Download presentation
1
Control of Scatter Radiation Beam Restricting Devices
By Prof. Stelmark

2
PRODUCTION OF SCATTER RADIATION
Two types of x-rays are responsible for the optical density and contrast on a radiograph: those that pass through the patient without interacting, and those that are scattered within the patient through Compton interaction. X-rays that exit from the patient are remnant x-rays and those that exit and interact with the image receptor are called image-forming x-rays

3
Proper collimation of the x-ray beam has the primary effect of reducing patient dose by restricting the volume of irradiated tissue. Proper collimation also improves image contrast. Ideally, only those x-rays that do not interact with the patient should reach the image receptor.

4
As scatter radiation increases, the radiograph loses contrast and appears gray and dull. Three primary factors influence the relative intensity of scatter radiation that reaches the image receptor: kVp Field size Patient thickness

5
kVp As x-ray energy is increased, the absolute number of Compton interactions decreases, but the number of photoelectric interactions decreases much more rapidly. Therefore, the relative number of x-rays that undergo Compton interaction increases.

6
Approximately 1% of x-rays incident on the patient reach the image receptor.

7
Field Size Another factor that affects the level of scatter radiation and is controlled by the radiologic technologist is x-ray beam field size. As field size is increased, scatter radiation also increases

10
Extremity radiographs appear sharp because of less tissue and, hence, less scatter radiation.

11
Beam Restrictors Basically, three types of beam-restricting devices are used: The aperture diaphragm Cones or cylinders The variable-aperture collimator

13
Aperture diaphragm is a fixed lead opening designed for a fixed image receptor size and constant source-to-image receptor distance

15
The most familiar clinical example of aperture diaphragms may be radiographic imaging systems for trauma. The typical trauma system has a fixed source-to-image receptor distance (SID) and is equipped with diaphragms designed to accommodate film sizes of 13×18 cm, 20×25 cm, and 25×30 cm. Radiographic imaging systems for trauma can be positioned to image all parts of the body
 and is equipped with diaphragms designed to accommodate film sizes of 13×18 cm, 20×25 cm, and 25×30 cm. Radiographic imaging systems for trauma can be positioned to image all parts of the body.")
16
Cones and cylinders are shaped differently, but they have many of the same attributes. A cone or cylinder is essentially an aperture diaphragm that has an extended flange attached to it. The flange can vary in length and can be shaped as either a cone or a cylinder. The flange can also be made to telescope, thereby increasing its total length . Like aperture diaphragms, cones and cylinders are easy to use. They slide onto the tube directly below the window

17
Cones and cylinders limit unsharpness surrounding the radiographic image more than aperture diaphragms do, with cylinders accomplishing this task slightly better than cones. However, they are limited in terms of the sizes that are available, and they are not necessarily interchangeable among tube housings

20
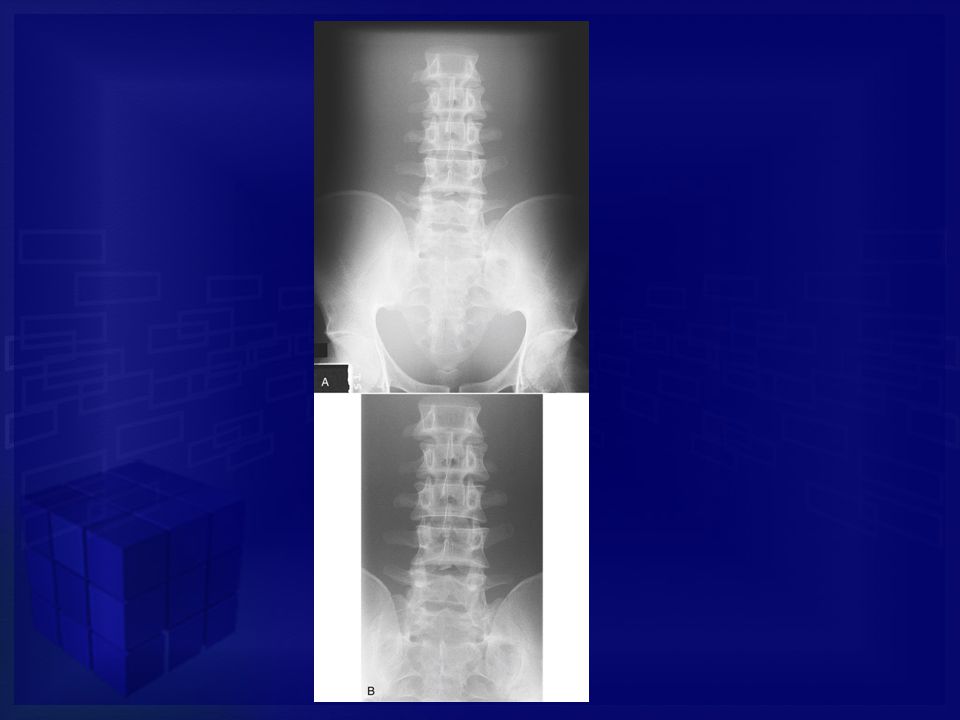
Images with and without a Cylinder
Images with and without a Cylinder. Radiograph of the frontal and maxillary sinuses. A, Not using a cylinder. B, Using a cylinder.

21
Variable Aperture Collimator
The light-localizing variable-aperture collimator is the most commonly used beam-restricting device in radiography.

22
Increased Factor Result Collimation Patient dose decreases. Scatter radiation decreases. Radiographic contrast increases. Film-screen: Radiographic density decreases. Digital: Quantum noise increases. Field Size Patient dose increases. Scatter radiation increases. Radiographic contrast decreases. Film-screen: Radiographic density increases. Digital: Quantum noise decreases.

23
Patient Thickness Imaging thick parts of the body results in more scatter radiation than imaging thin parts does. Compare a radiograph of the bony structures in an extremity with a radiograph of the bony structures of the chest or pelvis. Even when the two are taken with the same screen-film combination, the extremity radiograph will be much sharper because of the reduced amount of scatter radiation

25
Normally, patient thickness is not controlled by the radiologic technologist. If you recognize that more x-rays are scattered with increasing patient thickness, you can produce a high-quality radiograph by choosing the proper technique factors, and by using devices that reduce scatter radiation to the image receptor, such as a compression paddle











![[Radiography] Technique - Exposure Factors](/5/1525033/big_thumb.jpg "[Radiography] Technique - Exposure Factors>")











>")





