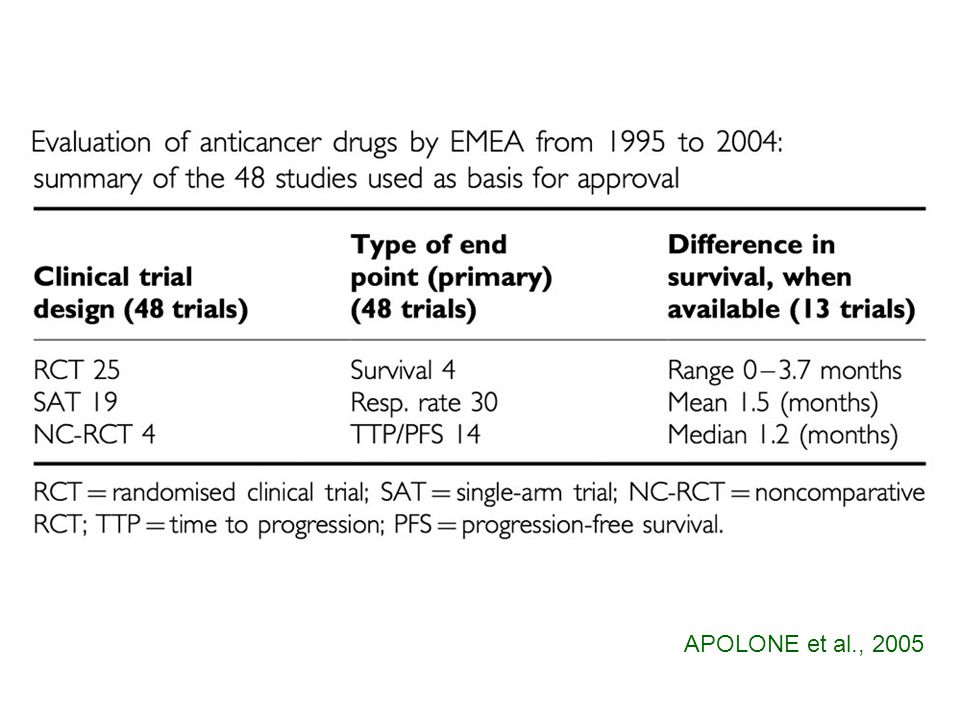
APOLONE et al., 2005

17
EQUIVALENCE

19
OUT OF 383 CLINICAL TRIALS 64 % COULD DETECT A DIFFERENCE > 50 % 84 % COULD DETECT A DIFFERENCE > 25 % MOHER et al., 1994

20
BIOTECH SUBSTANCES APPROVED IN 1995-2003 65 61 (15 ) WITH RCT 46 (11) WITH ACTIVE COMPARATOR 30 (5) SUPERIORITY 13 (4) WITH HARD ENDPOINTS 8 (4) 2 (2) EQUIVALENCE/ NON-INFERIORITY 17 (1) PLACEBO CONTROLLED 16 (5) WITHOUT DOSE-FINDING 33 (8) UNDER EXCEPTIONAL CIRCUMSTANCES 10 (6) DIAGNOSTICS 4 algasidase beta, basilkiximab, infliximab, interferon beta-1b, laronidase eptotermin alfa becaplermin, desirudin, rasburicase, trastuzumab, eptotermin alfa becaplermin, desirudin, rasburicase, trastuzumab becaplermin,desirudin alemtuzumab, beclapermin, eptotermin alpha, human protein C, interferon beta Ib, laronidase, rituximab, trastuzumab basiliximab, becaplermin, desirudin, infliximab
 WITH RCT 46 (11) WITH ACTIVE COMPARATOR 30 (5) SUPERIORITY 13 (4) WITH HARD ENDPOINTS 8 (4) 2 (2) EQUIVALENCE/ NON-INFERIORITY 17 (1) PLACEBO CONTROLLED 16 (5) WITHOUT DOSE-FINDING 33 (8) UNDER EXCEPTIONAL CIRCUMSTANCES 10 (6) DIAGNOSTICS 4 algasidase beta, basilkiximab, infliximab, interferon beta-1b, laronidase eptotermin alfa becaplermin, desirudin, rasburicase, trastuzumab, eptotermin alfa becaplermin, desirudin, rasburicase, trastuzumab becaplermin,desirudin alemtuzumab, beclapermin, eptotermin alpha, human protein C, interferon beta Ib, laronidase, rituximab, trastuzumab basiliximab, becaplermin, desirudin, infliximab")
21
ACUTE RENAL REJECTIONS ARE MINIMIZED WHEN TROUGH LEVELS ARE KEPT BETWEEN 330 - 430 ng/ml MARGREITER et al., 2002 TRIAL CYCLOSPORINE < 300 ng/ml TACROLIMUS VS CYCLOSPORINE 32.5 %51.3 % ACUTE REJECTIONS

22
Rabinowitz et al., 2001

23
Favours atypical Favours haloperidol Drop out rates by dose of comparator drug in trials of patients with schizophrenia or related disorders (risk difference and 95 % confidence intervals) Geddes et al., 2000 ≤ 12 mg haloperidol > 12 mg haloperidol -0.5-0.4-0.3-0.2-0.100.1
 Geddes et al., 2000 ≤ 12 mg haloperidol > 12 mg haloperidol")
24
ATYPICAL ANTIPSYCHOTICS THE REDUCED EFFECT ON EPS IS THE FOCUS OF ADVERTISEMENT WEIGHT GAIN AND PROPENSITY TO DIABETES ?

25
NEUROLOGIC EFFECTS14%17%0 WEIGHT GAIN30%12%0 BLOOD GLUCOSE (CHANGE)15 ± 205.2 ± 200 GLYCOSYLATED Mb00.4 ± 0.090.1 ± 0.06 CHOLESTEROL (CHANGE)9.7 ± 2.20.5 ± 2.30 TRIGLYCERIDES (CHANGE)42 ± 88 ± 11 OLANZAPINE vs PERPHENAZINE PARAMETER CATIE, 2005
15 ± ± 200 GLYCOSYLATED Mb00.4 ± ± 0.06 CHOLESTEROL (CHANGE)9.7 ± ± 2.30 TRIGLYCERIDES (CHANGE)42 ± 88 ± 11 OLANZAPINE vs PERPHENAZINE PARAMETER CATIE, 2005")
26
IF 4 MILLIONS SCHIZOPHRENIC PEOPLE WERE TREATED WITH ANTIPSYCHOTIC AGENTS CONFERRING A MEAN WEIGHT GAIN OF 4 Kg OVER A PERIOD OF 10 YEARS IN COMPARISON WITH A DRUG WITH LITTLE EFFECT ON BODY WEIGHT ADDITIONAL 24,560 DEATHS ADDITIONAL 92,720 CASES OF IMPAIRED GLUCOSE TOLERANCE ADDITIONAL 120,760 CASES OF HYPERTENSION FONTAINE et al., 2001

27
Vigor Study Group. N Engl J Med 2000 Cumulative Incidence of the Primary End Point of a Confirmed Upper Gastrointestinal Event among All Randomized Patients.

28
Time to cardiovascular adverse events in the VIGOR trial Mukherjee et al, JAMA, 2001

29
Risk of cardiovascular events and rofecoxib: cumulative meta-analysis. Peter Jüni et al, Lancet 2004 Cumulative meta-analysis of randomised trials comparing rofecoxib with control

30
Rofecoxib at the time of marketing approval (1999): safety data based on 5,000 patients at the time of withdrawal (2004): given daily to 2,000,000 patients (sales in 2003 US $ 2.5 billion) For newly licensed drugs, confidence about safety can only be provisional
: safety data based on 5,000 patients at the time of withdrawal (2004): given daily to 2,000,000 patients (sales in 2003 US $ 2.5 billion) For newly licensed drugs, confidence about safety can only be provisional")
31
CARDIOVASCULAR TOXICITY DICLOFENAC1 COXIBs0.92 * (0.81-1.05) * 26 RCT Psaty and Weiss, 2007
 * 26 RCT Psaty and Weiss, 2007")
32
CARDIOVASCULAR TOXICITY NAPROXEN1 COXIBs1.57 * (1.21-2.03) * 42 RCT Psaty and Weiss, 2007
 * 42 RCT Psaty and Weiss, 2007")
33
BEVACIZUMAB RECOMBINANT HUMANISED MONOCLONAL lgG1 ANTIBODY IS AN INHIBITOR OF h VEGF (ANGIOGENESIS). LICENSED IN COMBINATION WITH i.v. 5Fu/FA + IRINOTECAN FOR FIRST-LINE TREATMENT OF METASTATIC COLORECTAL CARCINOMA. DOSE: 5 mg/kg i.v. ONCE EVERY 14 days 100 mg0306.76 € 400 mg1224.55 € TOTAL COURSE AVERAGE 18.2 DOSES = 21,285.9 €

34
BEVACIZUMAB OUTCOME+FU/FA+FU/FA +BEVACIZUMAB MEDIAN OVERALL SURVIVAL n = 20913.2 mo.16.6 mo. NS n = 07113.6 mo.17.7 mo. NS PROGRESSION FREE SURVIVAL n = 2095.5 mo.9.2 mo. S n = 0715.2 mo.9.0 mo. S TUMOR RESPONSE RATE n = 20915.2 %25.2 % S n = 07116.7 %40.0 % NS METASTATIC COLORECTAL CARCINOMA

35
BEVACIZUMAB OUTCOMEIFLIFL- BEVACIZUMAB MEDIAN OVERALL SURVIVAL 15.6 mo.20.3 mo. n=8P3 PROGRESSION FREE SURVIVAL06.2 mo.10.6 mo. TUMOR RESPONSE RATE34.8 %44.8 % METASTATIC COLORECTAL CANCER

36
BEVACIZUMAB TREATMENTGRADE 3-4GRADE 3-4 ADVERSE REACTIONSHYPERTENSION IFL74.0 %02.3 % IFL+BEVACIZUMAB84.9 %11.0 % 5FU/FA71.0 %03.0 % 5FU/FA+BEVACIZUMAB87.0 %16.0 %

37
Paclitaxel-Carboplatin Alone or with Bevacizumab for Non-Small-Cell Lung Cancer Sandler et al. N Engl J Med 2006;355:2542-50 Conclusions The addition of bevacizumab to paclitaxel plus carboplatin in the treatment of selected patients with non-small-cell lung cancer has a significant survival benefit with the risk of increased treatment-related deaths. (ClinicalTrials.gov number, NCT00021060.)
.")
38
Script 23 April 2007

39
PACLITAXEL-CARBOPLATIN ± BEVACIZUMAB Sandler et al., NEJM 2006, 355, 2542 SURVIVAL BENEFIT 12 Pts MUST BE TREATED TO HAVE 1 MORE SURVIVAL AT 1 YEAR AT THE PRICE OF 1 TOXIC DEATH EVERY 24 PATIENTS TREATED MEDIAN OVERALL SURVIVAL 12.3 mo. vs 10.3 mo.

40
BEVACIZUMAB INCREASE OF SALES BY 76% IN 2006 vs 2005 WITH A TOTAL OF 2.4 Billion $ SCRIPT, 29 th March 2007

41
CETUXIMAB RECOMBINANT MONOCLONAL ANTIBODY THAT BLOKS EGFR LICENSED IN COMBINATION WITH IRINOTECAN FOR PATIENTS EXPRESSING EGFR IN METASTATIC COLORECTAL CANCER AFTER FAILURE OF CYTOTOXIC THERAPY THAT INCLUDED IRINOTECAN DOSE: 400 mg/m 2 i.v. (700 mg) FOLLOWED BY 250 mg/m 2 (430mg) weekly 100 mg189.05 € 1,323 € (LOADING DOSE) 842,9 (MAINTENANCE DOSE) TOTAL COURSE AVERAGE 16.8 DOSES = 13,117.8 €
 FOLLOWED BY 250 mg/m 2 (430mg) weekly 100 mg € 1,323 € (LOADING DOSE) 842,9 (MAINTENANCE DOSE) TOTAL COURSE AVERAGE 16.8 DOSES = 13,117.8 €.")
42
CETUXIMAB OUTCOMECETUXIMAB CETUXIMAB + IRONOTECAN MEDIAN OVERALL SURVIVAL n= 3296.9 mo.8.5 mo. n= 3476.6 mo.- n= 0576.4 mo.- n= 138-8.4 mo. METASTATIC COLORECTAL CANCER NS

43
SECOND-LINE TREATMENTIRINOTECANIRINOTECAN + CETUXIMAB OVERALL RESPONSE RATE (%)2.604.0 DISEASE CONTROL (%)4.216.4 MEDIAN PROGRESSION-FREE (MO)2.604.0 OVERALL SURVIVAL (MO)9.910.7 n=1300 patients with colorectal cancer failing first-line oxaliplatin-based therapy EPIC, 2007
 DISEASE CONTROL (%) MEDIAN PROGRESSION-FREE (MO) OVERALL SURVIVAL (MO) n=1300 patients with colorectal cancer failing first-line oxaliplatin-based therapy EPIC, 2007")
44
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Final Appraisal Determination Bevacizumab and cetuximab for metastatic colorectal Cancer Bevacizumab in combination with 5-fluorouracil plus folinic acid, with or without irinotecan, is not recommended for the first-line treatment of metastatic colorectal cancer. Cetuximab in combination with irinotecan is not recommended for the secondline or subsequent treatment of metastatic colorectal cancer.

45
THERE IS A NEED FOR MORE INDEPENDENT CLINICAL RESEARCH AT LEAST ONE PHASE 3 STUDY FOR DRUG APPROVAL SHOULD BE PERFORMED BY A NON-PROFIT INSTITUTION HEAD TO HEAD COMPARISON OF SINGLE DRUGS OR STRATEGIES

46
THE ROLE OF AIFA 54 PROJECTS APPROVED AND FINANCED IN 2006 (35 M €) 51 PROJECTS APPROVED IN 2007
 51 PROJECTS APPROVED IN 2007")
47
EXAMPLES OF APPROVED PROJECTS A prospective study on long-term outcome and potential usefulness of an intervention aimed at reducing adverse effects in patients with refractory epilepsy. Evaluation of prescribing pattern and safety profile of antidepressant and antipsychotic medications in italian general practice. Pharmacist’s outreach visits and new information formats: cluster and single-doctor randomised controlled trials for evaluating their feasibility and impact on knowledge, attitudes and prescribing practices of general practitioners in three italian regions.

48
EXAMPLES OF APPROVED PROJECTS A randomized, placebo-controlled study of the efficacy of low-dose aspirin in the prevention of cardiovascular events in subjects with diabetes mellitus treated with statins. A randomized prospective, multicenter trial to compare the effect on chronic allograft nephropathy of mycophenolate mofetil versus azathioprine as the sole immunosuppressive therapy for kidney transplant recipients. A randomized, controlled trial to evaluate the efficacy of low-molecular-weight heparin on pregnancy outcome of women with previous pregnancy complications.

49
EXAMPLES OF APPROVED PROJECTS First adjuvant trial on all aromates inhibitors in early breast cancer. A phase 3 study comparing anastrozolo, letrozole and exemestane, upfront or sequentially. A randomized clinical trial of trastuzumab optimization in patients with locally advanced and/or metastatic breast cancer overexpressing her 2 after a first-line chemotherapy plus trastuzumab. Multicenter randomized controlled study of azathioprine versus interferon beta in relapsing-remitting multiple sclerosis.

Similar presentations





 versus FOLFOX4 in Patients with Advanced Colorectal Carcinoma Previously Treated.>")

:>")

 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")



 Scientific Achievements.>")


 Treated with Anti Vascular Endothelial Growth Factor (VEGF)>")



>")

 with Newly Diagnosed Multiple Myeloma (NDMM) Receiving Lenalidomide and Low-Dose Dexamethasone.>")
: investigational agents TTP = median time to disease progression OS = median overall survival.>")